64 Uveal Melanoma
Epidemiology, Genetics, and Environmental Factors
Uveal melanoma is the most common primary intraocular malignancy of adults. The annual incidence is estimated to be between four and seven cases per million people in the United States, Canada, and Europe.1–4 Ocular melanomas in the United States represent approximately 3% to 5% of all melanomas, with approximately 1500 to 2000 new cases diagnosed each year in the United States.3–6 In contrast to cutaneous melanoma, which has shown a fivefold to sixfold increase in incidence over the past several decades,7 the frequency of ocular melanoma appears not to have changed.8,9 Of ocular melanomas, 85% are reported to be uveal, 5% conjunctival, and 10% occur at other sites. Uveal melanoma occurs more frequently in light-skinned people with light eyes. The incidence rate among African Americans is reported nationally to be less than one eighth that found in whites; it is also rare among Americans of Asian extraction.3 A steady increase in incidence with age is seen, with peak incidence between 60 and 79 years of age, whereas less than 2% are younger than 20 years old at the time of diagnosis.5,10 Incidence rates are generally higher for males (RR = 1.3).3
The cause of uveal melanoma is largely unknown, and there is mixed evidence regarding genetic susceptibility and host-factor patterns. It is extremely rare to have bilateral tumors, multiple uveal melanomas, or familial uveal melanomas.11 Uveal melanoma is more prevalent in white patients in an eye with ocular or oculodermal melanocytosis (nevus of Ota).12,13 The lifetime risk of uveal melanoma in patients with oculodermal melanocytosis is estimated to be 1 in 400.14 Reports of cutaneous and uveal melanoma occurring as double primary malignancies, some in the presence of dysplastic nevi or atypical mole syndrome, as well as familial clustering of both melanomas have led to speculation that cutaneous and uveal melanoma may have a common inheritable variant.15,16 However, others have been unable to detect an association between intraocular melanoma and cutaneous dysplastic nevi.17,18
Various molecular and genetic markers are currently under study.19 Chromosomal alterations most often observed in uveal melanoma include deletion of chromosome 3 (a finding associated with poor prognosis), over-representation of 6p, loss of 6q, and multiplication of 8q.20–24 Loss of chromosome 3, loss of 6q, and gains of 8q are significant predictors of survival.25,26 Abnormalities of chromosome 3 and 8 are present in approximately 50% of all cases.27 Tumors with monosomy 3 also exhibit amplification of c-myc (encoded on chromosome 8q24.1), suggesting that both play a role in the pathophysiology of uveal melanomas.28 In contrast, monosomy 3 and amplification of 8q are rare in cutaneous melanomas. Other common genetic alterations in cutaneous lesions are otherwise rare in uveal melanomas; these include deletion and translocation of 1p, and mutations in TP53, BRAF, and CDKN2.20,29,30 Further, c-myc amplification, described in 70% of uveal melanomas, is associated with improved survival.31,32 The opposite is found in cutaneous melanoma, in which high levels of c-myc are associated with worse outcomes. The distinct cytogenetic characteristics of cutaneous and uveal melanomas support the hypothesis that different mechanisms are involved in the genesis and progression of these neoplasms.21 The role of other molecular targets remain under investigation, including Bcl-2, ubiquitin-proteasome, histone deactylase, mitogen-activated protein kinase, AKT, receptor tyrosine kinases, intercellular adhesion molecules, matrix metalloproteinase, and angiogenic factors.19,30
More recently, gene expression profiling data shows that a more accurate assessment of prognosis is possible with a transcriptomic classification of uveal melanomas based on ribonucleic acid analysis of the primary tumor. Tumor samples can be processed from enucleation tissue or fine-needle biopsy before institution of eye-sparing therapies.33,34 A “class 1” signature is associated with an excellent prognosis, whereas a “class 2” signature portends a high risk of metastatic death. The latter class is associated with other predictors of poor prognosis, including epithelioid cytology, looping extracellular matrix patterns, and monosomy 3. This molecular classification represents a valuable prognostic tool to identify high-risk patients.
