4.1 Introduction
Nutrition, physical activity and public health nutrition
Historically, the science of medicine has differentiated into various specialties based on disease categories, organs in the human body, age, gender, special techniques or medical setting. Current health-care systems, international organizations, medical education, research and patient organizations are still deeply embedded in this structure and are served reasonably well by it.
However, this organizational structure, which may convey the impression of territorialism, also represents a major barrier to collaborative efforts between the different disciplines. Yet it is an interdisciplinary approach that may be critical for the success of research and developmental work, as well as for securing funding, especially in health promotion and disease prevention. Primary prevention directed at risk factors for cardiovascular disease, for example, often depends on experts from diverse areas such as behavioral medicine, nutrition, physical activity and epidemiology.
That today’s structure still considers (clinical) nutrition and physical activity (exercise physiology/orthopedy) as two different medical specialties is a result of history rather than of logic. It is hardly optimally suited for today’s needs in health promotion and disease prevention. For the majority of adults, the most significant controllable risk factors are what they eat and how physically active they are. Preventive research and the development of public health work will not reach its full potential until a more holistic view is adopted.
Collaboration between experts has certainly increased. Public health exemplifies such a multidisciplinary approach to promotion and prevention research, capitalizing on the variety of available expertise, but there is still much room for improvement. This book focuses on public health nutrition, a relatively new specialty, which embraces the promotion of good health through nutrition and physical activity and the prevention of related illness in the population. The links between diet and physical activity and their combined impact on health is a central issue for this rapidly growing multidisciplinary specialty.
This chapter describes some fundamental aspects of physical activity and defines the modern terminology used. It focuses on methodology for the assessment of the amount and character of physical activity at individual as well as at population levels. It is essential for public health work that information is available about the current level of physical activity in the population, and that risk groups are better identified, to make health promotion and disease prevention, and evaluation of the outcome, more meaningful and efficient.
The different instruments available for measuring physical activity and energy expenditure in individuals, groups and populations will be surveyed, with the main focus on methods that can be used in free-living people. The principles, feasibility, advantages and disadvantages associated with the different methods will be discussed, as well as the choice of method for a particular study. In addition, the precision (validity and reliability) of the different methods will be commented upon.
Evolution
The genetic constitution of humans has developed through billions of years of evolution. In the same way as all other living organisms, our ancestors evolved specific characteristics through a process of natural selection. Up to the time of the agricultural revolution, approximately 10 000 years ago, our ancestors were hunters and gatherers, a lifestyle characterized by physical activity. It has been estimated that such a lifestyle would involve daily movement ranges of 10–15 km, mainly through brisk walking.
In contrast to the enormous societal changes associated with the agricultural and industrial revolutions, our genetic pool has remained relatively unaltered during the past 40 000 years. Thus, the biological constitution of modern people remains similar to that originally developed for stone age life. In modern society, motorized transportation, labor-saving devices and sedentary leisure activities, such as watching television and using computers, have reduced the amount of physical activity to levels much lower than those for which our genome was selected.
Thus, from an evolutionary perspective it comes as no surprise that physical inactivity is recognized as a major health problem.
Physical activity and health
There is strong epidemiological evidence indicating that physical activity is highly beneficial to health.
- Higher levels of daily physical activity, or regular exercise, are associated with lower overall mortality rates and a lower risk of cardiovascular disease and mortality.
- The decrease in the risk of coronary heart disease attributable to regular physical exercise is of a similar magnitude to that achieved by refraining from cigarette smoking.
- Regular physical exercise prevents or delays the onset of high blood pressure and lowers the blood pressure in hypertensive people.
- Regular physical exercise, and maybe also a high level of daily activity, is associated with protection from some types of cancer.
- Regular physical exercise reduces the risk of developing type 2 diabetes.
- Physical activity helps to maintain energy balance and thereby prevent obesity.
- Weight-bearing physical activity is essential for the development of the skeleton during childhood and adolescence and for achieving the peak bone mass in young adults.
To gain an even better understanding of the relationship between physical activity and health there is a need for more accurate methods for determining patterns of physical activity and energy expenditure associated with physical activity. Further, the actual amount and patterns of physical activity in the general population are more or less unknown. Thus, to be able to monitor physical activity and identify risk groups in the population, accurate methods for the assessment of physical activity are required. The appropriate design of public health interventions requires the availability of accurate epidemiological data. These data, in turn, depend on valid methods for assessing physical activity.
