Vaccine-Preventable Diseases
Learning Objectives
• Identify the etiologic agent of diphtheria
• Recognize the most virulent strain of diphtheria
• Explain the relationship between iron and diphtheria exotoxin production
• Restate the diphtheria exotoxin mechanism of action
• Design a therapeutic regimen to treat diphtheria
• Identify the etiologic agent of whooping cough
• Restate the pertussis toxin mechanism of action
• Design a therapeutic regimen to treat whooping cough
• Compare and contrast whole-cell and acellular pertussis vaccines
• Identify the etiologic agent of tetanus
• Restate the tetanus exotoxin mechanism of action
• Identify the four different types of tetanus
• Design a therapeutic regimen to treat tetanus
• Identify the most common etiologic strain of Haemophilus infections
• Identify the major Haemophilus virulence factors
• Identify the factors that increase the risk of Haemophilus infections in children
• Explain the difference between T cell–dependent antigens and T cell–independent antigens
• Compare and contrast type I and II T cell–independent antigens
• Explain the rationale for conjugating capsular antigens to proteins
• Design a therapeutic regimen to treat Haemophilus infections
• Identify the major virulence factor associated with Streptococcus pneumoniae
• Identify the four different diseases caused by pneumococcus
• Identify therapeutic agents used to treat pneumococcal diseases
• Discuss the advantages and disadvantages of the licensed pneumococcal vaccines
• Identify the major strains of Neisseria meningitidis that causes infections in the United States
• Identify the major virulence factors associated with N. meningitidis
• Identify the three sequelae associated with meningitis
• Identify the role of lipo-oligosaccharide (LOS) in the pathophysiology of meningitis
• Understand the advantages and disadvantages of the three meningitis vaccines
• Recognize the four different types of polio infections and the three types of paralytic polio
• Discuss the mechanisms involved in post-polio syndrome (PPS)
• Compare and contrast the Sabin vaccine and the Salk vaccine for polio
• Identify the complications of rubeola infections
• Identify the two types of rubeola vaccines
• Compare and contrast rubeola and rubella infections
• Discuss congenital rubella syndrome
• Identify the five complications of mumps infections
• Compare and contrast the pathophysiology of varicella infection and varicella zoster infection
• Identify the four sequelae of chickenpox infections
• Explain the mechanism involved in post-herpetic neuralgia
• Design a therapeutic regimen to treat herpes zoster
• Compare and contrast the varicella vaccine and the varicella zoster vaccine
• Compare the transmission routes of hepatitis A and B
• Design a therapeutic regimen to treat hepatitis
• Compare and contrast the vaccines for hepatitis A and B
• Identify the host range for influenza types A, B, and C
• Explain the roles of hemagglutinins and neuraminidase in influenza infectivity
• Compare and contrast antigenic drift and antigenic shift
• Compare and contrast the pathophysiology of seasonal influenza and pandemic influenza
• Design a therapeutic regimen to treat influenza
• Identify the two types of influenza vaccines
• Compare and contrast inactivated and attenuated influenza vaccines
• Identify the disease caused by rotavirus
• Identify the rotavirus strains endemic in the United States
• Explain the pathophysiology of rotavirus infections
• Compare and contrast the three rotavirus vaccines
• Identify the diseases and syndromes caused by papilloma virus
• Identify the papilloma serotypes that cause skin and genital warts
• Identify the papilloma serotypes that cause 70% of cervical cancers
• Identify the therapeutic agents used to treat papilloma virus infections
• Identify the two papilloma vaccines
• Identify the advantages and limitations of papilloma vaccines
Key Terms
Antigenic drift
Antigenic shift
Bacteremia
Bacteriophage
Congenital rubella syndrome
Cytokine storm
Disseminated intravascular coagulopathy (DIC)
Elongation factor 2
Fimbriae
Gamma amino butyric acid
Hemagglutinin
Herd immunity
Intussusceptions
Koplik spots
Lipooligosaccharide
Neuraminidase
Nosocomial infections
Opisthotonos
Orchitis
Osteomyelitis
Otitis media
Pertactin
Post-herpetic neuralgia
Ramsay Hunt syndrome
Reye syndrome
Sabin vaccine
Salk vaccine
Tetanospasmin
Trismus
Vaccine-associated paralytic poliomyelitis (VAPP)
Introduction
Mass vaccination programs have been highly successful in reducing the 57 million deaths caused by infectious diseases in the world each year. The World Health Organization’s (WHO) global initiatives have eradicated smallpox and reduced the incidence of measles and polio deaths. In the last 7 years, vaccination reduced the incidence of measles-related deaths by 74%. Polio is now endemic only in four countries, as opposed to 185 countries in 1988.
