Loss of frontal lobe inhibition is the major reason why patients with dementia develop urinary incontinence.
Normal aging never causes urinary incontinence.
Detrusor hyperactivity is the most common cause of urinary incontinence in elderly men and women, accounting for 50% to 65% of cases.
Urinary incontinence is a late finding in patients with dementia; its early appearance should lead to suspicion of other causes.
In most cases, the diagnosis is made from the history.
Baseline laboratory tests include a urinalysis, urine culture, and serum blood urea nitrogen (BUN) and creatinine level.
Absolute dryness may not be a realistic goal.
For patients with dementia, prompted voiding can be helpful.
For women with severe stress urinary incontinence, early surgical referral may be indicated.
For excessive urine ammonia odor, chlorophyllin 100 mg daily may be prescribed.
Urinary Tract Infections
Enterococcus should be suspected in instrumented men and in patients with long-term indwelling catheters.
The diagnosis of urinary tract infection requires symptoms plus a positive urine culture.
Reports of “cloudy” or “smelly” urine do not count as symptoms.
Parenteral antibiotics need to be continued only until the patient is clearly improving, afebrile, and able to take an oral antibiotic.
Asymptomatic bacteriuria is not associated with the development of either hypertension or renal failure.
Urinary catheters may be a reasonable and compassionate choice for elders who are terminally ill or functionally very impaired.
Long-term catheters should be changed when obstructed or every 1 to 3 months.
Benign Prostatic Hyperplasia
Histologic prostatic hyperplasia affects up to 90% of men older than 85 years.
The most important part of the history is to quantitate the severity of the symptoms, using the American Urological Association Symptom Index (AUA-SI).
Therapy is chosen to address the patient’s predominant symptoms, not just to reduce the size of the prostate.
Tamsulosin is the clearly preferred α-blocker because it does not cause hypotension and is equal in efficacy to the nonselective α-blockers.
A few older men are not fit for operative intervention and would be best served by long-term urinary catheterization.
A single episode of urinary retention due to prostate hyperplasia does not mandate surgical treatment.
Prostate Cancer
More than two thirds of men older than 80 years have histologically proven prostate cancer, although only a tiny portion of these men die of this disease.
Prostate-specific antigen (PSA) is very prostate-specific but not cancer-specific.
Most older men choosing watchful waiting will do well, particularly if the Gleason grade is favorable and there is no evidence of metastatic disease.
Select men older than 70 or 75 years may occasionally be candidates for radical prostatectomy, although there is no clear evidence that the benefits outweigh the risks in this group.
Approximately 50% to 80% of men with prostate cancer treated with hormonal treatment will have a substantial benefit.
Urinary disorders are among the most common conditions faced by the geriatrician. This chapter examines the following: (i) Urinary incontinence, (ii) urinary tract infection, (iii) benign prostatic hyperplasia, and (iv) prostate cancer.
URINARY INCONTINENCE
Urinary incontinence is the involuntary loss of urine severe enough to cause social or health problems. The problem is often undiagnosed because patients may not voluntarily disclose their disability, clinicians may not ask or be comfortable with an evaluation, or multiple other serious conditions consume the attention of the clinician. However, most elders with urinary incontinence can be managed with a straightforward evaluation. Urinary incontinence is one of the fundamental syndromes of geriatrics. It is often caused by something remote from the bladder, such as dementia, pneumonia, or medications.1,2 As many as 15% to 30% of community-dwelling elders have some degree of urinary incontinence—the rate is always higher in women. The prevalence rises to more than 50% in nursing home patients. In fact, urinary incontinence is commonly a precipitating reason for nursing home placement. Families may tolerate wandering and providing support for feeding and dressing but urinating on the sofa may not be well tolerated.
Normal Aging
Normal aging never causes incontinence. Put another way, urinary incontinence is always pathologic and deserves evaluation. However, several aspects of normal aging of the genitourinary (GU) tract do predispose susceptible elders to developing incontinence. First, uninhibited bladder (detrusor) contractions become increasingly common as one ages. So if an elder with incontinence undergoes urodynamic testing and is found to have detrusor hyperactivity, this may not be the cause of the incontinence, but rather part of normal aging.
