4 T1b Glottic Cancer Treated with Transoral Laser Surgery
Abstract
T1b squamous cell carcinoma (SCC) of the glottis can be treated with radiotherapy or transoral laser surgery. Radiotherapy is usually advocated since voice results are considered better compared to transoral laser surgery; nevertheless, the transoral approach is also frequently performed for T1b at the request of the patients. In such cases, special care is needed to avoid unexpected scar. This chapter reports the typical case of a T1b SCC of the glottis with involvement of the anterior commissure observed in a 69-year-old male with a clinical history of daily cigarette smoking for 20 years, and progressive hoarseness lasting for 1 year, who underwent en bloc bilateral subligamental type II cordectomy. The patient, after 3 years of follow-up, is free of cancer. The endoscopic treatment in the form of type II cordectomy was chosen for the following reasons: (1) the surgical strategy has the advantages of a histologically proven resection without residual cancer and, in case of recurrence, a further surgical treatment (including transoral surgery) and also radiotherapy are still available; (2) early cancer of the glottis is associated with a low incidence of occult metastasis and there is no indication for the neck dissection in cN0 patients; (3) the transoral approach allows for treatment of the cancer with minimal complications, low trauma to healthy tissue, and without the need for tracheostomy and/or nasogastric feeding tube; (4) the patient requested to be treated quickly in one stage. In our opinion, transoral CO2 laser microsurgery is an important treatment option in T1b cancer of glottis.
4.1 Clinical Case
The eighth edition of the American Joint Committee on Cancer (AJCC) – TNM classification of laryngeal malignancies defines T1 cancer of the glottis as a cancer limited to the vocal cord(s) that may involve the anterior or posterior commissure with normal mobility; the cancer is classified as T1b when it involves both vocal cords. 1
The role of open partial horizontal laryngectomy (OPHL) for the management of laryngeal squamous cell carcinoma (SCC) has decreased considerably in the last 15 years owing to the development of transoral laser microsurgery and with advances in radiation therapy. 2
Although voice outcomes after transoral laser surgery for T1a cancer have been reported to be extremely favorable with type I to III cordectomies, results after endoscopic treatment for T1b can be worse, especially if the anterior commissure is involved and the resection is performed in one stage.
We report a typical case of a T1b SCC of the glottis with anterior commissure involvement observed in a 69-year-old male.
The patient reported a clinical history of daily cigarette smoking for 20 years, no alcohol intake, and progressive hoarseness during the past year.
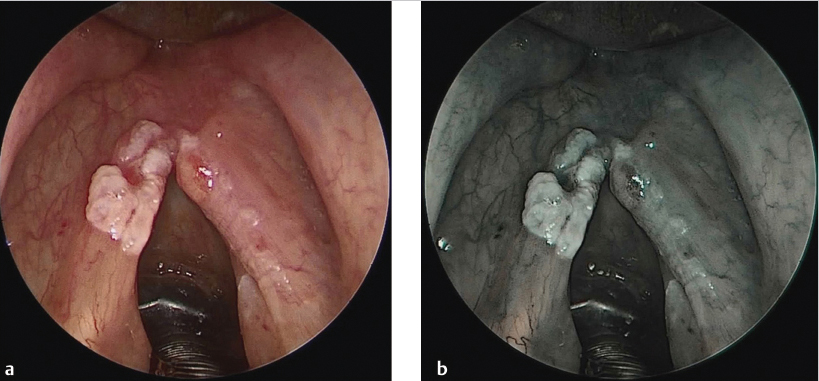
Flexible laryngoscope examination of the larynx revealed a mildly vegetating leukoerythroplastic lesion of the glottis with superficial involvement of the anterior commissure and without impairment of the vocal cord mobility.
Voice analysis showed a voice handicap index (VHI) of 40, the grade, roughness, breathiness, asthenia, and strain (GRBAS) scale showed the following scores: 3, 3, 1, 1, and 2.
During preoperative counseling, the patient expressed his wish to be treated in one stage in the form of an excisional biopsy.