4.2 Definition of commonly used terms
The terms physical activity, exercise and fitness are often used interchangeably and incorrectly, and therefore they need to be defined.
Physical activity
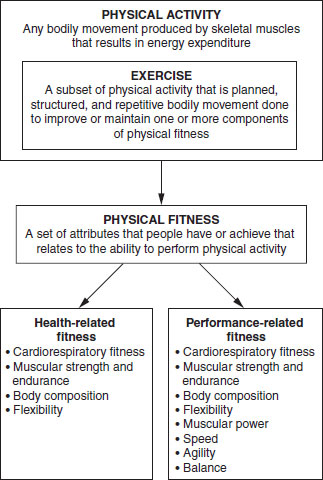
Physical activity is a complex multidimensional form of human behavior, or rather, a class of behaviors, that theoretically includes all bodily movement from fidgeting to participating in marathon running. Although physical activity is behavioral, it has biological consequences. Usually, physical activity refers to the movement of large muscle groups, as when moving the arms and legs. Physical activity is generally defined as any bodily movement produced by skeletal muscles that results in energy expenditure.
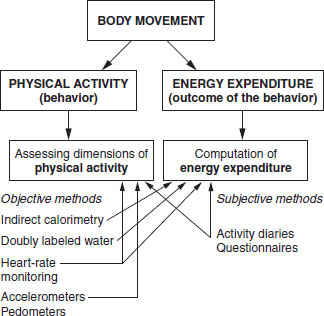
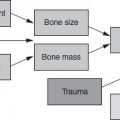
Physical activity and energy expenditure are not synonymous. Physical activity is a form of behavior, whereas energy expenditure is an outcome of that behavior. The relationships between body movement, physical activity and energy expenditure, and examples of different assessment methods are shown in Figure. 4.1.
Characterization of habitual physical activity is often of interest, since this reflects the long-term patterns of physical activity, and most of the health benefits derived from physical activity are a result of regular physical activity performed over extended periods (months and years). However, in many people the physical activity patterns differ between weekdays and weekends, between winter and summer, and from year to year.
To quantify habitual physical activity, different aspects of daily life (domains) in which physical activity takes place need to be recognized. These domains usually include occupational physical activity, transport or moving from place to place, household chores, gardening, and leisure time and recreational physical activity.
Figure 4.1 Schematic model explaining the relationships between body movement, physical activity and energy expenditure. Examples of objective and subjective assessment methods are included.
Exercise
Exercise is defined as a subset of physical activity that is planned, structured, and repetitive bodily movement done to improve or maintain one or more components of physical fitness. Thus, exercise is a minor part of the total volume of physical activity and is performed with a specific purpose. Both exercise and physical activity can be performed at a wide range of intensities (see below). It is generally believed that the exercise intensity has to be vigorous to improve fitness or health. Although this may be true for improving aerobic fitness, many other health benefits can be obtained from moderately intense physical activity.
In fact, the latest physical activity recommendations for public health purposes in adults emphasize the accumulation of 30 min of moderate physical activity every, or nearly every day. This recommendation is similar, with regard to intensity, to the recently published recommendations for young people, according to which all young people (5–18 years of age) should be physically active for at least 60 min every day. In addition, some of these activities should help to enhance flexibility and muscular strength. A detailed description of the evolution of physical activity guidelines, from exercise prescription to public health promotion, is given in Physical Activity and Public Health: A Report from the Surgeon General (http://www.cdc.gov/nccdphp/sgr/sgr.htm).
Physical fitness
Physical fitness is defined as a set of attributes that people have or achieve that relates to the ability to perform physical activity. Physical fitness is an attribute or a physiological state and is therefore clearly distinguished from physical activity and exercise, which are different types of behavior. It is generally considered that physical fitness can be classified as health-related fitness and performance-related fitness. Although these terms seem to overlap to some extent, there is a clear distinction (Figure 4.2). Health-related fitness refers to those components that are specifically related to health and in some instances related to performance, whereas performance-related fitness components relate only to athletic performance. Health-related fitness has been said to include cardiorespiratory (aerobic) fitness, muscular strength and endurance, body composition and flexibility.