Second, fluid excretion through the kidneys is highest during the hours of recumbency at night because of high atrial natriuretic peptide levels, depressed antidiuretic hormone levels, and mobilization of dependent edema. This could lead to filling of the bladder and a need to urinate (nocturia), but it would not be a direct cause of incontinence.
Third, bladder capacity diminishes with age. Bladder capacity, defined as the amount of urine in the bladder when the person feels he or she cannot possibly hold another drop, progressively falls with aging.
Fourth, in men, the prostate grows with aging. This benign growth can encroach on the urinary sphincters, causing symptoms of outlet obstruction, such as poor urinary stream, dribbling, and a sensation of incomplete bladder emptying. However, if prostate growth is the cause of incontinence, it is not normal aging—it is benign prostatic hyperplasia, prostate cancer, or some other pathologic cause.
Fifth, also in men, urinary flow rate falls with advancing age. Normal flow rates in elderly men should exceed 20 mL per second. Urinary flow rates <10 mL per second are clearly abnormal and those between 10 and 20 mL per second are borderline. With hyperplasia of the median lobe of the prostate, the velocity of flow through the urethra decreases. This can be measured with a urine velocity meter, a piece of equipment normally found in a urologist’s office. A “poor man’s” flow estimate is described later in this chapter.
Urinary incontinence is not just a nuisance; it causes substantial morbidity, including rash, skin infections, urinary tract infection (UTI), restriction of activity, depression, social isolation, decreased sexual function, and falls. Pressure sores are not independently associated with urinary incontinence, once one controls for comorbidities. Probably the most important complication of incontinence is social isolation. For example, an elder may stop going to church and civic clubs because of the embarrassment of becoming wet in a public place. Although urinary incontinence can cause substantial morbidity, it is not independently linked to mortality risk.3
It is easy to overlook urinary incontinence, especially in elders with multiple medical problems. For example, an 83-year-old woman with congestive heart failure, renal insufficiency, and poorly controlled diabetes will be on numerous medications and require substantial monitoring. Despite this, her major functional problem may be urinary incontinence—this may be the one thing that is really limiting her life. As part of every comprehensive geriatric assessment, ask a screening question about incontinence. A good question is: “Do you have accidents, or leak, when you urinate?”
Pathophysiology
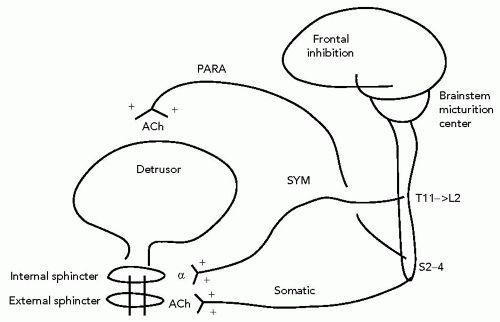
The bladder has two major functions—it needs to fill and it needs to empty3 (see Figure 15.1).
The bladder fills through relaxation of the detrusor muscle, with contraction of the bladder sphincters. The detrusor muscle is innervated by the muscarinic parasympathetic nervous system, which proceeds as a defined nerve from the second, third, and fourth sacral nerve roots. Any drug that is cholinergic will therefore contract the bladder (few drugs are cholinergic—e.g., bethanechol); any drug that is anticholinergic would relax the bladder (examples are legion and include antihistamines, antipsychotics, tricyclic antidepressants, and directly anticholinergic drugs).
The bladder sphincter is made up of two parts—the internal and external sphincters. The internal sphincter is innervated by the α part of the sympathetic nervous system. The sympathetic nerves to the internal sphincter arise from the thoracolumbar spinal cord (T11 through L2) and travel along blood vessels, ending in a well-defined bladder neck muscle. Any drug with α-agonist effect will therefore contract the internal sphincter. Examples of this are cold remedies such as pseudoephedrine (Sudafed) or the herb Ephedra. Any drug that is an α-antagonist will relax the sphincters. Examples of these drugs include the nonspecific α-blockers phentolamine or phenoxybenzamine and the α1-blockers prazosin, doxazosin, and tamsulosin.
