Innate Immunity
Learning Objectives
• Describe the barriers that prevent microbial infection of the skin
• Describe the respiratory tract barriers that prevent microbial infection
• Define pathogen-associated microbial patterns (PAMPs)
• Define Toll-like receptors on leukocytes and describe their function
• List 11 different Toll-like receptor ligands
• Compare and contrast the roles of Toll-like receptors in innate and adaptive immunologic responses
• Explain the immunologic mechanisms involved in endotoxins or septic shock
• Describe the components of an acute phase response
• List five acute-phase proteins synthesized by the liver and their function
• Identify antimicrobial agents produced by cells and tissue
Key Terms
Acute-phase proteins
Acute-phase response
Adaptive immune response
Complement
Innate immune response
Opsonin
Pyrogen
Toll-like receptor
Introduction
The body is protected from infection by anatomic and physiologic barriers in the skin and in the respiratory, intestinal, and urogenital tracts. If these barriers are breached an innate immune response is generated. In the response, phagocytic cells, antimicrobial proteins and serum enzymes are activated by molecules common to most bacteria. The innate immune response functions to contain an infection until an adaptive response can be mounted against the infective agent. An adaptive response begins 7 to 10 days after infection and consists of antibodies, CD4Th1 inflammatory response or CD8 cytotoxic cells.
Anatomic and Physiologic Barriers
Skin
The skin is an inhospitable environment for bacterial colonization and growth with the exception of staphylococcus epidermidis, bacteria cannot attach to the outer layer of skin or stratum corneum because it is composed of dead keratinocytes, keratin, ceramides, free fatty acid, and cholesterol. Moreover, the stratum corneum is continually shed and renewed by younger keratinocytes pushing up from below. Bacterial colonization is prevented by other factors as well. Perspiration deposits salt on the skin. High salt concentrations create a hypertonic environment that inhibits bacterial growth. Sebaceous glands also produce a waxlike substance called sebum, which contains lactic acid and propionic acid produced by Propionibacterium acnes—a commensal organism found in the sebaceous gland. Sebum reduces the skin pH to between 3.0 and 5.0, and this acidic environment inhibits bacterial growth.
Respiratory Tract
The respiratory tract is protected from infection by ciliated epithelial cells and a mucous layer. Glycosylated mucous proteins cover the entire respiratory tract and trap particulate matter. The coordinated beating of the cilia on respiratory epithelial cilia moves the mucus upward to the glottis, where it is expelled from the airways or swallowed. This mechanism is referred to as the mucociliary escalator. The mucous covering is replaced several times each day, leading to the production of a pint to a quart of mucus per day. Defective escalator function increases the risk of developing respiratory tract infections, sinusitis, and otitis media.
Mucociliary escalator dysfunction can be inherited or can be the result of environmental insults. For example, primary ciliary dyskinesia (PCD) is an inherited syndrome characterized by impaired transport and the abnormal structure of cilia. In this syndrome, lungs and sinuses are prone to repeated infections.
Environmental insults and drugs often affect the function of the mucociliary escalator. For example, halothane, cocaine, and sulfur dioxide are toxic to epithelial cells. Smoking or inhalation of toxic fumes also injures the epithelium causing loss of ciliated cells. Escalator function can be compromised by cold or dry air that often creates a highly viscous mucus that cannot be moved upward by ciliated cells.
Stomach and Intestine
Stomach acid forms a passive barrier to prevent infection of the intestinal tract. With the exception of Helicobacter pylori (the etiologic agent of gastric and duodenal ulcers), most ingested pathogenic bacteria cannot survive in stomach acid. Bile salts found in the intestine also are toxic to bacteria.
Urogenital Tract
The components of the urogenital tract that actively participate in the innate immune response are the urethra and the vaginal mucosa. The urethra is usually sterile because the persistent flushing of urine prevents bacterial attachment to urethral epithelial cells. The acidity of urine also prevents bacterial colonization. In females, the normal flora of the vaginal mucosa prevents colonization by pathogenic microbes. Acids produced by lactobacilli create a slightly acidic mucosal environment that inhibits bacterial growth. The risk of infection increases when the lactobacillus population is reduced, the pH of urine is increased, or both.