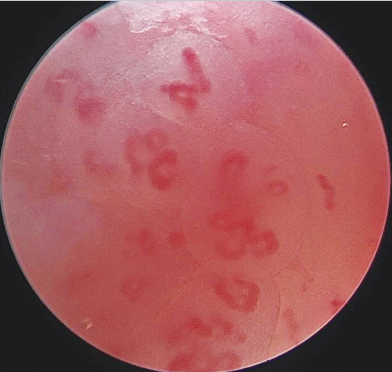
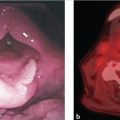
The day of surgery, the patient received ceftriaxone (1,000 mg IV) as antibiotic prophylaxis. The patient was evaluated under general anaesthesia using an endotracheal Mallinckrodt tube (internal diameter of 5.0–7.0 mm; Athlone, Ireland), and using white light and image-enhanced system ( Fig. 4‑1), in order to assess the precise superficial extension of the lesion, to search for synchronous primary cancers, and to identify other precancerous lesions. The endoscopic evaluation was also associated with a contact endoscope performing an image-enhanced contact endoscopy (Image-ECE) that revealed a vascular pattern grade 4 according to the classification of Puxeddu et al 3 ( Fig. 4‑2), highly suspicious for SCC.
Palpation of the lesion showed adherence to the vocal ligament that was confirmed at hydrodissection.
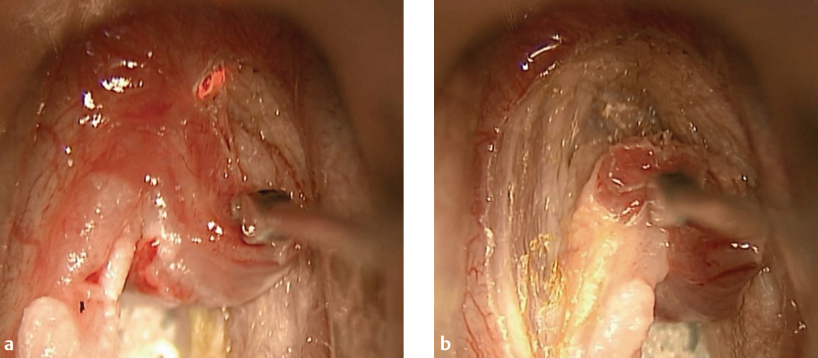
After the intraoperative evaluation, the patient underwent en bloc bilateral subligamental type II cordectomy ( Fig. 4‑3 and Fig. 4‑4), according to the classification of the European Laryngological Society, 4 , 5 in macroscopically healthy tissue. The procedure was performed using Zeiss S21 (Jena, Germany) with 400-mm focal lens coupled with a AcuPulse (Tel Aviv, Israel) CO2 laser with an AcuBlade (Tel Aviv, Israel) focusing system, with which it was possible to obtain a 150μm spot. The superpulsed mode was used at 10 W in continuous wave. This technique allowed a precise dissection with minimal charring with the complete preservation of the vocalis muscle.
The postoperative course was uneventful, and the patient was discharged from the hospital after 2 days. On the 6th and 14th day after surgery, he underwent flexible scope examination under local anaesthesia with removal of the fibrin from the glottis.
Definitive histologic examination revealed a pT1b SCC according to the AJCC–TNM classification 1 resected in free margins of more than 0.5 mm.
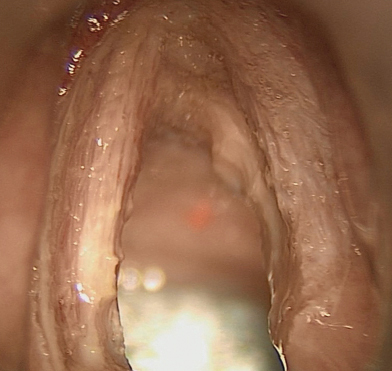
The patient, after 3 years of follow-up, is free of cancer ( Fig. 4‑5). The last voice analysis performed 3 years after surgery showed a VHI of 20, the GRBAS scale showed the following scores: 2, 2, 0, 1, and 1.

Related posts:
 1 T1a Glottic Carcinoma Undergoing Transoral Laser Surgery
1 T1a Glottic Carcinoma Undergoing Transoral Laser Surgery
 8 The Role of Radiation Therapy in Early-Stage Supraglottic Cancer
8 The Role of Radiation Therapy in Early-Stage Supraglottic Cancer
 23 Locally Advanced Supraglottic Cancer: Organ-Preservation Protocol
23 Locally Advanced Supraglottic Cancer: Organ-Preservation Protocol
 20 Locally Advanced Glottic Cancer: Supratracheal Laryngectomy
20 Locally Advanced Glottic Cancer: Supratracheal Laryngectomy
 16 Locally Intermediate Supraglottic Cancer: Radiotherapy
16 Locally Intermediate Supraglottic Cancer: Radiotherapy
 15 Locally Advanced Supraglottic Cancer: Larynx Preservation by Transoral Laser Microsurgery
15 Locally Advanced Supraglottic Cancer: Larynx Preservation by Transoral Laser Microsurgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