The external sphincter is under voluntary muscle control. Therefore, it is innervated by a somatic nerve, with acetylcholine as the neurotransmitter. But this acetylcholine receptor is not a muscarinic (autonomic) cholinergic receptor but a nicotinic receptor. The typical anticholinergic drugs mentioned previously have no effect on this sphincter. Unfortunately, the voluntary sphincter cannot maintain continence for long because it requires constant active stimulation. It is mainly used to back up the internal sphincter (as when the bladder is very full and you must consciously “hold” your urine) or when the internal sphincter has been damaged (e.g., after prostate surgery).
So when the bladder is in filling mode, the sympathetic (α) system is on, keeping the sphincters contracted, and the parasympathetic (cholinergic) system is off, keeping the bladder relaxed. Actually, both systems are on, just to different degrees. When the bladder is filling, the sympathetic system dominates. This domination occurs at the level of the brainstem micturition center. This brainstem center regulates the balance of the autonomic nervous system—during the bladder’s filling phase, the micturition center turns up the adrenergic, sympathetic tone to the bladder’s neck and turns down the cholinergic, parasympathetic tone to the wall of the bladder, the detrusor muscle.
After the bladder fills to a significant extent, it switches to emptying mode. In this case, the brainstem makes a switch in autonomic tone—it revs up cholinergic transmission through parasympathetic nerves to the detrusor, to contract the bladder, and ramps down adrenergic transmission through sympathetic nerves to the internal sphincter. Therefore, the bladder contracts, the sphincters relax, and urine flows.
Note that the brainstem can do this without control by the cortex. In newborn infants, before the cerebral cortex becomes fully developed, the micturition center switches from filling to emptying mode as many as 20 times per day—therefore, 20 wet diapers. As the cortex develops, the final important part of the control of micturition develops—frontal lobe inhibition. The frontal lobes learn to tonically inhibit the micturition center, essentially keeping it in filling mode. Some readers of this text may at the moment have enough urine in the bladder to switch from filling to emptying mode, but their frontal lobes, below the level of consciousness, are telling the bladder not to because this would be socially inappropriate.
Loss of frontal inhibition is the major reason why patients with dementia and other neurodegenerative diseases develop urinary incontinence. In these patients, there is generally nothing wrong with the bladder, its innervation, the spinal cord, or the brainstem, but the frontal lobe loses function. Therefore, the patient loses the tonic frontal inhibition, and the body reverts to its primitive reflex form of urination—the micturition center simply switches from filling to emptying mode whenever an adequate amount of urine has been sensed in the bladder.
Remembering this functional anatomy makes the workup and treatment of urinary incontinence fairly straightforward.
Reversible Causes of Urinary Incontinence
After establishing the presence of incontinence, it is worthwhile to check for acute, reversible, transient causes of this condition. Table 15.1 lists several common causes, using the mnemonic “DIAPPERS.”3
Elders with delirium frequently have urinary incontinence. For example, a vigorous 86-year-old man, with no prior history of incontinence, is admitted to the hospital with lobar pneumonia, accompanied by fever, hyponatremia, mild dehydration, and urinary incontinence. In this case, the incontinence is almost surely due to the acute illness. An appropriate response would be to treat the underlying infection and reassess the incontinence after he has gone home and fully recovered.
Urinary incontinence is a common symptom in elders with symptomatic UTI. However, both asymptomatic bacteriuria and incontinence are very common, especially in frail, institutionalized elders, so their occurrence in the same patient is very likely to be a coincidence, not cause and effect. In new-onset urinary incontinence, or when incontinence suddenly worsens, it is reasonable to check for infection. One can generally wait for the urine culture and sensitivity, pick a simple antibiotic, and see whether clearing the infection helps the incontinence. If it does not, then the two are not related. Do not get in the endless game of treating every positive urine culture in incontinent patients—this does not help the incontinence and leads to predictable complications of chronic antibiotic therapy.
