13 Locally Intermediate Glottic Cancer: Supracricoid Laryngectomy with CHEP
Abstract
Locally intermediate glottic cancer may be treated by larynx preservation with chemoradiation or conservation laryngeal surgery. Supracricoid laryngectomy (SCL) is very useful for glottic and supraglottic tumors classified as T3 that do not extend to the subglottis and some selected T4a with limited extra laryngeal spread. At least one functional arytenoid must be preserved during this procedure. This technique allows voice rehabilitation and the removal of tracheostomy, bringing a better quality of life when compared to patients who have a total laryngectomy. It may be performed even in elderly patients provided that the patient has good pulmonary function and a multidisciplinary team are available for successful rehabilitation. SCL may be used as rescue surgery post radiotherapy in selected cases but with more frequent complications. When compared to chemoradiation, SCL has similar overall and disease-free survival rates, but with fewer patients requiring total laryngectomy due to recurrence or lack of rehabilitation.
13.1 Clinical Case
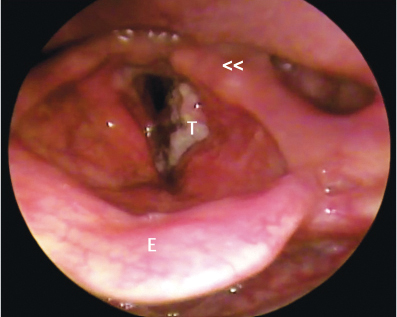
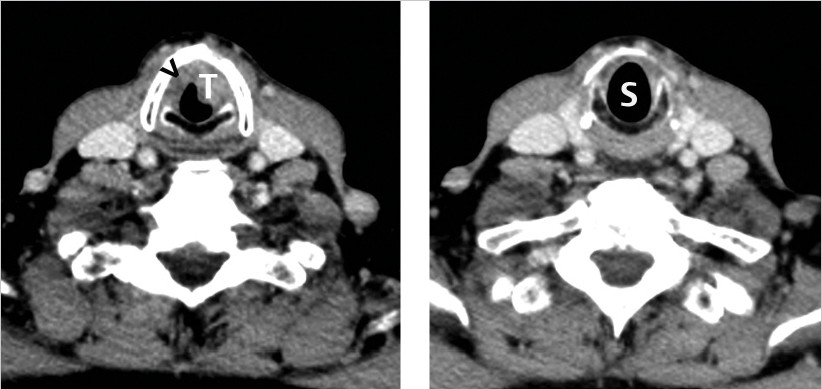
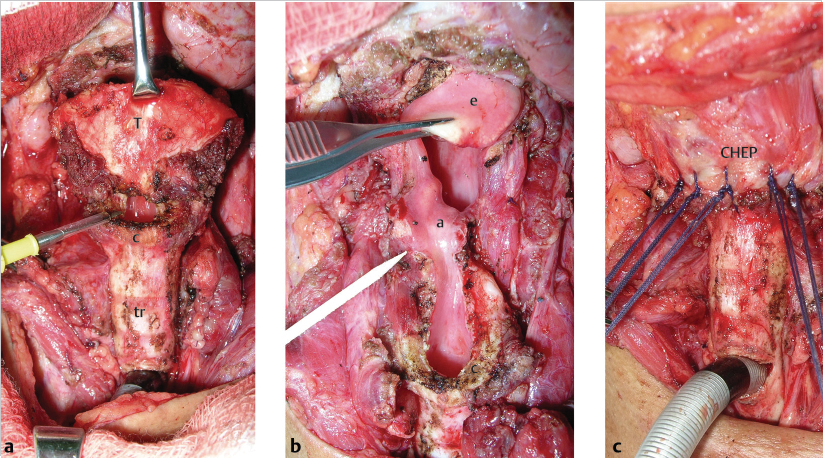
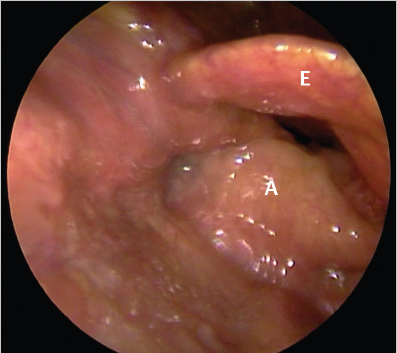
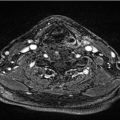
A 73-year-old Caucasian male, retired metallurgist presented to our clinic complaining of progressive hoarseness for 10 months. In the last month, he has noticed difficulty in breathing during physical efforts. He was a 25 pack-year cigarette smoker who had stopped smoking 30 years ago, a social alcohol drinker, and had no comorbidities except for a history of a partial gastrectomy 32 years ago for peptic ulcer. The Karnofsky’s performance status was 70. Physical examination did not reveal any enlarged cervical lymph nodes. Laryngoscopy revealed an ulcerated lesion in the left vocal fold extending the anterior commissure to the anterior third of the right vocal fold, left ventricular fold, left ventricle, and with fixation of the ipsilateral arytenoid ( Fig. 13‑1). Biopsies taken at the time of the endoscopy revealed an epidermoid carcinoma. Computed tomography demonstrated left paraglottic space involvement but no extension to the subglottis ( Fig. 13‑2). Initial staging was T3N0M0. A supracricoid laryngectomy (SCL) and cricohyoidoepiglottopexy (CHEP) with preservation of the right arytenoid and left a selective neck dissection (levels II–IV) were performed ( Fig. 13‑3). The patient was discharged on postoperative day 5, without complications. The cancer was a grade 2 epidermoid carcinoma, measuring 2.5 × 2.0 × 1.5 cm, without vascular or neural invasion, with free margins, and without metastasis to the neck. Pathological staging was pT3pN0. No adjuvant therapy was advised. He did well with speech therapy, and has developed a well-tolerated hoarse voice, with no dysphagia. The tracheostomy tube was removed after 38 days and the feeding tube after 48 days. At 2 years after surgery, he is free of cancer ( Fig. 13‑4) and fully rehabilitated.
Related posts:
 1 T1a Glottic Carcinoma Undergoing Transoral Laser Surgery
1 T1a Glottic Carcinoma Undergoing Transoral Laser Surgery
 6 T1b Glottic Cancer, Vertical Partial Laryngectomy
6 T1b Glottic Cancer, Vertical Partial Laryngectomy
 23 Locally Advanced Supraglottic Cancer: Organ-Preservation Protocol
23 Locally Advanced Supraglottic Cancer: Organ-Preservation Protocol
 20 Locally Advanced Glottic Cancer: Supratracheal Laryngectomy
20 Locally Advanced Glottic Cancer: Supratracheal Laryngectomy
 16 Locally Intermediate Supraglottic Cancer: Radiotherapy
16 Locally Intermediate Supraglottic Cancer: Radiotherapy
 15 Locally Advanced Supraglottic Cancer: Larynx Preservation by Transoral Laser Microsurgery
15 Locally Advanced Supraglottic Cancer: Larynx Preservation by Transoral Laser Microsurgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


