29 Reconstruction for Advanced Cancer: Supraclavicular Island Flap
Abstract
The supraclavicular island flap (SCIF) is very versatile option for the reconstruction of defects in the head and neck and are used in the reconstruction of skin defects (mainly the lower third of the face, such as the malar, parotid, auricular, and cervical regions), the mucosa (oral cavity, oropharynx, and hypopharynx), and lateral defects, and for skull base repair (especially in the lateral and posterior regions). In this chapter we describe a case of a patient with a recurrent squamous cell carcinoma of the neopharynx following a salvage total laryngectomy that was resected and the circular defect was reconstructed with a SCIF with a very good result. The tips and traps about the flap’s operative technique are described. The SCIF may be harvested rapidly, and it may be used in a single reconstruction procedure with no need to change the patient’s position. The literature also reports that the supraclavicular flap presents similar success rates compared to other flaps and can still be safely used in patients with various comorbidities. The results of our group demonstrate that the average time for flap harvesting was approximately 50 minutes. There were 14.9% of partial flap necrosis (7 of 47 cases). Four cases required surgical debridement and primary closure, and there were three cases of fistula, all of which occurred in the four cases of hypopharyngeal reconstruction that had complete resolution with conservative treatment. All patients exhibited an adequate functional response at the end of 6 months of follow-up after reconstruction.
29.1 Case Report
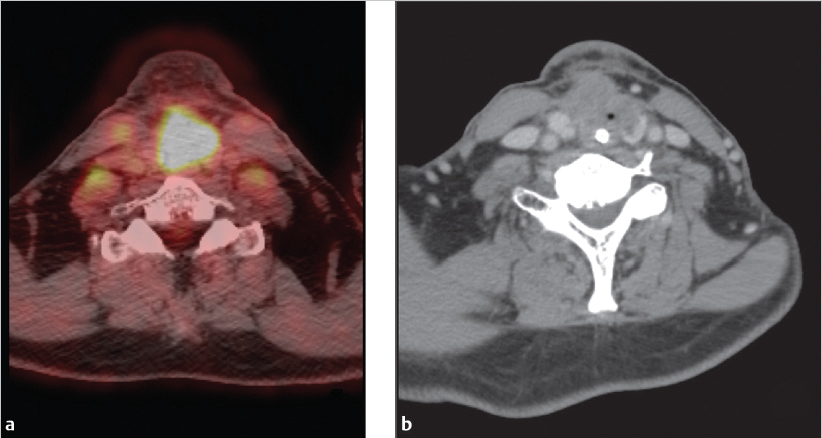
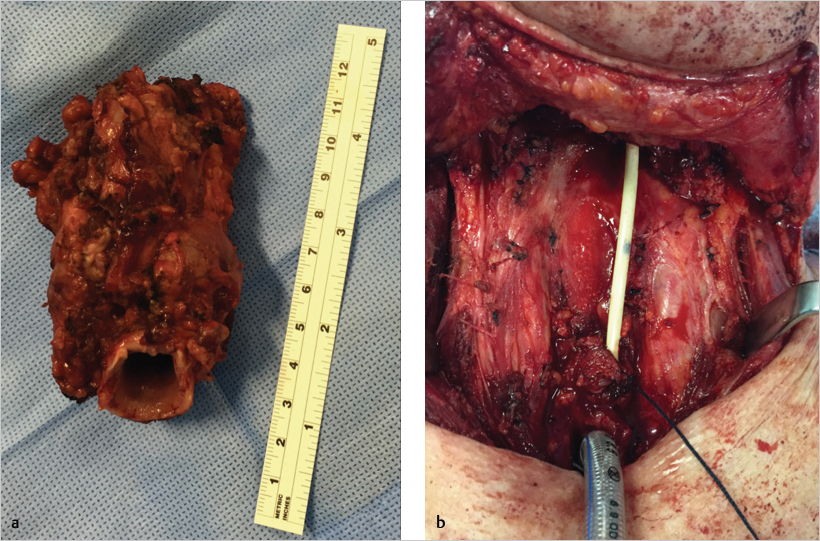
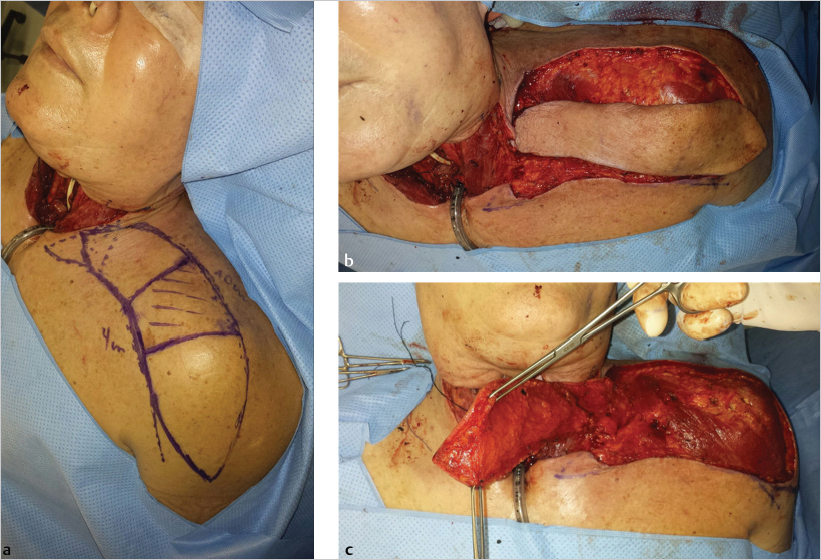
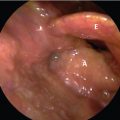
The patient was a 64-year-old Caucasian male patient previously treated with chemoradiotherapy (3 years prior) as an organ preservation protocol for a stage III (T3N0M0) transglottic squamous cell carcinoma (SCC). Two years after this treatment, he presented with a local recurrence and underwent salvage total laryngectomy with primary closure. The histopathological examination revealed a 1.9-cm grade 2 rpT4a (stage IVa) SCC of the left vocal cord with extension to the supraglottis, both piriform