In the United States, the success of mass vaccination programs may be one of the greatest public health achievements of the twentieth century. Prior to the institution of mass vaccination programs, 100,000 cases of diphtheria, whooping cough, and tetanus occurred each year. After the institution of vaccination programs, the incidence of these diseases is between 1 and 5000 cases per year. Vaccines against measles, mumps, rubella, and Haemophilus have also reduced annual disease incidence to less than 500 cases per year.
Mass vaccination programs are based on the concept of herd immunity. When a high proportion of a population is vaccinated, person-to-person disease transmission is interrupted by surrounding the infected person with vaccinated individuals. The percentage of vaccinated individuals necessary to disrupt transmission depends on the infectivity of the microbe and the number of secondary infections that are transmitted by a single index case in a susceptible population. Using these data, crude herd immunity thresholds for potentially vaccine-preventable diseases can be calculated mathematically. The threshold of herd immunity is the minimum percentage of the population that must be immunized to prevent person-to-person transmission. When the minimum threshold is reached, disease transmission is stopped, and the epidemic or pandemic is halted. Herd immunity thresholds for childhood diseases are provided in Table 25-1.
Table 25-1
Herd Immunity Thresholds for Common Childhood Diseases
| Infection | No. of Individuals Infected from an Index Case | Herd Immunity Threshold (%) |
| Diphtheria | 6–7 | 85 |
| Measles | 12–18 | 83–94 |
| Mumps | 4–7 | 75–86 |
| Pertussis | 12–17 | 92–94 |
| Polio | 5–7 | 80–86 |
| Rubella | 6–7 | 83–85 |
Modified from Fine P: Herd immunity: History, theory, practice, Epidemiol Rev 15(2):265, 1993.
The previous chapter discussed the general nature of vaccines, additives, and adjuvants. This chapter explores the natures of vaccine-preventable diseases and vaccines licensed for use in the United States.
Diphtheria
Diphtheria is a multiple-organ disease caused by gram-positive Corynebacterium diphtheriae. The three strains of corynebacteria are gravis, intermedius, and mitis. The gravis strain is the most virulent because it divides every 60 minutes and produces large amounts of exotoxin.
Diphtheria Exotoxin
The exotoxin-producing diphtheria bacteria carries a bacteriophage (bacterial virus) gene (Dtox) that codes for the exotoxin. Expression of the Dtox gene is controlled by a diphtheria iron-dependent repressor gene (DtoxR). If sufficient iron is available, the DtoxR gene synthesizes a repressor protein that inhibits the transcription and translation of the Dtox gene. When iron stores are exhausted, the repressor protein is not synthesized and the toxin gene is transcribed and translated.
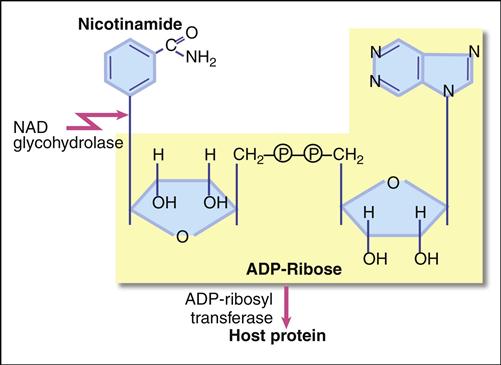
The diphtheria exotoxin is a classic two component A+B protein subunit toxin. Using the B subunit, the intact toxin binds to epidermal growth factor (EGF) receptors on epithelial cells. Protease activity associated with the EGF receptor cleaves the toxin into A and B fragments. The A fragments undergo endocytosis and target nicotinamide adenine dinucleotide (NAD), a coenzyme involved in redox reactions in the cytochrome system. The A subunit has both glycohydrolase and ribosyl transferase activities. Glycohydrolase splits the NAD molecule into nicotinamide and adenosine diphosphate (ADP) ribose. Using the ribosyl transferase function, the A subunit attaches ADP-ribose to histidine (diphthamide) found in the elongation factor 2 (EF-2) protein, which assists in joining of amino acids during protein synthesis (Figure 25-1). Exotoxin inactivation of EF-2 prevents peptide elongation. The reaction is as follows:

Diphtheria Pathophysiology
Diphtheria organisms colonize the tonsils and the pharynx. The secreted exotoxin destroys surrounding tissue, and leakage of blood and plasma in the necrotic tissue activates fibrin, which creates a pseudomembrane at the back of the throat. If untreated, the membrane ultimately obstructs airflow and causes death.