Figure 4.2 Relationship between physical activity, exercise and fitness.
Cardiorespiratory fitness relates to the ability of the respiratory and circulatory systems to provide the muscles with oxygen during physical activity. Maximum oxygen uptake (Vo2 max) is often used as an indicator of an individual’s cardiorespiratory fitness. Vo2 max is usually measured by indirect calorimetry during a graded exercise test to exhaustion and is considered the best marker of aerobic fitness. However, various sub-maximal exercise tests, for example ergometer bicycle tests and walking tests, have been developed for the assessment of cardiorespiratory fitness.
Muscular strength is the ability of the muscle to exert force, whereas muscular endurance is its ability to continue with physical activity without fatigue. The body composition is generally considered to be a part of health-related fitness and may be defined as the relative amounts of body fat, muscles, bones and other parts of the body (fat-free mass). The assessment of body composition and its relation to health and disease has been extensively discussed (see Introduction to Human Nutrition, Chapter 2). Flexibility is the potential range of motion of a specific joint.
Specific components of performance-related fitness are muscular power, speed, agility and balance. These components are almost entirely related to athletic performance. Muscular power is the rate at which the muscle can perform work. Agility is the ability rapidly to change the position of the body in space and speed is the ability to perform a movement of the whole body within a short period. Finally, balance is the ability to maintain equilibrium while stationary or moving.
4.3 Dimensions of physical activity
There is no assessment method available today that is able to capture all the different dimensions of physical activity. Researchers have to choose which dimensions of activity they are interested in measuring and then decide upon an appropriate method. Further, there seems to be a relationship between cost, time and effort, on the one hand, and the precision of the method, on the other. The methods that yield data with the highest precision are those that are the most sophisticated and the most time and labor consuming. Thus, when choosing a particular instrument the scientist has to strike a balance between precision, cost, the characteristics of the subjects, time, the number of subjects, feasibility and the overall objectives of the study.
When assessing physical activity, there are at least four main dimensions that are of interest, namely the type, the frequency, the duration and the intensity of physical activity, all of which are important for both descriptive and analytical purposes. The type or mode of physical activity refers to the different specific activities in which the subjects are engaged. This could be of importance for different specific research questions. It is well known, for example, that weight-bearing activities and strength-conditioning exercises are related to bone health.
Most people spend the vast majority (approximately 85–90%) of their awake time in sitting, standing and walking activities, and the relative contribution of each is of importance. Perhaps even more important is the type of activities in the remaining part of the day, since this time may include activities of higher intensity and thereby contribute significantly to the total daily energy expenditure.
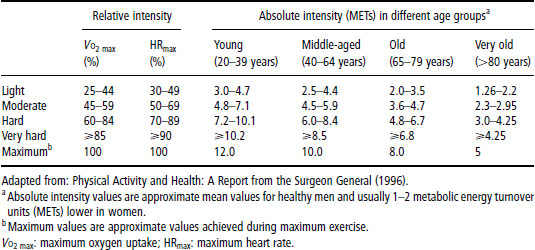
Table 4.1 Relative and absolute classification of physical activity intensity
The frequency of physical activity refers to the number of sessions of physical activity per unit of time. The duration of physical activity is the length in time spent in this activity. In theory, the frequency and duration of physical activity seem easy to assess, since most subjects who are exercising on a regular basis remember the length and number of exercise sessions. It is much more complicated to recall the frequency and duration of less frequently performed activities or activities of lower intensity. Furthermore, in children and adolescents the assessment is even more complicated. First, the activity pattern of young people is much more complex and multidimensional than that of adults. Secondly, the cognitive ability of children to recall physical activity is not normally as well developed as in adults. These problems can at least partly be solved by using objective measures of physical activity.