The impact of other environmental factors such as exposure to sunlight and ultraviolet (UV) light have been studied in uveal melanoma because of the known association with cutaneous melanoma. However, unlike in cutaneous melanoma, intermittent outdoor leisure, chronic occupational sunlight exposure, and birth latitude are reported to be nonsignificant factors in a recent meta-analysis.35 Perhaps most problematic with the putative link between sunlight exposure and uveal melanoma is that virtually no UV-A or UV-B is transmitted through the lens and cornea in adults. The juvenile lens may allow small amounts of UV radiation to reach the retina, but tissue overlying the uveal tract would still likely filter out the residual UV radiation. Arc welding exposure is a significant risk factor for development of uveal melanoma.35,36 Other causal factors, including cell phone usage, have not shown convincing evidence of correlation to uveal melanoma.6
Anatomy
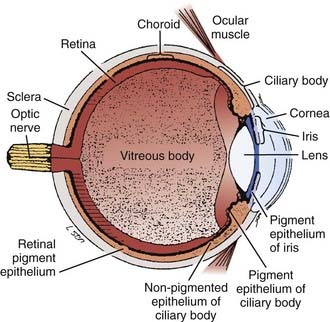
Melanomas develop in the uveal tract, the vascular support layer of the eye. Approximately 80% of uveal melanomas involve the choroid, which is the posterior portion of the uveal tract located under the retina. Less than 10% involve the iris; and approximately 10% to 15% involve the ciliary body, which contains the muscle responsible for accommodation and movement of the lens (Fig. 64-1).37 The Bruch membrane, the transparent inner membrane of the choroid, is significantly weaker than the sclera (which is the tough fibrous outer layer surrounding the choroid). As choroidal lesions grow, the Bruch membrane can stretch and eventually rupture, allowing the tumor to penetrate through and create the characteristic “collar button” or mushroom-shaped deformity by protrusion into the retina. This geometry is virtually pathognomonic for a uveal melanoma. Scleral penetration is significantly less common, and is often associated with tumor tracking along a vessel.
Pathologic Conditions and Prognostic Factors
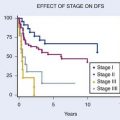
Uveal melanoma cells are characteristically spindle-shaped or epithelioid; these latter, plumper cells are associated with a worse prognosis. In addition to cellular characteristics, pathologists have quantitated pigment content, argyrophil fiber content, and the presence of tumor necrosis. This is the basis for the Callender classification initially described in 1931.38 It has been modified to describe several pathologic patterns including spindle, mixed, necrotic, and epithelioid types. The American Joint Committee on Cancer (AJCC) 2002 histopathologic staging is shown in Table 64-1. It is likely that benign choroidal nevi were included in the “malignant” category in early reported series.39 Virtually no tumor-related mortality is observed with the spindle A cell type,40 although the spindle B variant is clearly malignant. In patients undergoing enucleation, eye wall resection, or irradiation, several factors are described as having poor prognostic significance. These include (1) gross tumor features, such as large tumor size (tumor diameter and tumor thickness), anterior location (ciliary body invasion), proximity of tumor to the foveal avascular zone, scleral penetration, and optic nerve invasion; (2) pathologic features, such as epithelioid cell type, high mitotic rate, large nucleolar size, lymphocytic infiltration, vascular pattern (microvascular loops and networks); (3) genetic features, including alterations in deoxyribonucleic acid content, gene expression profiling, and monosomy of chromosome 3; and (4) patient factors such as older age, and in some series male gender linked with impaired tumor control27,41–66 (Table 64-2 and Fig. 64-2).
Table 64-1 Histopathologic Staging of Uveal Melanomas
Table 64-2 Negative Prognostic Factors
| Tumor |
|---|
| Pathologic |
|---|
| Genetic/Patient |
|---|
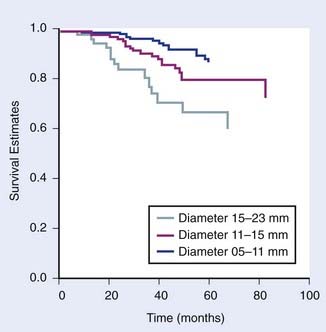
FIGURE 64-2 • Kaplan-Meier survival estimate for time until metastasis following helium ion or iodine-125 plaque by largest tumor diameter.
(From Char DH, Castro JR, Quivey JM, et al: Uveal melanoma radiation: 125-I brachytherapy versus helium ion irradiation, Ophthalmology 96:1708, 1989.)