sinuses and the thyroid cartilage, with free margins. No adjuvant treatment was performed at that time. The patient presented with another recurrence at the neopharynx ( Fig. 29‑1) and circumferential resection of the pharynx, including two tracheal rings ( Fig. 29‑2) that demonstrated a 7.0-cm grade 2 rpT4a rpN0 (stage IVa) SCC including the pharyngeal mucosa and involving the thyroid gland skin of the anterior neck, esophageal mucosa, and left common carotid artery. A supraclavicular island flap (SCIF) of 8 × 24 cm was used to reconstruct the pharyngeal defect ( Fig. 29‑3 and Fig. 29‑4). The patient stayed in the hospital for 30 days due to complications at the donor site. A cervical hematoma was drained on postoperative day 6, and two resutures were performed to treat donor area dehiscences.

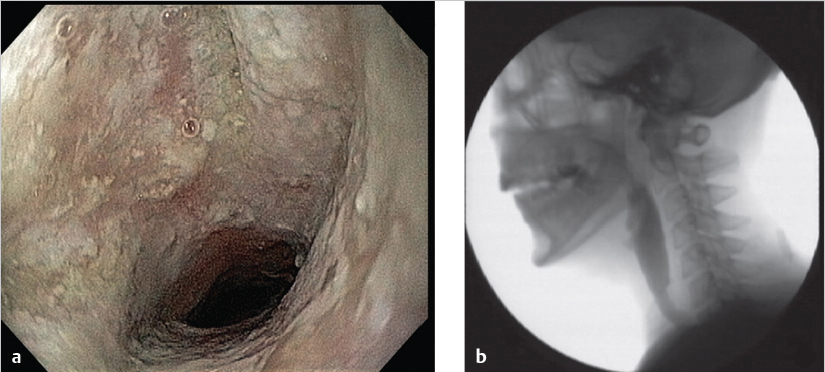
The patient was started on a liquid diet and gradually advanced to a normal diet 45 days after the operation. The feeding tube was removed on the 70th postoperative day. He then received re-irradiation treatment and one cisplatin cycle (the chemotherapy was withdrawn due to nephrotoxicity). The neopharyngeal aspect and the videodeglutogram 6 months after the surgery are displayed in Fig. 29‑5 . Unfortunately, 8 months after the surgery and only 3 months after the end of re-irradiation therapy, a new recurrence was discovered and the patient died 3 months later.
Related posts:
 1 T1a Glottic Carcinoma Undergoing Transoral Laser Surgery
1 T1a Glottic Carcinoma Undergoing Transoral Laser Surgery
 6 T1b Glottic Cancer, Vertical Partial Laryngectomy
6 T1b Glottic Cancer, Vertical Partial Laryngectomy
 13 Locally Intermediate Glottic Cancer: Supracricoid Laryngectomy with CHEP
13 Locally Intermediate Glottic Cancer: Supracricoid Laryngectomy with CHEP
 18 Locally Advanced Glottic Cancer: Supracricoid Laryngectomy
18 Locally Advanced Glottic Cancer: Supracricoid Laryngectomy
 28 Reconstruction for Advanced Cancer: Pectoralis Major Myocutaneous Flap
28 Reconstruction for Advanced Cancer: Pectoralis Major Myocutaneous Flap
 15 Locally Advanced Supraglottic Cancer: Larynx Preservation by Transoral Laser Microsurgery
15 Locally Advanced Supraglottic Cancer: Larynx Preservation by Transoral Laser Microsurgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