The exotoxin is also transported to the heart, muscle, adrenal glands, kidneys, liver, and spleen. The most frequent diphtheria complications are myocarditis and neuritis. Abnormal heart rhythms occur early in the infection, and necrosis of heart muscle often leads to heart failure.
Treatment
Treatment for active disease usually entails a combination of antitoxin and antibiotics. Equine diphtheria antitoxin is available from the Centers for Disease Control and Prevention (CDC). Antitoxin is most effective in the early stages of the infection because it neutralizes free diphtheria. A 14-day regimen of erythromycin or intramuscular procaine penicillin G also is recommended to treat active cases. Since the bacterium is transmitted by respiratory aerosols, persons coming in contact with the infected patient are given a course of benzathine penicillin G or oral erythromycin. Therapeutics used to treat diphtheria are listed in Table 25-2.
Table 25-2
Therapeutic Agents Used to Treat Diphtheria
| Penicillin G | Arrests bacterial cell wall synthesis by inhibiting cross-linking cell wall polymers |
| Erythromycin | Binds to 50S ribosomal subunits and prevents ribosomal translocation |
| Diphtheria antitoxin | Provides passive protection against circulating toxin. It has no effect on bound toxin |
Diphtheria Vaccine
Diphtheria toxoid is usually included with other antigens in combination vaccines of varying strengths. In the description of diphtheria vaccines, uppercase letters (D, P, or T) denote full strength diphtheria, pertussis, and tetanus. Lowercase letters (d and p) indicate reduced concentrations of diphtheria and pertussis in the vaccine. Acellular components of a vaccine are represented by the lowercase “a” (DTaP).
DTaP and DT vaccines are used through 6 years of age. The DTaP also is formulated with inactivated polio–hepatitis B (Pediarix). Adult Td can be used to vaccinate individuals 7 years and older. Tdap vaccines are available for children between 10 and 18 years of age (Boostrix), and Adacel is approved for individuals 11 to 64 years of age.
Following a four-vaccination series over 8 months, the clinical efficacy is 97%. However, diphtheria immunity wanes with age, and children and adults are at risk for contracting the disease. To maintain protective immunity, children vaccinated with DTaP should receive booster doses at 4 to 6 years of age and every 10 years thereafter. Older children vaccinated with adult Td or Tap should receive a booster shot every 10 years.
Pertussis (Whooping Cough)
The etiologic agent of whooping cough is Bordetella pertussis, an aerobic, gram-negative rod. The term whooping cough is derived from the unique paroxysmal coughing pattern associated with the disease. As a consequence of prolonged coughing, the individual is unable take air into the lungs. When the coughing stops, a protracted inspiratory effort with an associated high-pitched “whoop” occurs. Coughing begins 1 to 2 weeks after infection and lasts for 6 to 10 weeks.
B. pertussis produces a number of virulence factors that include filamentous hemagglutinin (FHA), fimbriae, adenylate cyclase, pertactin, and toxin production. B. pertussis attaches itself to cells in the respiratory tract using the FHA. Secondary attachment points are facilitated by fimbriae and pertactins. The pathology of the disease is caused by a pertussis toxin, a tracheal cytotoxin, and a dermonecrotic toxin.
Pertussis Toxin
The B. pertussis toxin (PTx) is an A+B subunit toxin. Attachment to the cell is facilitated by the B units, and the A unit is responsible for the toxicity. PTx is a ribosyl transferase, which binds ADP-ribose to a membrane-bound regulatory G1 molecule. Inactivation of the G1 protein allows uncontrolled conversion of adenosine triphosphate (ATP) to cyclic adenosine monophosphate (cAMP). Accumulating cAMP disrupts normal cellular function and alters hormone activity. For example, increased cAMP levels increase sensitivity to histamine, which results in increased capillary permeability, hypotension, and shock. PTx also downregulates both cellular and antibody-mediated immune responses, increasing the risk for secondary infections.