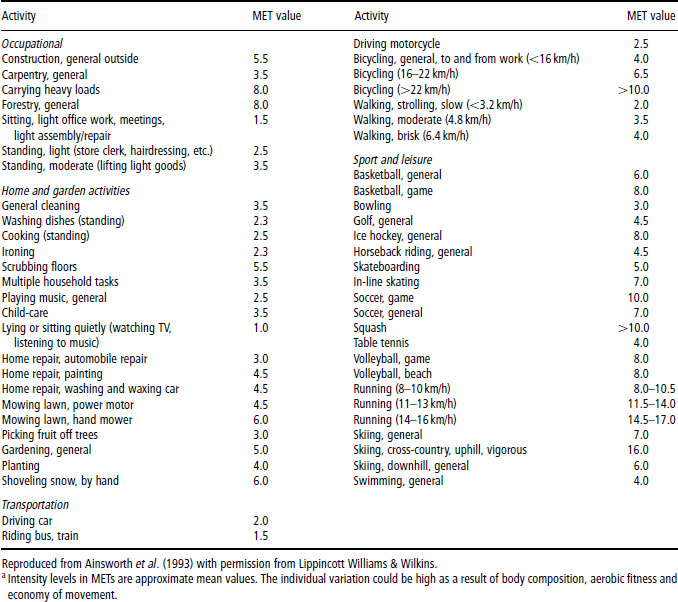
The intensity of physical activity is commonly described as low or light, mild or moderate, hard or vigorous, and very hard or strenuous (Table 4.1). These intensity categories can be defined in absolute and relative terms. A frequently used absolute categorization of the intensity of physical activity is the metabolic energy turnover (MET) classification. One MET corresponds to the energy expenditure during rest, about 3.5ml O2/kg per minute. The MET classification is a useful tool when calculating energy expenditure from subjective assessment instruments such as activity diaries and questionnaires. A wide range of specific activities has been classified according to their respective MET values. Table 4.2 summarizes the average MET values for a number of physical activities. However, the use of an absolute intensity categorization is to some extent limited (see Box 4.1).
Another limitation of the use of MET values relates to differences in the energy cost of movement between subjects with different body compositions. The absolute MET value for a weight-bearing activity (e.g. walking), calculated as the oxygen cost of the activity divided by the resting metabolic rate (RMR), is significantly elevated in obese subjects. Thus, the energy expenditure in obese subjects may be underestimated when calculated from self-report methods using standard MET values (Table 4.2).
Physical activity can also be assessed in terms of the total volume of, or energy expenditure associated with physical activity. Some of the available assessment instruments are able to capture the frequency, duration and intensity, as well as the total volume of physical activity. When assessing physical activity for public health purposes the total volume of physical activity may be of importance, as it seems that this dimension has a significant impact on the health status. If the researcher is interested in a more detailed picture of the activity behavior, an instrument that is able to measure the frequency, duration and intensity may be preferable.
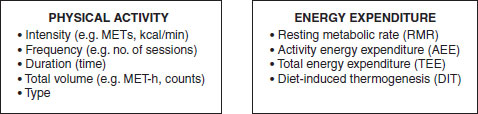
The total volume of physical activity can be quantified in MET-hours per day or week. That is, the intensity of all different activities performed during the assessment period expressed in MET equivalents multiplied by time spent in all activities. This is a common way to express the total volume of physical activity when using questionnaires. When activity monitors are used, the total volume of physical activity is expressed in terms of total counts or the ratio of total counts to registered time. The key dimensions of physical activity and energy expenditure are summarized in Figure 4.3.
Table 4.2 Average metabolic energy turnover (MET) values from a selected range of commonly performed physical activitiesa
If an instrument is designed to quantify the total energy expenditure over a specific period, it is possible to calculate the average daily energy expenditure (ADEE) or total energy expenditure (TEE). The TEE comprises RMR, diet-induced thermogenesis (DIT) and energy expenditure in physical activity (see Introduction to Human Nutrition, Chapter 3). The basal or resting energy expenditure consists of 60–70% of the ADEE, and the DIT constitutes about 10% of the total energy expended per day.
Energy expenditure from physical activity is by far the most variable component of the ADEE. In extreme cases, the energy expended in physical activity is more than four times the resting energy expenditure. Such extremely high values have been reported in endurance elite athletes, for example cyclists racing in the Tour de France. By subtracting estimated or measured RMR from ADEE, the activity energy expenditure (AEE) can be calculated. The AEE is a useful measure, since it quantifies the total amount of energy associated with physical activity. The calculation of AEE usually takes into account DIT, assuming that 10% of TEE is due to DIT.