In most studies, several additional factors have no consistent effect on survival with univariate or multivariate analysis, including duration of signs and symptoms, reticulin fiber content, pigmentation, necrosis, location of the posterior tumor margin, or penetration through the Bruch membrane.41,44 In most historic series, cell type is the most important single predictor of death following enucleation. The relative importance and relationship between various prognostic factors is uncertain, with current series showing gene expression profile of the tumor to be most tightly correlated with prognosis.33,34,67
The predictive value of melanoma genome studies are under study as a more quantifiable and reproducible system of tumor classification. Currently some groups report testing for monosomy 3 on tumor specimens for prognostic purpose. One investigator found that the relapse-free survival in 30 patients with monosomy 3 was 43% in contrast to 100% in 24 patients without this chromosomal loss.27 Our current practice has been to use a more sensitive technique of measuring intratumor melanoma gene alterations, which shows superior results in terms of accuracy of prognostic information.33,67 These gene studies are performed on patients who have either fine-needle biopsies or surgical resections, and the assays are better correlated with tumor-related mortality and patient survival than monosomy 3. Tumors in a class 1 pattern have less than 15% tumor-related mortality, whereas class 2 tumors have more than 85% metastatic deaths within 5 years. This tumor genomic classification provides a risk assessment of patients and potentially may help delineate which patients benefit from specific adjuvant management or prophylactic systemic treatment.
Clinical Presentation
The appearance of fundus lesions on indirect ophthalmoscopy is often diagnostic. Examination includes measurement of the tumor diameter and thickness, delineation of tumor location, geometry, and tumor coloration. Patients are also evaluated for associated subretinal fluid or exudative detachment. The pigmentation of uveal melanomas is variable, with as many as 25% of cases being amelanotic; most uveal melanomas are light to medium in pigmentation. Lesions that most commonly simulate uveal melanoma include nevi, choroidal hemangiomas, rhegmatogenous retinal detachments, age-related disciform lesions, scleritis, and choroidal metastases (most commonly from breast, lung, and gastrointestinal cancer).68–70 Making the correct diagnosis in suspected uveal melanomas is a function of observer experience, media clarity, and tumor size.71 Most ocular oncology units currently report a 99% accuracy,72 although a generation ago, 20% of eyes enucleated with a clinical diagnosis of this malignancy had a simulating lesion on histopathologic examination.39,73–77
Diagnostic and Staging Studies
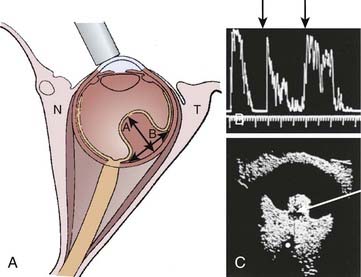
The evaluation of patients with a possible uveal melanoma includes clinical examination, fundus photography, and ocular ultrasonography with immersion B-scan and Kretz A-scan (Fig. 64-3). Other diagnostic tests include visual field testing, indocyanine green angiography, optical coherence tomography, and magnetic resonance imaging (MRI). Clinical findings more frequent in larger tumors include the presence of subretinal fluid and a collar button configuration. Fluorescein angiography, which can identify tumor vessel leakage, is often not diagnostically useful except in differentiating uveal melanomas from hemorrhagic choroidal simulating lesions; in a masked study without other ancillary tests, this technique has a diagnostic accuracy of only 63%.75 In contrast, experienced ultrasonographers can differentiate uveal melanomas from simulating lesions in approximately 89% to 96% of cases that require therapeutic intervention.78,79 Ultrasound factors useful for diagnosing melanoma include choroidal excavation, orbital shadowing, acoustic quiet zone, and homogeneity on A-scan (Fig. 64-4). Ultrasound is also useful and reproducible in measuring tumor height, although it is less reliable in tumors located anterior to the equator because of the difficulty in positioning of the A-scan probe. Extensive subretinal fluid over the lesion can also lead to inaccuracy of A-scan with an overestimate of tumor height. Some observers have used ultrasound to estimate tumor diameter, although we note this to be less accurate in lesions that have a large area of relatively flat tumor extension.