Tracheal Cytotoxin
The tracheal cytotoxin is a cell wall peptidoglycan fragment and cannot be classified as an exotoxin or an endotoxin. The toxin kills ciliated epithelial cells in the respiratory tract and stimulates the release of interleukin 1 (IL-1), which acts as an endogenous pyrogen.
Dermonecrotic Lethal Toxin
Dermonecrotic lethal toxin is an exotoxin that causes local necrosis of tissue adjacent to areas colonized by pertussis. The role of the lethal toxin in the pathophysiology of whooping cough is unknown.
Treatment
The treatment of choice is erythromycin, which reduces transmission and the number of organisms in the respiratory tract. Other drugs such as clarithromycin or trimethoprim-sulfamethoxazole can also be used in treatment (Table 25-3).
Table 25-3
Agents Used to Treat Whooping Cough
| Erythromycin | Binds to 50S ribosomal subunits and prevents ribosomal translocation |
| Azithromycin | Same as above |
| Clarithromycin | Same as above |
| Trimethoprim/Sulfamethoxazole | Inhibits bacterial synthesis of folic acid |
Vaccine
The original whole-cell, inactivated pertussis (wBP) vaccine was developed in the 1930s. Although the vaccine was effective, it contained small amounts of the lipopolysaccharide endotoxin. The endotoxin caused significant adverse health effects, including acute encephalopathy, febrile seizures, and hypotonic or hypertonic episodes. The vaccine has been discontinued in the United States.
Acellular subunit pertussis (aBP) vaccines were introduced in 1996 for pediatric use and for adolescent and adult use in 2005. All aBP vaccines contain a pertussis toxoid. However, the concentrations of the filamentous hemagglutinin, fimbriae, and pertactin in vaccines vary considerably (Table 25-4). None of the vaccines contain the pertussis endotoxin.
Table 25-4
Composition of Acellular Pertussis Vaccines
| Product | Target Population | Pertussis Toxin | FHA | PERT | FIM |
| Daptacel | Infant | 10 | 5 | 3 | 5 |
| Infantrix | Infant | 25 | 25 | 8 | |
| Tripedia | Infant | 23 | 23 | ||
| Boostrix | Adult | 8 | 8 | 2.5 | |
| Adacel | Adult | 2.5 | 5 | 3 | 5 |

FHA, Filamentous hemagglutinin; FIM, fimbriae; PERT, pertactin.
Modified from Centers for Disease Control and Prevention. Atkinson W, Hamborsky J, McIntyre S, editors: Epidemiology and prevention of vaccine preventable diseases, ed 10, Washington, DC, 2007, Public Health Foundation.
Following the standard four-dose immunization regimen, between 70% and 90% of the patients are protected from pertussis infection for 5 to 10 years.
Tetanus
Clostridium tetani is a gram-positive, anaerobic organism that is a common inhabitant in the intestines of horses, sheep, cattle, dogs, cats, rats, and guinea pigs. In soils contaminated with animal manure, the vegetative microbe derives nutrients from dead or decaying organic material. When nutrients become limited, the bacteria form spores, which are impervious to heat, chemicals, and other environmental toxins. Viable spores can persist in soil for decades.
Tetanus Toxin
C. tetani spores infect humans by accident, through a deep puncture wound. A deep wound ensures an oxygen-depleted (anaerobic) environment, which allows spores to germinate into vegetative bacteria. Vegetative bacteria release two protein exotoxins—tetanolysin and tetanospasmin. Tetanolysin lyses red blood cells but has no other physiologic function. Tetanospasmin is responsible for the recognized pathophysiology of tetanus.
Tetanospasmin is a 150-kiloDalton (kDal) A+B toxin. The B subunit binds to membrane gangliosides on neural pathways, and the complete toxin is transported to peripheral nerve end plates, the sympathetic nervous system, the spinal cord, and the brain. In the nerve endings, the A subunit inactivates synaptobrevin and prevents the release of gamma amino butyric acid (GABA) and glycine, which normally control the release of acetylcholine. Uncontrolled acetylcholine synthesis and increased nerve firing cause unpredictable muscle contractions, spasms, and seizures characteristic of tetanus.
