32 Early Primary Tumor with Advanced Neck Disease
Abstract
Advanced metastases to the cervical lymph nodes from a small primary cancer is an uncommon pattern of disease in squamous cell carcinoma of the larynx with unique treatment considerations. This pattern is seen more commonly with a supraglottic than a glottic primary cancer, and almost all such patients have a significant smoking history. In accordance with the National Comprehensive Cancer Network (NCCN) guidelines, treatment decisions should be based on the extent of the primary cancer, expected functional outcomes, and patient preferences. Treatment options include surgery to the primary and neck, followed by directed adjuvant therapy, primary concurrent chemoradiation, or chemoselection (neoadjuvant chemotherapy), followed by concurrent chemoradiation for responders and surgery for nonresponders. Oncologic outcomes are similar with all three treatment options. While primary surgical treatment paradigms provide more accurate staging and prognostic information, advanced nodal disease may preclude a modality-sparing approach and all patients will likely still require radiation with or without chemotherapy. As such, functional outcomes may be better in patients treated with concurrent chemoradiation or chemoselection which are the preferred treatment in this patient population. Close monitoring of the neck is important to ensure treatment response, with salvage neck dissection indicated for persistent metastatic cancer in the neck.
32.1 Introduction
Squamous cell carcinoma of the larynx (LSCC) represents a common subsite of head and neck cancers, and unfortunately has not seen improvement in survival over the past 40 years. 1 The majority of patients who present with cancer of the larynx are male, have a significant history of smoking cigarettes and alcohol, and have advanced cancer at the time of diagnosis. 1 , 2 , 3 Staging of LSCC is based on the eighth edition of the American Joint Commission on Cancer TNM (tumor size, node involvement, and metastasis status) staging system. 4 Advanced stage is defined as patients who have advanced T classification (T3–T4) or N classification (N1–N3) and requires multimodality therapy for the best chance of cure.
Patients who have an early primary cancer with advanced cervical lymph node metastases are stage III/IV, and are particularly interesting, because the larynx is typically quite functional because the cancer is low volume and has not invaded in the vital laryngeal structures. The primary cancer is, therefore, amenable to organ-preservation therapies, including partial laryngectomy or radiation paradigms. In this chapter, we present a clinical case and discuss the presentation, evaluation, and treatment options in patients with an early primary cancer and advanced metastases to the neck.
32.2 Case Example
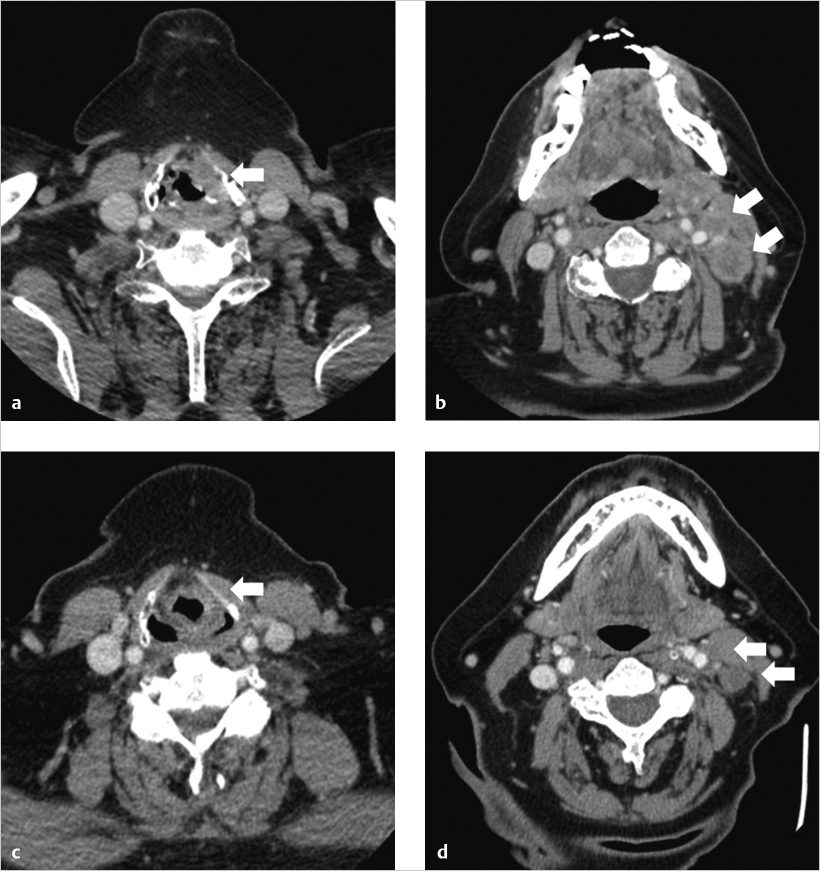
A 55-year-old male with a 25 pack-year history of smoking cigarettes presented with a 3-month history of worsening hoarseness. He reported no dysphagia, odynophagia, or shortness of breath. Examination revealed left palpable cervical lymphadenopathy at the level of the hyoid bone. Flexible laryngoscopy revealed a left glottic mass that extended to the false vocal fold and onto the arytenoid mucosa, without fixation of the vocal cord. A contrast-enhanced CT scan of the neck revealed showed a left glottic lesion extending into the false vocal cord ( Fig. 32‑1 a), without definitive pre-epiglottic or paraglottic space involvement, with pathologic nodes in the left neck at the level of the hyoid bone ( Fig. 32‑1 b). Chest imaging was negative for metastasis. Biopsies obtained in the operating room were positive for squamous cell carcinoma, assessed as T2N2bM0, stage IV disease.