Figure 4.3 Key dimensions of physical activity and energy expenditure. MET: metabolic energy turnover.
Although the calculation of AEE provides an estimate of energy expenditure devoted to physical activity, it may not differentiate between subjects or groups of subjects with different levels of physical activity. Comparisons of activity levels between individuals require correction of energy expenditure for body size. If two subjects with different body weight do the same weight-bearing activity (e.g. walking or jogging), the gross energy expenditure is higher in the heavier subject even if their movement economy is the same. In contrast, if the subjects do exactly the same amount of work in a nonweight-bearing activity (e.g. bicycling) their gross energy expenditure is almost the same. In attempts to adjust for differences in body size several options are available. TEE or AEE can, for example, be divided by body weight, although the use of ratios (TEE/kg or AEE/kg) to express energy expenditure data has been questioned on the grounds of the variability of the nonzero intercepts between the numerator and denominator, which are necessary if a ratio is to remove the confounding effect of the denominator. Unfortunately, there is no simple approach to adjusting AEE for differences in body size.
Thus, other adjustments for body size differences may be more appropriate. One such approach is to quantify the total amount of physical activity by expressing TEE as a multiple of the resting or basal metabolic rate. The physical activity level (PAL) is calculated as the ratio of ADEE over RMR. PAL can be a useful indicator of the overall physical activity, although it assumes that the variation in ADEE is dependent on body size and physical activity. Nevertheless, PAL is frequently used for interindividual comparisons of physical activity, since it provides a way to adjust for differences in age, gender, body weight and body composition.
Table 4.3 (a) Physical activity level (PAL) values for different lifestyles and activity levels in adults, and (b) suggested PAL values corresponding to different intensities of habitual physical activity in children and adolescents
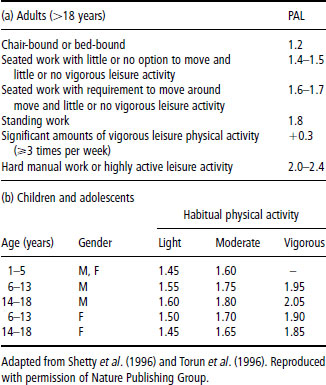
PAL values have been estimated for different lifestyles and activity levels in adults, and for low, moderate and vigorous intensities of physical activity in children and adolescents. A summary of these values is given in Table 4.3. In general, PAL values vary between 1.2 and 2.4. It has been suggested that a PAL value of 1.2 is the lowest “survival” level in a free-living individual. However, lower values for PAL have been reported from wheelchair-dependent individuals.
At the other extreme, there is a distinction between the physical activity that is maximally achievable in short period (weeks) and the maximally sustainable long-term physical activity (years). It has been proposed that a PAL value of 2.5 is the maximal value for longer periods. Such PAL values have been reported, for example, for athletes in regular training and for women during the harvest season in developing countries. Although referring to a limited period (1–3 weeks), even higher PAL values (>4.0) have been obtained for athletes during intense training or competition.
Each dimension of physical activity differs from the others. This fact contributes to the difficulties for the researcher in choosing an appropriate method and comparing results between studies. Furthermore, each dimension may demand its own assessment method. A combination of methods could be an alternative and this possibility should be considered when designing a new research project.
4.4 Reliability and validity of physical activity assessment instruments
All measurements are associated to some extent with measurement errors. Reliability and validity are important issues in connection with all measurements, not least when measuring physical activity.
Reliability
Reliability may be defined as the consistency of measurements or the absence of measurement error. When assessing physical activity, reliability can be considered as the amount of error deemed acceptable for the use of a particular assessment instrument. When testing or developing a new instrument, the test of reliability is the first step, since an instrument cannot be valid if it is not reliable, that is, consistent over time.
Several terms have been used interchangeably with reliability, such as repeatability, reproducibility, stability and agreement. In physical activity assessment, reliability most often refers to repeatability or test–retest repeatability.
Repeatability is the extent to which an instrument produces the same result on different occasions, assuming that the respondents do not alter their behavior between administrations. When assessing physical activity using subjective instruments, such as questionnaires, it is important to ensure that the instrument provides the same result over time. That is to say, when developing a new questionnaire, or applying an old instrument in a new population, a repeatability study is not only recommended but also warranted. For other types of instrument (i.e. objective methods), such as heart-rate monitors and activity monitors, the interinstrument reliability is critically important; that is, a high degree of agreement between two (or more) instruments of the same type.
