22 Transoral Robotic Surgical Total Laryngectomy: The Technique Step by Step
Abstract
The aim of our study is to demonstrate our technique in performing transoral robotic surgery total laryngectomy (TORS-TL) with the use of the da Vinci robotic system. We provide a comprehensive description of the TORS-TL operative techniques. Two fresh frozen human cadavers were selected after ethical approval to describe the appropriate step-by-step surgical resection. We adopted a five-step procedure that was later applied on two of our patients. The first patient presented initially with a squamous cell carcinoma (SCC) in the laryngeal glottis area. A lack of clinical response to initial treatment by chemoradiotherapy led to the decision of performing salvage total laryngectomy surgery. The second patient had a previous history of head and neck SCC; he had no recurrence of his primary tumor but significantly suffered postoperatively of breathing and swallowing difficulties due to severe laryngeal incompetence. TORS-TL was successfully performed on all cases. The operative time on the two cadavers was approximately 65 and 55 minutes. It was significantly longer on our patients, 210 minutes and 235 minutes, respectively, despite the fact that exactly the same steps were followed throughout all procedures. There were no intraoperative and postoperative complications or surgical morbidity related to the use of the da Vinci robotic system. TORS supraglottic laryngectomy (TORS-SL) for SCC was performed in a safe, reliable, and smooth manner and has shown to be successful in treating our patients. We thus believe our described step-by-step technique for TORS-SL is efficient and reproducible.
22.1 Introduction
Transoral surgery is nowadays a well-established procedure for the management of laryngeal diseases, benign or early malignancies. Transoral robotic surgery (TORS) using the da Vinci System (Intuitive Surgical, Sunnyvale, CA) is described as a minimally invasive surgery providing with excellent outcomes and shortening hospital stays. 1 Different laryngeal subsite surgeries has been addressed by TORS such as supraglottic laryngectomys. Literatur and hypopharyngectomy 3 with feasibility trials and promising initial data. A combination of both procedures is now adapted to perform a TORS total laryngectomy (TORS-TL).
22.2 Patients and Methods
We performed a transoral resection of the entire larynx on two different series. We first operated on two fresh frozen human cadavers in the faculty of medicine anatomy laboratory after ethical approval. Both interventions were performed by the senior author following a predesigned five-step technique. We then operated on live patients in our operative room hospital setting. Both surgeries were also performed by the same surgeon. The da Vinci robotic system was mounted and prepared in the operating room in our usual standard fashion, and we followed exactly the same five-step procedure used during the cadaveric dissection.
Subject selection: The selection of our cadavers was based on the fact that they had to be freshly frozen in order to simulate as closely as possible a real-life situation. A mouth-opening retractor was used to allow exposure and access to the larynx transorally.
The selection of our patients was based on the following criteria: first, both patients should have no general surgical contraindications as confirmed during the preoperative anesthesia consultation. Second, a proper mouth-opening range was required in order to appropriately access the larynges to perform transoral laryngeal resections with a safe margin in case of a tumor.
The first case was a T3N0 glottic cancer that had previously failed an organ preservation strategy based on concomitant chemoradiation therapy. The second case was a patient presenting with a previous history of T3N1 glottic cancer successfully treated by concomitant chemoradiation therapy. A year after treatment, the patient presented to us with a severe laryngeal incompetency, impairing both his breathing and swallowing patterns. Thus, we decided to perform a functional total laryngectomy.
Operative instruments used were found in our regular open neck tracheotomy surgical case.
Regarding the transoral robotic approach, we recommend (according to GL’s learning curve) the use of specific instruments adapted to the da Vinci robot, as well as standard cordectomy instruments and a mouth gag adapted to the surgery: Remacle and Lawson–LARS (Fentex Medical, Neuhausen, Germany) or the FK-WO (Gyrus ACMI, Tuttlingen, Germany).