TABLE 15.1 CAUSES OF TRANSIENT INCONTINENCE IN THE ELDERLY
D
Delirium
I
Symptomatic urinary tract infection—asymptomatic bacteriuria has poor correlation with incontinence
Excessive urine output—hyperglycemia, hypercalcemia, treatment of CHF
R
Restricted mobility—musculoskeletal problems, inability to get to the toilet
S
Stool impaction
CHF, congestive heart failure. Reprinted with permission from Resnick NM. Geriatric incontinence. Urol Clin N Am. 1996;23:55-74.
Atrophic vaginitis/urethritis in elderly women can present with urinary incontinence, especially the stress or outlet incompetence type. Consider treatment with vaginal, transdermal, or oral estrogens, taking care to assess the overall appropriateness of hormone replacement in the woman (Evidence Level B). Even in an older woman with a uterus, however, intermittent vaginal estrogen (e.g., once or twice per week) to treat atrophy and incontinence is very unlikely to cause endometrial hyperplasia or other important side effects. However, the only large clinical trial of oral estrogens (Premarin) in postmenopausal women suggested that estrogen is ineffective (or even harmful) in all types of urinary incontinence.4
Many drugs can worsen urinary incontinence. Drugs with centrally acting sedative effect can remove the normal frontal inhibition. Examples include narcotics, sleeping medicines, alcohol, and antidepressants. Anticholinergic medications, including antihistamines and antipsychotics, may cause urinary incontinence by relaxing the detrusor muscle and causing bladder distension and overflow incontinence. Diuretics do not directly cause incontinence, but they can certainly make it worse through direct pharmacologic effects. Most diuretics should be dosed in the morning, so nocturia and nighttime incontinence is less of a problem. α-Agonists or blockers may interfere with proper functioning of the sphincters. Some chemotherapy agents (e.g., cyclophosphamide and vincristine) are toxic either to the bladder or the nerves supplying the bladder.
Depression is a major cause of urinary incontinence, as are other primary psychiatric disorders. Sometimes, incontinence can even be a tool used by patients to manipulate caregivers.
Rarely, polyuria is so excessive, usually from uncontrolled diabetes or hypercalcemia, that it may provoke urinary incontinence. And in hospitalized patients who receive several liters of intravenous hydration per day, one can expect incontinence, particularly when the patient is tethered to the bed with heart monitors, antithromboembolism leg pumps, oximetry devices, and so on.
A very common cause of acute (and chronic) urinary incontinence is impairment of mobility. A patient with severe osteoarthritis may simply not be able to move fast enough to get from the bed across the room to the bathroom and toilet. In cases like this, placing a portable commode next to the bed is a logical step, if the underlying disease cannot be adequately managed.
Finally, stool impaction can induce or exacerbate urinary incontinence. This is a particular problem in elders who take opiates for long term and in patients with dementia. The enlarging rectal ampulla may mechanically obstruct the bladder outlet and compress the bladder, causing detrusor overactivity.
Established Urinary Incontinence
Once the presence of urinary incontinence is verified, and transient causes have been eliminated, it is helpful to subdivide the incontinence into one of four major categories:
Detrusor hyperactivity (the bladder is too strong)
Detrusor underactivity (the bladder is too weak)
Outlet obstruction (the sphincter is too strong)
Outlet incompetence (the sphincter is too weak).
Combinations of these subtypes can also occur.
Detrusor hyperactivity (bladder too strong) is the most common cause of urinary incontinence in both elderly men and women, accounting for 50% to 65% of cases. Other common names for this type are urge incontinence, overactive bladder, or bladder spasms. Patients describe an abrupt sensation that urination is imminent. In many cases, no clear cause is found. The most commonly identified causes of detrusor hyperactivity are neurodegenerative diseases that affect the frontal lobes, thereby reducing or eliminating the normal frontal inhibition of the brainstem-spinal cord urinary reflex. Therefore, Alzheimer disease, Parkinson disease, and cortical stroke can cause urinary incontinence by reducing frontal inhibition, leading to uncoordinated detrusor hyperactivity. Incontinence should be a late finding in patients with dementia; its early appearance should lead to suspicion of other causes.