Pathogen-Associated Molecular Patterns
Pathogen-associated molecular patterns (PAMPs) are molecular structures or molecules that are shared by most pathogenic bacteria and some viruses. Most components are constituents of microbial cell walls, single-stranded and double-stranded nucleic acids, or unmethylated deoxyribonucleic acid (DNA). Common PAMPs are presented in Table 2-1. In an innate immune response, PAMPs are recognized by several different mechanisms, including the following:
Table 2-1
Common Pathogen-Associated Microbial Patterns in Bacteria, Fungi, and Viruses
| Peptidoglycan | Gram-positive bacteria |
| Lipopolysaccharide | Gram-negative bacteria |
| Lipoteichoic acids | Gram-positive bacteria |
| Flagellin | Bacteria |
| Lipoarabinomannan | Mycobacteria |
| Beta 1,3 glycan | Fungi |
| Respiratory syncytial virus (RSV) protein | Viruses |
| Double-stranded ribonucleic acid (RNA) | Viruses |
| Lipopeptides | Mycoplasma |
| Unmethylated CpGDNA∗ | Bacteria |
| Profilin-like molecules | Toxoplasma |
∗Unmethylated bacterial deoxyribonucleic acid (DNA) containing cytosine phosphate guanine motifs.
Serum Complement Components and Pathogen-Associated Molecular Patterns
Complement comprises nine serum proteins (Figure 2-1) and produces proinflammatory factors that are chemotactic for phagocytic cells (see Chapter 11). Complement fragments coat bacteria to create opsonins, which are, by definition, molecules that attach to microbes and promote phagocytosis.
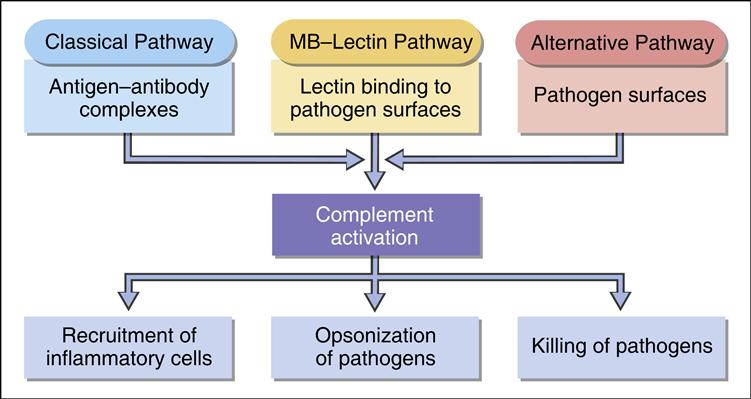
Complement can be activated by different mechanisms. In an adaptive response, complement is activated by antigen–antibody complexes (see Chapter 11). Three other mechanisms do not require the presence of antibody and are activated during an innate immune response. Complement can be activated by interaction with select molecules (e.g., zymozan) on microbial surfaces in an alternative complement activation pathway. Lectins (proteins that bind to sugars) also activate the complement cascade in the mannose-binding lectin (MBL) pathway. Some acute phase proteins produced by the liver during inflammation activate the complement cascade (see Acute Phase Response).
Mannose-Binding Lectin Complement Activation Pathway
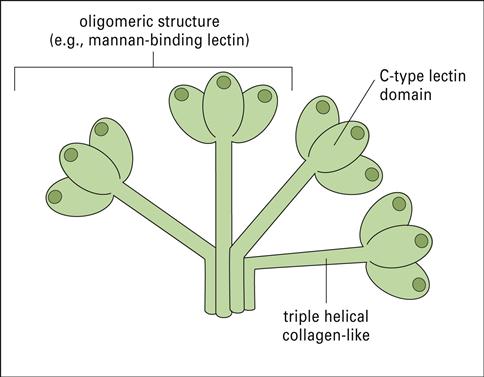
Collectins are a family of lectins that react with terminal mannose or fructose molecules on microbes and activate complement. The collectin family includes Mannose-binding lectin (MBL), bovine conglutinin, lung surfactants A and D, and bovine collectin 43. Structurally, collectins are multi-meric proteins with a “flower bouquet” or an “X-like” structure (Figure 2-2).

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