The five-step procedure is summarized as follows ( Table 22.1 ):
1. Cervical exposure, with tracheostomy and laryngeal dissection ( Fig. 22.1) |
2. Intraoral resection with clipping of the laryngeal artery ( Fig. 22.2) |
3. Larynx delivery through the mouth ( Fig. 22.3) |
4. Intraoral reconstruction by suturing the hypopharyngeal mucosa to the base of tongue ( Fig. 22.4) |
5. Cervical closure by suturing cervical skin to the tracheostomy site (Fig. 22.5) |
Cervical exposure: The procedure begins with a standard tracheostomy skin incision, approximately 4 cm in length, at the midpoint between the cricoid cartilage and the sternal notch. After superior subplatysmal skin flap is raised, the strap muscles are divided along the midline raphe to expose the trachea and cricoid cartilages. A thyroid isthmusectomy is performed, and the lateral lobes are dissected off of the lateral tracheal walls. A complete transection of the trachea is placed at the third tracheal space with rising posterior tracheal mucosal cuts. Inferior stomal stitches are used to secure the thoracic trachea. The skin incision gives ample visualization to dissect around the remaining rostral trachea and cricoid cartilage, which includes sectioning bilateral recurrent laryngeal nerves. At this point, two 2–0 Vicryl sutures are placed around the lateral walls of the rostral trachea and are threaded through glottis for intraoral retraction. The stoma site is covered with sterile drapes.
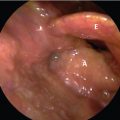
Intraoral resection: The procedure is started with the initial placement of the intraoral retractor with the epiglottis retracted out of view of the glottis. A 0-degree endoscope is used along with 5-mm Maryland dissector and 5-mm spatula Bovie. With optimal retraction and visualization, the initial intraoral incision is placed along the superior aspect of the arytenoid mucosa. With the dissector retracting the mucosa, the Bovie separates the postcricoid mucosa and the medial pyriform sinus wall from the cricoid cartilage. Subsequently, the epiglottis is then released from retraction and the vallecula incision is made along the lingual surface of the epiglottis in a direction toward the superior border of the thyroid cartilage. Extending the vallecular incision laterally and posteriorly, the superior laryngeal vessels are encountered as they course through the thyrohyoid membrane. Multiple clips are placed on the vessels and divided. Dissection is continued caudally until the thyroid cartilage is encountered, keeping the hyoid bone retracted underneath the intraoral retractor blade. The instruments are directed along the external thyroid cartilage perichondrium. As we resume inferiorly, tension will be required on the previously placed inferior tracheal retraction sutures. These sutures will give a rostral pull to the inferior portion of the thyroid cartilage as well as allowing for lateral retraction to improve visualization. Dissection continues caudally and laterally until the larynx is freed from its attachments.
Laryngeal delivery through the mouth: At the end of the dissection, the larynx is delivered orally.
Intraoral reconstruction: The mucosa is reapproximated to the base of tongue with 3–0 braided absorbable sutures placed with the use of the 5-mm needle holder arm. In our experience, given the extensive mucosal preservation, the pharyngotomy can be closed in a horizontal orientation. Following the watertight closure, fibrin glue is placed over the incision. At this point, steps of salivary bypass tube placement and primary tracheoesophageal prosthesis placement may be performed in a typical manner depending on surgeon preference. Intraoral retraction is released.
Cervical closure: With superiorly directed skin retraction, the pharyngotomy may be bolstered with externally placed sutures along the tongue base musculature. The strap muscles are reapproximated over the pharyngotomy site. A small suction drain is placed superior to the stoma site. Superior skin flap is released and the superior stomaplasty is performed using braided absorbable suture. At the end of the procedure, the endotracheal tube is replaced with a laryngectomy tube.
Related posts:
 1 T1a Glottic Carcinoma Undergoing Transoral Laser Surgery
1 T1a Glottic Carcinoma Undergoing Transoral Laser Surgery
 6 T1b Glottic Cancer, Vertical Partial Laryngectomy
6 T1b Glottic Cancer, Vertical Partial Laryngectomy
 13 Locally Intermediate Glottic Cancer: Supracricoid Laryngectomy with CHEP
13 Locally Intermediate Glottic Cancer: Supracricoid Laryngectomy with CHEP
 18 Locally Advanced Glottic Cancer: Supracricoid Laryngectomy
18 Locally Advanced Glottic Cancer: Supracricoid Laryngectomy
 16 Locally Intermediate Supraglottic Cancer: Radiotherapy
16 Locally Intermediate Supraglottic Cancer: Radiotherapy
 15 Locally Advanced Supraglottic Cancer: Larynx Preservation by Transoral Laser Microsurgery
15 Locally Advanced Supraglottic Cancer: Larynx Preservation by Transoral Laser Microsurgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