Other rare causes of detrusor hyperactivity are the “normal” increase in bladder contractions in patients who have urethral obstruction. Chronic cystitis, induced by radiation, interstitial disease, or chemotherapy, can cause bladder spasms. Finally, bladder stones or bladder cancer are irritating to the detrusor muscle, leading to detrusor hyperactivity.
Not all patients with an overactive bladder are incontinent. Many patients, especially women, have the intense sensation of urinary urgency, but they still have the mental and physical capacity to get to the bathroom in time. These patients can be assessed and treated like patients with actual urge incontinence.
Elders with detrusor hyperactivity have frequent moderate- or large-volume urine leakage, with leakage at night. The patient describes an intense desire to urinate, followed by a wet episode within a few seconds. Patients with dementia, of course, will not present with this sensation of urge but will simply have reflex incontinence. And in some cognitively intact patients, the urge is not felt, but incontinence still follows uninhibited bladder contraction. A neurologic examination should be normal, except perhaps for signs of frontal lobe release or other focal signs of cortical brain disease. The residual volume, if measured, should be normal.
A subset of patients with detrusor hyperactivity also has impaired bladder contractility, leading to incomplete emptying of the bladder. These patients may have an elevated residual volume.
Detrusor underactivity (bladder too weak) is uncommon. It is usually due to a neurogenic cause, such as disc compression, spinal cord tumor, surgical damage to nerves, or autonomic neuropathy (such as that caused by diabetes, alcohol, vitamin B12 deficiency, or syphilis). It can also result as the end stage of chronic outlet obstruction—initially the bladder would hypertrophy and be overactive, but as time progresses, the bladder stretches too far and becomes weak and dilated, with ineffectual contractions.
Elders with detrusor underactivity have frequent smallvolume leaks (overflow, hard to distinguish from primary outlet obstruction), rare nocturnal leakage, and possible loss of sacral reflexes or anal sphincter control, depending on the cause. Residual volume is high, and there are clinical symptoms of hesitancy, straining, and a sense of incomplete emptying. These obstructive symptoms are usually caused by outlet obstruction, but keep in mind rare causes of primary detrusor underactivity.
Outlet obstruction (sphincter too strong) is the second most common cause of urinary incontinence in elderly men, after urge incontinence. It is rare in women. It produces characteristic overflow incontinence, with dribbling, incomplete emptying, straining, and hesitancy. By far the most common cause of outlet obstruction is prostatism, either benign or malignant. Urethral strictures in men and, occasionally, a very large cystourethrocele or cervical or ovarian cancer in women are causes. Urinary leakage is nearly continuous and of low volume. Residual volume will be high, but neurologic tests should be normal.
Outlet incompetence (sphincter too weak) is the second most common cause of urinary incontinence in elderly women, after urge incontinence. It is usually of the stress incontinence type caused by intrinsic weakness, vaginal delivery, estrogen deficiency, or surgical damage. From 1% to 2% of men who undergo prostatectomy are left with wide-open outlet incompetence. Rarely, diabetes can be a primary cause of outlet incompetence. Hysterectomy and postmenopausal state may be weakly linked to an increased risk of outlet incompetence.
The characteristic pattern is daytime small leaks with any increase in abdominal pressure, such as with coughing, laughing, or straining. Leakage at night is rare. Residual volume should be low, unless urine pools in a large cystocele, and the neurologic examination is normal.