MRI has been evaluated in this neoplasm.80–83 Although the T1 and T2 pattern of pigmented uveal melanomas is relatively typical, a number of false-negative and false-positive cases have been reported. This is a relatively expensive test that usually does not increase diagnostic accuracy afforded by ultrasound. MRI can be diagnostically useful (although inaccuracies have been noted) in the detection of localized extraocular extension, and in the differentiation between a uveal melanoma and a peripheral choroidal hemorrhage resulting from an extramacular disciform lesion. MRI is potentially useful in providing anatomic information that can improve tumor volume delineation for treatment planning purposes.84,85
For smaller pigmented lesions, noninvasive diagnostic tests are less accurate and it is often difficult to distinguish an atypical benign melanocytic proliferation from a small melanoma less than 3 mm thick.74 We have labeled patients who have indeterminate pigmented choroidal lesions with the neologism nevoma. This includes lesions that are too large to be clinically thought of as nevi (generally >7 mm in diameter and >1.5 mm thick), but that appear to be relatively inactive. The clinical approach to these lesions is usually close observation with serial fundus photography to assess changes in tumor borders, and ultrasound A-scan to assess changes in tumor thickness (height).
It is unusual (approximately 1% in contemporary series) to simultaneously present with metastatic disease and a primary uveal melanoma; the markedly shortened survival in this setting significantly influences the treatment approach. The most common sites of metastatic spread are liver, lung, and bone.86 The metastatic evaluation includes a thorough physical examination with liver function studies and a computed tomography (CT) scan of the abdomen if serum abnormalities are detected. Chest x-rays have a very low yield for detecting metastasis, but are a useful baseline study.87,88 Whole-body positron emission tomography (PET)-CT scans have been increasingly used for detection of uveal melanoma metastases. The clinician must be mindful of other primary neoplasms, including breast, lung, and genitourinary cancers, which may produce choroidal metastases that simulate uveal melanoma.
Fine-needle aspiration and gene profiling of tumor samples can be used for diagnostic and prognostic purpose. Gene expression separated into class I and II patterns is shown to correlate tightly with tumor-related mortality and provides risk assessment that can be useful for clinical decision-making.33,34,67
Staging System
There are two staging systems commonly used in uveal melanomas, AJCC and Collaborative Ocular Melanoma Study (COMS).89–92 The AJCC tumor (T) classification is defined according to the tumor dimensions, including the largest basal diameter and the tumor thickness or height. The AJCC staging also subgroups tumors with microscopic or macroscopic extraocular extension within the T1 through T2 categories. Stage grouping is as follows: stage I includes T1-N0-M0; stage II is T2-N0-M0; and stage III is T3– and T4-N0-M0 disease. Any nodal or metastatic spread is considered stage IV disease. Of note, ciliary body and choroidal melanomas are staged differently from iris melanomas.89 In general, iris melanomas are often detected earlier and are smaller in size than posterior melanomas.
A second staging system is recommended by the COMS. The two systems, presented in Table 64-3, differ in the definition of stages, although the newer AJCC staging system is modified based on clinical observations in the COMS trials. Size criteria definitions vary across studies and must be reviewed carefully when comparing patient series. Generally, COMS small, medium, and large tumors now roughly correspond, though not exactly, with AJCC T1, T2, and T3 or greater tumors, respectively. Unfortunately, neither staging system takes primary tumor location or visual acuity into consideration. These factors greatly influence the optimization of treatment modalities. Most authors with large series have reported these factors and attempted to correlate them with tumor control and treatment complications.
Standard Therapeutic Approaches
The optimum management of uveal melanomas is controversial. In small, indeterminate, pigmented tumors (≤3 mm thick and ≤10 mm in diameter), data reported by our group and others support the concept that serial observation of these lesions is reasonable unless growth is documented.93 Approximately two thirds of these lesions do not grow. The survival in patients whose lesions subsequently grow and require treatment is no worse than has been reported with prompt, early therapy of small lesions. In addition, many such patients are allowed to maintain good vision in an eye that would have had marked treatment sequelae.
For medium-sized, T2 or growing T1 tumors, various surgical and radiation-based therapeutic alternatives are reported in the literature. Surgical intervention includes local resection with or without adjuvant radiation, enucleation, or exenteration. Radiation modalities include plaque brachytherapy, charged particles (i.e., protons or helium), and radiosurgery. Both prospective COMS and retrospective studies demonstrate comparable survival rates between enucleation and irradiation.94–96 Selecting the optimal radiation modality depends on tumor and patient parameters as well as accessibility to specialized treatment facilities.