A relatively high intraindividual day-to-day variability is expected in physical activity assessment. Therefore, when using some types of objective instruments it is of importance to estimate the critical minimum number of days that can be assumed to reflect the overall or longterm pattern of physical activity. Researchers have attempted to define the minimum number of days of assessment required to reflect usual physical activity. It has been clearly demonstrated that both weekdays and weekend days should be included. The minimum number of days that need to be assessed is dependent on the intraindividual and interindividual variability in physical activity and the variability of the assessment method. Thus, different assessment methods require measurement of different lengths of time.
This type of reliability is referred to as stability. Stability has been defined as the day-to-day variability in measurements. It has recently been suggested that 4–5 days of monitoring is necessary to achieve a stability coefficient of 0.8 in children, and that a 7 day monitoring period, including both weekday and weekend days, will provide reliable estimates of habitual physical activity behavior in children and adolescents when an activity monitor is used as the assessment instrument.
Similar data have been reported for other objective assessment methods, such as heart-rate monitoring. Since the activity patterns of young people in general are more variable than those of adults, a 7 day monitoring period also seems to be appropriate in adults. However, a 7 day monitoring period does not take into account seasonal variations. Repeated measurements throughout the year may therefore reflect the habitual physical activity behavior more closely.
Validity
Validity may be defined as the extent to which an instrument assesses the true exposure of interest, in this case physical activity. More precisely, this definition of validity is frequently referred to as internal validity. This implies that there is an absolute measure of the variable of interest against which the alternative assessment instrument is compared. Since physical activity is a multidimensional exposure, an accurate definition of physical activity is fundamental to the design of a subjective assessment instrument (e.g. a questionnaire) and its validation. The above-cited definition of physical activity includes all physical activity and refers to energy expenditure as the outcome variable. The selection of a comparison instrument is fundamental to the design of a validation study. The perfect validation instrument would measure physical activity objectively with uncorrelated error from the method being validated.
Indirect calorimetry is one option when choosing a criterion instrument for validating a specific instrument (e.g. activity monitors) during specific physical activities over a limited period. However, although portable, lightweight indirect calorimetry systems have been developed, they are not suitable for measuring energy expenditure over longer periods.
The doubly labeled water (DLW) method (see below) is considered a gold standard method for measuring TEE over longer periods, such as weeks. This method is therefore probably the best criterion method for validation of an instrument aimed at assessing the total amount of physical activity or energy expenditure. Often it is not possible to use a gold standard method. If a more practical instrument is chosen, it should be highly correlated to a gold standard method. When an assessment instrument that is considered from previous research to be accurate is used as a criterion for validation, the validity studied is referred to as relative validity or concurrent validity.
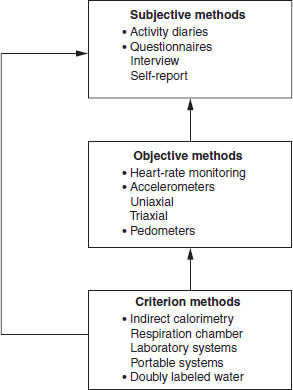
In some studies, a subjective instrument (e.g. a questionnaire) for assessment of physical activity has been validated against another subjective instrument (e.g. an activity diary) or compared with other questionnaires. Although a high correlation between two subjective instruments suggests validity, the instruments are not of a different type and may be subject to correlated error. A study aiming to validate a subjective assessment instrument should therefore include a comparison with an objective instrument. A suggested validation schema is shown in Figure 4.4. Criterion methods should preferably be used when validating objective assessment techniques, and self-report methods should at least be validated against an objective method that has previously been shown to be precise.
Figure 4.4 A study aimed at validating a subjective assessment instrument should include a comparison with an objective instrument. A suggested validation schema is shown.
4.5 Physical activity assessment methods
Laboratory-measured energy expenditure
Laboratory methods are not generally applicable to the assessment of physical activity in field situations. The methods include direct measurement of energy expenditure (heat production) and indirect measurement of oxygen uptake (Vo2
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