Workup
Evaluation of urinary incontinence in the elderly relies heavily on history. Indeed, in most cases, the diagnosis is made from history alone. Ask about the pattern of voiding, including onset of urinary incontinence, frequency, severity, and any precipitating or palliating factors. Use a 2- to 3-day voiding record (see Table 15.2) to quantitate and individualize this information. The patient urinates into a measuring cup inserted beneath the toilet seat. Ask about urine leakage at night and about any symptoms of outlet obstruction (hesitancy, dribbling, incomplete emptying).
As in all geriatric conditions, look at the big picture. Look for signs and symptoms of delirium, dementia, stroke, parkinsonism, cord or nerve root compression, and peripheral or autonomic neuropathy. Assess for evidence of functional impairment, and look at the patient’s general medical illnesses and medications. The history will usually lead to one of these major categories:
TABLE 15.2 BLADDER RECORD, OR VOIDING DIARY
Name:____
Date____/____/____
month day year
INSTRUCTIONS:
1. In the column “urinated in toilet,” make a mark every time during the 2-hour period you urinate into the toilet.
2. Use the next column “amount” to record the amount you urinate (or simply use a check mark if you are not measuring).
3. In the column marked “accident,” make a mark every time you accidentally leak urine.
4. In the last column, describe the reason for the accident. For example, if you coughed and leaked a small amount, write “cough—small amount.” If you had a large accident after a strong urge to urinate, write “urge—large amount.”
Time Interval
Urinated in Toilet
Amount
Accident (YES/NO)
Reason for Accident
6-8 AM
8-10 AM
10 AM-Noon
Noon-2 PM
2-4 PM
4-6 PM
6-8 PM
8-10 PM
10 PM-Midnight
Overnight
Number of pads used today:_____
Reprinted with permission from Agency for Healthcare Quality and Research. Urinary incontinence in adults. Clinical practice guideline, AHCPR Pub. No. 92-0038, Rockville, MD: AHRQ; March 1992.
URGE: large-volume leakage preceded by brief warning (seconds to minutes) → detrusor hyperactivity
STRESS: leakage only with increases in abdominal pressure → outlet incompetence
REFLEX: leakage without warning (“I am suddenly wet for no reason.”) → detrusor hyperactivity
Note: When urinary incontinence occurs immediately with an increase in abdominal pressure, this strongly suggests outlet incompetence and stress incontinence. When the increase in abdominal pressure is followed several seconds later by urinary leakage, urge incontinence is suggested. In this case, the abdominal pressure secondarily causes bladder spasm (detrusor hyperactivity), which then causes leakage.
Physical examination should be completed but rarely adds any information. One might confirm a distended bladder. Stress leakage can be duplicated by asking the patient to stand with a full bladder and then perform maneuvers increasing abdominal pressure. Rectal examination may demonstrate a fecal impaction, which itself can worsen urinary incontinence. In men, the prostate can be palpated, but prostate size correlates poorly with obstruction. One can also ask the elderly patient to voluntarily contract the anal sphincter, but at least 15% of normal elders cannot do this, so a negative result for this test is not helpful.
Pelvic examination can demonstrate laxity, such as a cystocele or rectocele, but these findings are rarely the cause of incontinence. Occasionally, a large cystocele may kink the urethra and cause outlet obstruction in women. Signs of atrophic vaginitis suggest estrogen deficiency and outlet incompetence. Finally, there is the Bonney (or Marshall) test—the bladder is pushed up, stabilizing the bladder base and preventing leakage caused by outlet incompetence. This test predicts whether surgery may cure the outlet incompetence.
Laboratory is also of limited usefulness, but in most cases, one should order a urinalysis, urine culture, and serum blood urea nitrogen (BUN) and creatinine level determination. If the urinalysis shows sterile hematuria, then one should move out of the incontinence algorithm and perform a structural workup, usually cystoscopy and some kind of upper tract imaging, such as spiral computed tomography (CT) scan. Urine cytology is only necessary if transitional cell carcinoma is suspected, such as in patients with hematuria. A positive urine culture may indicate UTI or asymptomatic bacteriuria; in select cases, give a trial of antibiotics and assess their effect on continence.