Photocoagulation, Laser Treatment, and Thermotherapy
Although photocoagulation and laser treatment have been used to treat small choroidal melanomas and high-risk nevomas for approximately 40 years, the efficacy of these treatment modalities is limited. Newer laser approaches have used an 810 nm laser with long duration treatments. This treatment, termed transpupillary thermal therapy, involves delivering a beam of infrared radiation through a dilated pupil into an intraocular tumor. The exact cytotoxic mechanism of this infrared diode laser is uncertain; however, it is thought to result in tumor cell necrosis by cell membrane damage, protein denaturation, chromosomal damage, and breakdown of mitochondria.97 The maximum depth of penetration of this modality is estimated to be about 4 mm. In some centers, the use of transscleral (rather than transpupillary) infrared diode laser is being investigated.
Most centers use thermotherapy to treat small posterior pole choroidal tumors, such as high-risk choroidal nevomas (based on clinical, ultrasound, and fluorescein angiographic criteria); small, growing melanomas in close proximity to the optic nerve or fovea; or small, growing tumors in the posterior pole that have produced sufficient subretinal fluid to decrease vision.98 Some investigators have combined infrared diode laser with radiation, either to more promptly reduce exudative retinal detachments99 or for adjunctive therapy in posterior pole choroidal melanomas to improve the efficacy of brachytherapy.100
Melanomas contiguous to the disc should not be treated by this technique. There is as much as a 60% late recurrence rate, and several centers report localized extraocular recurrences from the intrascleral extension of the tumor not effectively treated by this modality.100 Retinal complications are described in approximately 30% to 75% of treated eyes, including retinal detachment, retinal vascular occlusions, hemorrhage, or internal limiting membrane contracture and associated decreased vision.
Eyewall Resection
Surgical resection of uveal melanoma has been described in several series.101–104 The rationale for eyewall resection is to attempt to preserve the eye and useful vision. Adjunctive radiation is an important part of this approach, using either protons or radioactive episcleral plaques. Eyewall resection with or without radiation has been recommended for patients in whom radiation alone may carry increased complication risk (i.e., those with thicker tumors) or decreased expected local control. A secondary benefit of eyewall resection is the availability of tumor specimen for diagnostic and prognostic research purpose.
The major problem with a local tumor resection is lack of predictability. In our experience we have treated tumors up to 18 mm in diameter and 14 mm thick with tumor resection. Although some of the eyes were retained with 20/20 vision, others have been lost at the time of surgery and others have had what appeared to be good tumor resection but with major ocular complications. In a review of 125 patients followed for a mean of 6 years, 76% of eyes were successfully retained and 53% had a final visual acuity of at least 20/40.105
A recent analysis reports on eyewall resection of 344 cases with median tumor diameter 13 mm (range 4-21 mm) and median tumor thickness 8 mm (range 1.5-16.5 mm).104 Adjunctive ruthenium plaque brachytherapy was used in 37.5% of patients. Local tumor control at 8 years was 47% to 75%, depending on the number of risk factors (higher local failure rate with diameter >15 mm, epithelioid cells, posterior extension < 3 mm from disc or fovea). Ocular conservation rate at 8 years ranged from 57% to 81%. Visual acuity of at least 20/40 was maintained in 38% to 43% of patients; and if only conserved eyes were analyzed, then 50% of eyes retained this level of vision. Others have retrospectively reported on large tumors with increased local tumor relapse and enucleation rate with local resection (with or without radiation) versus plaque therapy alone.106
The exact role of eyewall resection remains to be defined. Generally, eyewall resection is not considered ideal in cases of very large tumor size, optic disc involvement, extensive ciliary body or retinal invasion, extrascleral extension, diffuse or multifocal disease, ring melanomas, and if it is unlikely that useful vision will be conserved in the affected eye.103,106 Eyewall resection is a technically difficult surgery, can require hypotensive anesthesia, and is not readily available at many centers. Complications for eyewall resection can include hemorrhage, retinal detachment, ocular hypotony, and anesthetic effects. Postoperative brachytherapy can cause maculopathy, optic neuropathy, glaucoma, and wound dehiscence.