Clostridium tetani and Disease
Four clinical forms of tetanus have been described: (1) generalized (most common), (2) local (common), (3) cephalic (rare), and (4) neonatal (common in the developing countries).
Generalized Tetanus
Trismus, or lockjaw, is the first sign of generalized tetanus. This is usually followed by a stiff neck, difficulty in swallowing or breathing, and abdominal muscle rigidity. Severe muscular contractions are frequent and last 5 to 10 minutes. Contractions in the long muscles of the back often arch the back in a characteristic form called opisthotonos, which often results in fractures of the spine (Figure 25-2). If the toxin reaches the lung, paralysis of respiratory muscles causes death.
Under the best of circumstances, the mortality rate from tetanus in unvaccinated individuals ranges between 40% and 78%.
Localized Tetanus
Localized tetanus is characterized by muscle contraction near the injury site. The contractions are self-limiting and seldom result in long-term complications.
Cephalic Tetanus
Cephalic tetanus occurs when the organism is present in the flora of the middle ear. Paralysis of facial muscles occurs when nerve transmission is inhibited in the branches of the fifth cranial nerve.
Neonatal Tetanus
Neonatal tetanus is a form of generalized tetanus that occurs in infants when spores infect the unhealed umbilical cord stump. Neonatal tetanus is rare in the United States but common in other countries when contaminated instruments are used to cut the umbilical cord. Globally, an estimated 257,000 deaths occur from neonatal tetanus each year.
Treatment
Tetanus immune globulin (TIG) or equine tetanus antitoxin is usually administered to persons with active tetanus. If TIG is unavailable, intravenous immunoglobulin (IVIG) containing anti-tetanus toxin antibodies is used. Both preparations neutralize and remove free toxins but have no effect on neuronal-bound toxin. To provide active immunity, immunization with the tetanus toxoid should begin as soon as the patient’s condition permits. Common therapeutic agents used to treat tetanus are listed in Table 25-5.
Table 25-5
Agents Used in the Treatment of Tetanus
| Tetanus immunoglobulin | Provides passive immunity by neutralizing free toxin |
| Metronidazole | Is considered a prodrug, which results in the production of cytotoxic radicals |
| Penicillin G | Arrests bacterial cell wall synthesis by inhibiting cross-linking cell wall polymers |
| Erythromycin | Binds to 50S ribosomal subunits and prevents ribosomal translocation |
| Clindamycin | Bacteriostatic agent that binds to 50S ribosomal subunit |
| Tetracycline | Blocks binding of animoacyl transfer ribonucleic acid (tRNA) to the ribosomal A site |
Tetanus Vaccine
Like the diphtheria toxin, tetanus toxin is treated with formalin to create a toxoid. It is offered as a fluid toxoid or absorbed to aluminum hydroxide. Although both formulations induce antibodies, a higher antibody response and duration of protection is induced by the adsorbed toxoid. Tetanus toxoid is available as a stand-alone vaccine or combined with diphtheria toxoid and acellular pertussis to form the DTaP vaccine. Three doses of tetanus toxoid in children 7 years of age and older or four doses in infants confer immunity in 100% of individuals. Without booster doses, immunity wanes, and antibody levels fall below the protective levels after 10 years.
Haemophilus Influenzae Type B
Haemophilus influenzae is an encapsulated gram-negative coccobacillus. It is the etiologic agent of meningitis, otitis media, epiglottitis, pneumonia, arthritis, occult febrile bacteremia, septic arthritis, cellulitis, and purulent pericarditis.
A polyribosyl phosphate (PRP) capsule appears to be the major Haemophilus virulence factor. It protects the organism from phagocytosis and the effects of complement. There are different capsular serotypes (A–F), however, H. influenzae type b (Hib) serotype accounts for 95% of all infections. Haemophilus is endemic in the United States, with epidemics occurring every 3 to 5 years. Most epidemics originate in nurseries or daycare centers, and a single index case can infect 90% of contacts with 48 hours.
