Civilian
Deployment
Military
Military anticipatory guidance
Military eligibility
Military service
Predeployment
Redeployment
Reservist
Resilience
excess weight (15.9%), which decreased from 21.6% the 4 years prior,
poor visual acuity (12.5%), and
the report of psychiatric conditions (12.3%), which increased almost 10% from 2007.6
military can qualify for the Health Professions Scholarship Program (HPSP), which requires a military commitment in exchange for medical school tuition. Commissioning after ROTC or service academy education requires successful completion of undergraduate studies and continued medical qualification. Medical students who are accepted into the HPSP are immediately commissioned into the reserves as officers during school if they meet the physical and legal requirements.
TABLE 75.1 Medical Conditions Not Typically Waivered | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
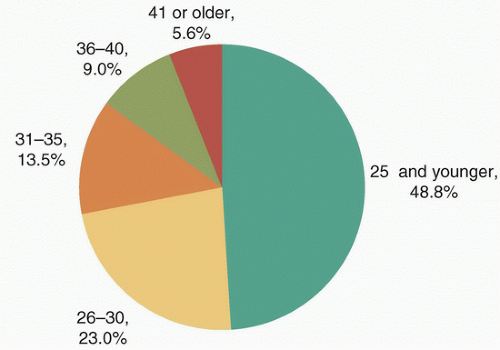 FIGURE 75.1 Age distribution of enlisted active duty personnel. |
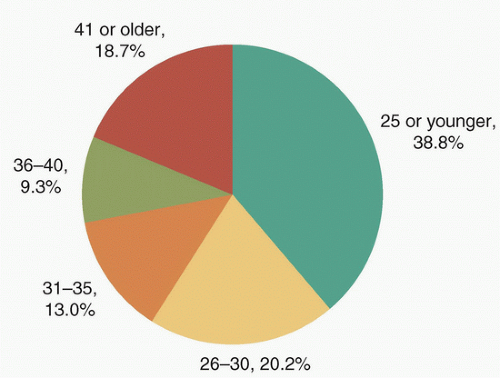 FIGURE 75.2 Age distribution of enlisted reserve personnel. |
including posttraumatic stress disorder (PTSD) that may present without visible manifestations.
Military young adults had similar smoking rates but far less illicit drug use.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