Enucleation
Although enucleation was the standard method for treating uveal melanomas as early as 1882,107 the effect of this treatment on the natural history of uveal melanomas was called into question by Zimmerman,108 who proposed that surgical manipulation at the time of enucleation might cause tumor dissemination. Several subsequent analyses pointed out the pitfalls inherent to his retrospective review and challenged this conclusion.109 Nonetheless, the role of enucleation in the treatment of uveal melanoma has diminished with the availability of successful alternative therapies. Several indications still exist for enucleation, including patient request after informed consent, failure of alternative therapy, tumor involving more than 40% of the intraocular volume, tumor with large extrascleral extension, tumor in a blind or painful eye, and a melanoma in an eye with marked neovascularization. In multiple studies, patients who have known visceral metastases from uveal melanoma have a median survival of less than 6 to 7 months.88,109 Patients with metastatic disease do not benefit from enucleation unless the eye is painful.
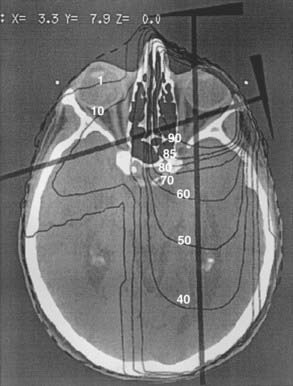
Adjunctive pre-enucleation radiation therapy or postoperative radiation has been used in an attempt to minimize local recurrence and tumor-related mortality.110–113 Preoperative irradiation was given to 42 patients in our institution in the hopes of exploiting the theoretic advantage of this approach (Fig. 64-5). Unfortunately, when compared with 33 patients with similar tumors enucleated by the same surgeon without preoperative irradiation, no benefit could be measured.110 The dose of radiation was 20 Gy given in 5 fractions of 4 Gy in this small series. A subsequent study by the COMS group using the same daily fractionation and total dose but done in a multi-institutional, prospective randomized setting, also found no survival advantage with pre-enucleation radiation.92,114
Exenteration
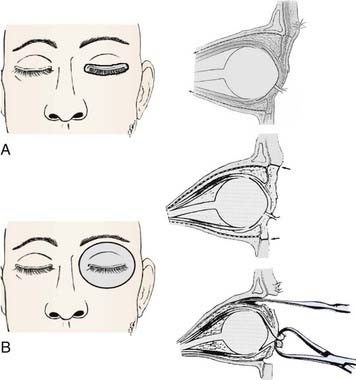
If there is diffuse extraocular extension, exenteration is indicated provided there are no metastases.115 Postoperative external-beam radiation therapy may be employed. Exenteration can be performed using either lid-sparing, or non–lid-sparing techniques (Fig. 64-6A, B). An incision is made through the periosteum at the orbital rim to free orbital contents from the orbital bones. A temporalis muscle flap is often used to minimize the surgical defect and a partial thickness skin graft can cover the defect left by the eyelid resection.