In suspected cases, a postvoid residual volume should be measured. Normal residual volume is <100 mL, and >200 mL is clearly abnormal. If the residual volume is abnormal, order a renal ultrasound to check for hydronephrosis. In men, it is usually safer and easier, although more expensive, to measure residual volume by ultrasonography than by urethral catheterization.
Men with obstructive symptoms should complete the American Urological Association Symptom Index (AUA-SI) (see Table 15.7). An ancillary test in these patients is a urinary flow rate, which is generally done in the urologist’s office. If polyuria is present, it is prudent to check the serum glucose and calcium levels to evaluate for causes of osmotic diuresis.
The diagnosis is generally clear from history, physical examination, and basic laboratory tests. If not, then the physician might consider referring the patient to a gynecologist or urologist who specializes in urinary incontinence. Unfortunately, even in severe cases, urodynamic testing is not likely to provide more precise diagnostic and therapeutic information.
Following these diagnostic suggestions leads to a diagnosis in most cases. Consider referral to a surgical specialist in the following cases: Marked pelvic prolapse, severe stress incontinence, marked prostate enlargement, suspicion of cancer, inability to pass a urinary catheter, residual volume >100 to 200 mL, recent pelvic surgery or radiation, sterile hematuria, recalcitrant symptomatic UTIs, and severe obstructive symptoms.
Management
In all cases, try to correct the underlying problem or precipitating factors. Accept that absolute dryness may not be a realistic goal, but a reduction in the number and severity of incontinent episodes is generally possible. Reducing the number of episodes by one or two per day can have a substantial impact on the daily lives of patients and their caregivers.
Realize that drugs have not been adequately tested in the elderly, particularly the sick elderly. Be very careful of drug side effects, and if a drug is not clearly effective, stop it.
Bladder training (habit training) can be useful in most causes of urinary incontinence, except in cognitively impaired elders (Evidence Level B). Ask the patient to void every 30 to 60 minutes; then progressively increase the duration between voids to every 3 to 4 hours. A night schedule is optional.5
For detrusor hyperactivity, start with pelvic muscle exercises (Kegel exercises; see Table 15.3). Although these were originally designed for outlet incompetence, when they are done correctly, the sphincter muscles contract and the bladder reflexively relaxes. However, if the exercises are done incorrectly (as is often the case), they can make the situation worse. Referral to a urinary incontinence therapist, usually in the occupational therapy department, can often help. These professionals will place a probe in the vagina of the patient and teach her how to contract and relax the correct muscles, using biofeedback. Several sessions of this training may substantially reduce or even cure incontinence6,7 (Evidence Level B).
Avoidance of caffeinated beverages, alcohol, and artificial sweeteners may improve symptoms.8
TABLE 15.3 KEGEL PUBOCOCCYGEUS MUSCLE EXERCISES FOR DETRUSOR HYPERACTIVITY OR OUTLET INCOMPETENCE
▪
Pull in or “squeeze” your pelvic muscles as if you were trying to stop urine flow or keep from passing gas
▪
To better feel the muscles to be contracted, attempt to stop the flow of urine while urinating
▪
Hold the contraction for several seconds
▪
Relax completely for a period as long as the contraction was held, then repeat
▪
Perform at least three sets of eight to ten contractions every day.
▪
Try to hold contractions for progressively longer times (from 1-2 s to 10 s, if possible)
▪
Improvement in bladder control may not be evident for 3 mo; keep exercising!
The most commonly used drugs are the bladder smooth muscle relaxants oxybutynin (Ditropan) or tolterodine (Detrol). Oxybutynin comes in immediate-release preparations (5 and 10 mg tablets) that are dosed twice daily. There is also a sustained-release product, oxybutynin (Ditropan XL) (5, 10, and 15 mg), which is dosed once per day. Finally, there is a transdermal oxybutynin product (Oxytrol patch, 3.9 mg) that is dosed twice per week.