Treatment
Children with Hib respiratory infections usually require hospitalization and treatment with cephalosporin or chloramphenicol and ampicillin. Since many Hib strains produce a β-lactamase and are resistant to ampicillin, these medications are not used as monotherapy for severe disease. Third-generation cephalosporins are the drugs of choice to treat invasive Haemophilus infections and meningitis. Glucocorticoids are also useful for reducing the risk of deafness associated with meningitis (Table 25-6).
Table 25-6
Agents Used to Treat Haemophilus Infections
| Ceftriaxone | Arrests bacterial cell wall synthesis by cross-linking cell wall polymers |
| Cefotaxime | Same as above |
| Meropenem | Arrests bacterial cell wall synthesis in a manner similar to penicillin |
| Chloramphenicol | Inhibits the ribosomal peptidyl transferase which elongates polypeptides |
| Ampicillin | Interferes with transpeptidation step of peptidoglycan biosynthesis |
| Dexamethasone | Suppresses migration of polymorphonuclear leukocytes into inflamed areas |
| Rifampin | Binds to β-prime subunit of deoxyribonucleic acid (DNA)-dependent ribonucleic acid (RNA) polymerase and inhibits the transcription of messenger RNA (mRNA) |
Vaccines
To convert the capsules to a T cell–dependent antigen, Haemophilus capsular polysaccharides are conjugated to proteins such as the diphtheria toxoid, the tetanus toxoid, or meningococcal outer membrane proteins (Table 25-7). Three conjugate vaccines are licensed in the United States for the vaccination of infants as young as 6 weeks of age. Each conjugate vaccine uses a different protein carrier.
Table 25-7
Conjugate Vaccines Licensed by the U.S. Food and Drug Administration
| Vaccine | Carrier Protein |
| HbOC (Hib TITER) | Diphtheria protein |
| PRT-T ActHIB | Tetanus toxoid |
| PRP-OMP (Pedvax HIB) | Meningococcal protein |
From Centers for Disease Control and Prevention. Atkinson W, Hamborsky J, McIntyre S, editors: Epidemiology and prevention of vaccine preventable diseases, ed 10, Washington, DC, 2007, Public Health Foundation.
Pneumococcus
Streptococcus pneumoniae is a gram-positive bacterium that is most commonly found in the nasopharynx in children and adults. In high density populations such as military installations or prisons, 50% to 60% of the population may be asymptomatic carriers. Pneumococci are the most common cause of community-acquired pneumonia (CAP), meningitis, and bacteremia.
A polysaccharide capsule surrounding the bacterium is the major virulence factor. It prevents phagocytosis and inhibits the deposition of the complement fragment C3b.
Capsules form the basis for pneumococcal serotyping. More than 90 different serotypes have been reported, and 23 to 25 pneumococcal serotypes infect humans. Two different numbering systems are used to identify pneumococcal serotypes. In the American system, serotypes are numbered in the order in which they were discovered and associated with disease. A Danish numbering system, which is more accepted by clinicians and microbiologists, groups serotypes with similar antigenicity. Predominant serotypes vary by geographic area, socioeconomic status, and age of the patient. Ten common serotypes account for 65% of invasive diseases in adults. Other serotypes (4 and 14) and serogroups (6, 7, 8, 9, 18, 19, and 23) are associated with pneumococcal infections in children younger than 6 years of age.
Pneumococcal Diseases
From the initial colonization in the respiratory tract, the organism spreads into the paranasal sinuses, the middle ear, the lung, and the brain. In children and older adults, pneumococci also cause osteomyelitis, endocarditis, cellulitis and brain abscesses.
Pneumonia
S. pneumoniae is the major cause of community-acquired lobar pneumonia. In lobar pneumonia, an entire lung lobe is infected and filled with serous fluid. A subsequent inflammatory response creates a purulent exudate in the infected lobe. A lobe containing fluid or exudates is commonly termed a consolidated lung. Pneumonia is a leading cause of death in children. Each year 1.8 million children under the age of 6 years die from pneumonia worldwide.
Otitis Media
In some individuals, the organism migrates up the eustachian tube to the middle ear. Inflammatory cells occlude the eustachian tubes and create negative pressure in the middle ear. If the pressure is not equalized by normal ventilation, serous fluid accumulates in the ear. Increased fluid pressure on the tympanic membrane causes pain and difficulty hearing. Severe infections may result in damage to the auditory nerve or perforation of the eardrum.
Bacteremia

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