Charged-Particle Radiotherapy
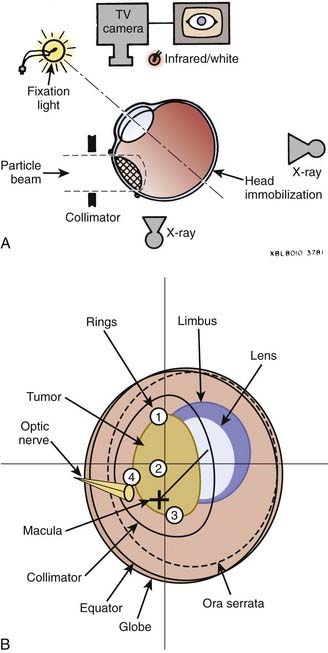
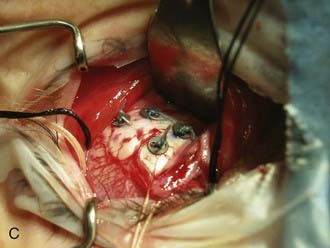
The development of uveal melanoma treatment with the expanded Bragg peak of charged particle beams was described by Constable and others working at the Harvard cyclotron with a 160-MeV proton beam.116,117 Accelerated charged particles, including protons and helium ions, can treat small targets with minimal lateral scatter and radiation dose beyond the end of the Bragg peak. Studies with modulated and collimated proton beams demonstrate a relative biologic effectiveness (RBE) of close to unity when compared to 2-meV photon beams. The adaptation of this technique for humans required the development of sophisticated tumor mapping using the surgical placement of tantalum rings (Fig. 64-7A), immobilization devices controlling for both head position and gaze angle, and a computerized treatment planning program.118,119 A similar technique using helium ions was developed at the Lawrence Berkeley National Laboratory (LBNL) in collaboration with the Department of Radiation Oncology and the Ocular Oncology Unit at the University of California, San Francisco (UCSF). The RBE of the helium ion beam is 1.3, slightly greater than the proton beam, and accordingly dose adjustments were made.120 Because of decommissioning of the heavy ion synchrotron at LBNL, the program was moved to a 76-inch cyclotron at the Crocker Nuclear Laboratory (CNL) on the University of California, Davis, campus.121
More than 3000 patients with uveal melanoma have been treated with protons at the Harvard cyclotron to date. The prescribed dose in their series is 70 cobalt gray equivalent (CGE) in five fractions over 7 to 10 days (assuming CGE = proton Gy × RBE 1.1). Reporting on more than 2000 of their patients, their local control at 5 years is 97% and at 15 years is 95%.122–125 The 5-year actuarial survival for the patients treated with protons is 78.5% for the entire group, with 97.5%, 85.8%, and 58.1% survival for patients with small, intermediate, and large melanomas, respectively. The 5-, 10-, and 15-year tumor-specific survival rates are 86%, 77%, and 73%, respectively. Using the Cox proportional hazards model, the factors that predict decreased survival on multivariate analysis include maximum tumor diameter greater than 15 mm, ciliary body involvement, age older than 59 years, and the presence of extrascleral tumor extension.52
These results have been confirmed at the Paul Sherrer Institute by Egger and colleagues,43 who reported on 2435 patients treated between 1984 and 1998 with 54.5 Gy in four fractions (corresponding to 60 CGE). The local control rate is estimated to be 95.8% at 5 years and 94.8% at 10 years (by Kaplan-Meier). Patients treated with a reduced safety margin because of proximity of the tumor to the fovea have a much higher local failure rate at 5 years of 28.7%. Local tumor control is correlated with survival rates; the overall 10-year CSS is 72.6% for patients with controlled tumors versus 47.5% for those with local recurrence. In their series, with greater experience including updated planning software and techniques, patients treated after 1993 have higher control rates than those treated before (5-year local control 99% versus 90%-96% and 5-year CSS 88% versus 82%-83%, respectively). Additional factors adversely affecting prognosis include older age, increased amount of retinal detachment, ocular melanosis, large tumor diameter, increased tumor height, and extrascleral extension.
A randomized dose trial for proton-beam therapy was conducted on 188 patients comparing doses of 50 CGE and 70 CGE in five fractions and found no significant difference between dose regimens in terms of ocular toxicity or local control at 5 years.126 As described, Egger and colleagues reports 99% control with a contemporary subgroup of patients treated with proton therapy to a dose of 54.5 Gy in four fractions (60 CGE).
Numerous single-institutional reports on proton-beam therapy similarly describe excellent 5-year local control in the range of 95% or greater (range 90.5%-99%).43,122–130 With 15-year follow-up, authors report local control to be maintained at 95%.124–125 At the UCSF–CNL treatment facility, more than 1000 uveal melanoma patients have been treated since 1994, and the dose we currently use is 56 Gy equivalent in four fractions over 4 consecutive days with comparable high local control rates. Overall survival at 5 years is approximately 80% across series (range 70%-88%), with small tumors ranging from 95% to 98%, medium from 80% to 86%, and large at 60%. Enucleation rate after proton therapy at 5 years is approximately 10% (range 0%-25%), with small tumors ranging from 2% to 3%, medium from 7% to 8%, and large from 22% to 25%.122–132 One author reports on a contemporary series of patients treated with current proton-beam technique who achieved enucleation rates of 0% for small, 0.3% for medium, and 10.5% for large tumors.132 The overall enucleation rate at 15 years is approximately 15%.125





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