32.3 Presentation Evaluation
Both glottic and supraglottic cancers can present as early primary cancer with advanced metastases to the cervical lymph nodes. Supraglottic cancers are more common than glottic scancers with this presentation given the readily accessible lymphatic system of the pre-epiglottic and paraglottic spaces. Glottic cancers typically do not present with neck disease as patients develop hoarseness early in the course of their disease, but growth of the cancer can involve the laryngeal ventricle and subsequent nodal metastasis does occur. 5
Evaluation of these patients should include a full history and physical examination, supplemented with a fiberoptic examination of the larynx. A thorough assessment of the patient’s overall functional status and pulmonary comorbidities is necessary to evaluate surgical candidacy. Vocal fold mobility, speech and swallowing ability, and airway patency should be documented. Patients with lymphadenopathy at presentation have a higher risk of distant metastasis, and imaging should include the neck as well as the chest to evaluate the extent of disease and/or presence of synchronous malignancy. 6 Biopsies taken in the operating room allow for a close examination of the subsites involved by the primary cancer and can aid in surgical and radiation planning.
32.4 Treatment Options
The treatment options for advanced stage LSCC have evolved, with organ preservation protocols favored when compared to total laryngectomy. 5 , 7 , 8 Patients who present with early primary cancer of the larynx of the glottis and supraglottis may be amenable to organ-preservation surgery, but the advanced nodal stage drives treatment paradigms that require the need for adjuvant radiation with or without chemotherapy. Consistent with the National Comprehensive Cancer Network (NCCN) guidelines, there are three treatment paradigms that are available to patients with early primary laryngeal cancer with advanced lymph node metastasis: surgery followed by directed adjuvant therapy, concurrent chemoradiation, or chemoselection. 9
Related posts:
 1 T1a Glottic Carcinoma Undergoing Transoral Laser Surgery
1 T1a Glottic Carcinoma Undergoing Transoral Laser Surgery
 6 T1b Glottic Cancer, Vertical Partial Laryngectomy
6 T1b Glottic Cancer, Vertical Partial Laryngectomy
 13 Locally Intermediate Glottic Cancer: Supracricoid Laryngectomy with CHEP
13 Locally Intermediate Glottic Cancer: Supracricoid Laryngectomy with CHEP
 18 Locally Advanced Glottic Cancer: Supracricoid Laryngectomy
18 Locally Advanced Glottic Cancer: Supracricoid Laryngectomy
 28 Reconstruction for Advanced Cancer: Pectoralis Major Myocutaneous Flap
28 Reconstruction for Advanced Cancer: Pectoralis Major Myocutaneous Flap
 15 Locally Advanced Supraglottic Cancer: Larynx Preservation by Transoral Laser Microsurgery
15 Locally Advanced Supraglottic Cancer: Larynx Preservation by Transoral Laser Microsurgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


