Case study 97.1
A 56-year-old white male with no past medical history presents to his primary care physician for his yearly physical. His exam and laboratory results are all negative with the exception of an elevated prostate serum antigen (PSA) level at 8 ng/mL (normal <4 ng/mL). Prostate biopsy is scheduled.
1. In an asymptomatic patient with a normal digital rectal exam, should PSA screening be standard?
- Yes
- No
- It depends
Since the introduction of the PSA test for early detection of prostate cancer in 1987, its use has steadily increased with an estimated 47–58% of all new prostate cancers being screen-detected in 2000. This, in turn, has led to an increased incidence with a corresponding decreased proportion of metastatic or locally advanced stage disease at diagnosis. The primary goal of PSA-based screening is to find men in whom treatment would reduce morbidity and mortality. Although the risk of prostate cancer varies with the PSA level in the serum, the PSA level is not specific to prostate cancer, and the majority of men with an increased PSA do not have cancer.
However, PSA screening has become controversial recently. The latent prevalence of disease detected by screening, as reported by Draisma et al., is much higher than the incidence in the absence of screening. The possibility of causing harm from overdiagnosis and treatment in patients whose cancer would otherwise have remained latent has many physicians asking if screening is appropriate or even beneficial in some patient populations.
The US Preventive Services Task Force released a recommendation against the use of PSA screening in May 2012, citing several studies that could not demonstrate a benefit in overall or all-cause mortality with routine screening. It argues that the harms associated with screen-detected diagnosis and treatment in men who would have remained asymptomatic are too prevalent, and thus outweigh the benefits of screening.
The American Society of Clinical Oncology (ASCO), however, recommends testing for asymptomatic men with a life expectancy of 10 years or greater. It emphasizes the further findings of the European Randomized Study of Screening for Prostate Cancer (ERSPC), and other studies including the Goteberg trial, which demonstrate a decrease in prostate cancer–related death of 20–44% with the use of screening in men 55–69 years, indicating that in some studies the benefits of screening validate its continued use.
Most recently (March 2014), the National Comprehensive Cancer Network (NCCN) has released a new recommendation to begin PSA screening as early as age 45. The purpose of this revision is to allow for possible future cancer risk stratification. This new recommendation is based on observational studies, including a large study group in Sweden where a PSA test prior to age 50 predicted prostate cancer risk up to 30 years later. The frequency of future testing would be based on risk stratification according to age-specific PSA levels released by the NCCN (0.7 ng/mL for age 40–49 years and 0.9 ng/mL for age 50–59 years), and annual or biannual follow-up for all men with a PSA greater than 1 ng/mL. Additionally, the NCCN released new recommendations for when to stop screening. The panel suggests discontinuing screening at 69, continue screening up to age 74 (allowing for an increase in PSA threshold in men age 70–74), or discontinue screening at age 75 years for patients with a PSA less than 3 ng/mL. The updated guidelines also suggest any patient with a PSA greater than 3 ng/mL should be considered for biopsy.
Although there is no across-the-board right or wrong answer to the debate, many patients will continue to request PSA screening, and physicians will continue to offer it. The use of PSA screening, therefore, should be used at the physician’s discretion, taking into consideration the patient’s clinical information, including age, comorbidities, ethnicity, and family history of prostate cancer.
The patient underwent a 12-core prostate biopsy, and pathology results are adenocarcinoma, Gleason Score 3 + 3 = 6, involving two cores (40% of one and 20% of the second core). After discussing his options with his primary care physician, a decision is made to undertake active surveillance.
2. Does the patient qualify for active surveillance?
- Yes
- No
This is according to the following widely accepted criteria (Epstein):
- Two or fewer cases with cancer and no more than 50% involvement in any one core
- PSA density <0.15%
- Gleason score ≤6 (no Gleason pattern 4 or 5)
- PSA <10 ng/mL
- Clinical stage T1
The aim of active surveillance is to identify low-risk or clinically insignificant prostate cancer that, if untreated, would not pose an immediate threat to the patient. Active surveillance is strict surveillance with the intent to cure when necessary. Unlike watchful waiting, which does not have treatment with intent to cure as an endpoint, the premise of this treatment is based on the ability to determine low-risk disease that may be followed without causing harm. Low-risk disease has been characterized by the D’Amico risk classification and Epstein criteria, which can be summarized as follows: less than one-third of the biopsy cores are positive, with <50% involvement of any one core; PSA density <0.15%; a Gleason score less than or equal to 6; PSA <10 ng/mL; and stage T1 disease. The Epstein criteria are more stringent with no more than two positive cores. Our patient meets these criteria for risk stratification as a low-risk prostate cancer.
The above criteria are predominantly based on biopsy results. Although there has been a trend toward increasing the number of biopsies performed from 6 to 10–12, there is still inherent undersampling of the gland. This could cause an underestimation of disease burden, and, therefore, an improper diagnosis of insignificant prostate cancer. It is for this reason that several published protocols have modified the triggers of the criteria discussed here. Instead of relying entirely on a PSA level, it has been proposed to follow the course of the PSA, and treat if it rises dramatically. The rate of change in the PSA level is the PSA velocity. The current recommendation is that a biopsy should be considered with a PSA velocity greater than 0.35–0.4 ng/mL per year. PSA doubling time as a method to assess the status of prostate carcinoma is also being studied. It is well understood that the median PSA doubling time of nonmetastatic prostate carcinoma is approximately 36 months. A short PSA doubling time has been observed in 7–47% of patients, and it has been postulated that these patients may have carcinoma in an exponential-growth phase resulting in rapidly increasing PSA levels. In contrast, 30% of patients with relatively stable or declining PSA levels likely have carcinoma in a linear phase of growth that could be followed safely without treatment. Additionally, staging re-biopsy prior to the enactment of active surveillance has also been recommended.
There are currently no reported data from randomized trials showing whether patients who undergo active surveillance have better or worse outcomes in comparison to patients who were treated immediately following diagnosis. However, noncomparative cohort studies have shown comparable disease-free and overall survival rates to patients given curative therapy initially. There are side effects and morbidities as a result of any treatment for prostate cancer, even active surveillance. Therefore, treatment options should be discussed with the patient in association with the patient’s risk profile.
The patient’s PSA level continues to increase over the next several years, and a second prostate biopsy is performed. His pathology report now describes a Gleason pattern 4 in one of two involved cores. The patient undergoes radical prostatectomy (RP).
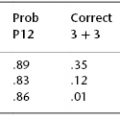
3. Can the patient’s disease-free survival rate be estimated preoperatively?
< div class='tao-gold-member'>
 17: Management of Therapy-Related Myeloid Neoplasms
17: Management of Therapy-Related Myeloid Neoplasms
 36: Nodular Lymphocyte-Predominant Hodgkin Lymphoma
36: Nodular Lymphocyte-Predominant Hodgkin Lymphoma
 11: Minimal Residual Disease in Acute Myeloid Leukemia
11: Minimal Residual Disease in Acute Myeloid Leukemia
 71: Secondary Brain and Spinal Cord Tumors
71: Secondary Brain and Spinal Cord Tumors
 130: Controversies Related to Oncology Clinical Trial Development
130: Controversies Related to Oncology Clinical Trial Development