Tolterodine (Detrol) may be slightly more bladder specific. It comes as immediate-release (1 and 2 mg) tablets, which are dosed twice daily, and a sustained-release product (Detrol LA, 2 and 4 mg), which is dosed once per day.9
There are three newer bladder relaxants: Trospium (Sanctura, 20 mg twice daily),10 darifenacin (Enablex, 7.5 to 15 mg daily),11 and solifenacin (VESIcare, 5 mg daily).12 These newer drugs may be more bladder specific, but there is no convincing evidence of increased efficacy. All the anticholinergic drugs for overactive bladder are only modestly more effective than placebo (Evidence Level A).
If these drugs do not clearly decrease the number and severity of incontinent episodes, they should be discontinued. If the physician is unsure whether the drug will be helpful, a limited trial is indicated. If, on the other hand, the physician is unsure whether the drug is really doing any good, then a trial off the drug is a good idea. Common side effects include dry mouth, constipation, blurred vision, and gastroesophageal reflux. Patients with dementia may become more confused. Side effects may be less common with the sustained-release products. All anticholinergic drugs can rarely precipitate urinary retention, especially if there is any degree of underlying outlet obstruction.
For patients with dementia, prompted voiding can be helpful.13 In this approach, the caregiver first completes a voiding diary to understand the pattern of incontinence episodes. Then, he or she approaches the patient at the appropriate time and asks, “Do you need help in going to the bathroom?” If the patient says yes, then the caregiver calmly helps. If the patient says no, the caregiver lets the patient know he or she is available if needed. If the patient still wets himself or herself, then calm cleaning, without scolding or belittling is needed. This “simple” maneuver may reduce the number of incontinent episodes by 50% or more. A randomized trial in nursing home patients with detrusor hyperactivity associated with dementia found that adding oxybutynin to a schedule of prompted voiding added no extra benefit in reducing incontinent episodes.14
A few other drugs have been suggested to help with detrusor hyperactivity, but their side effects generally preclude their use in the elderly, particularly the frail elderly. Drugs with doubtful efficacy include imipramine (Tofranil), dicyclomine (Bentyl), flavoxate (Urispas), and the strongly anticholinergic drug propantheline (Pro-Banthine).
An indwelling catheter, although it immediately prevents wetting, is not recommended. In addition to a substantially increased risk of urosepsis, the underlying bladder spasms often worsen because there is a foreign body in the bladder. Eventually in some of these patients, spasms increase to the extent that urine leaks around the catheter, leading to placement of a larger catheter and a vicious cycle.
Detrusor underactivity can be overcome with the Credé maneuver (physically pushing on the abdominal wall to encourage bladder emptying) or Valsalva maneuvers. In patients who are dexterous enough or who have capable caregivers, intermittent catheterization is an option. Another choice is to place an indwelling catheter for 2 to 4 weeks and then attempt discontinuation of the catheter to see whether the bladder has contracted down and regained some muscular tone. The cholinergic drug bethanechol (Urecholine) or the α-blocker phenoxybenzamine (Dibenzyline) often have too many side effects to be useful.
In patients with outlet obstruction, usually men, the appropriate first step is relief from the obstruction. This usually means surgery, as with a transurethral resection of the prostate (TURP) or dilation of a urethral stricture. In some patients, surgical repair is not possible or the patient may be at too high a risk for surgery. In these cases, long-term drainage of the bladder by an indwelling catheter is indicated. Choices include urethral or suprapubic catheters. The catheter should be meticulously maintained to avoid mechanical and infectious complications.
Drugs have little role in incontinence caused by outlet obstruction. An α-blocker such as phenoxybenzamine (Dibenzyline) or terazosin (Hytrin) or tamsulosin (Flomax), although indicated for obstructive symptoms of benign prostatic hyperplasia (BPH), are usually inappropriate if incontinence is present.
Finally, there are several effective treatments for patients with incontinence caused by outlet incompetence. For women with severe stress incontinence, early surgical referral may be indicated, either to urologists or to gynecologists with a special interest in this area. Short of surgery, pelvic floor exercises (Table 15.3), perhaps with a referral to an incontinence therapist who can use biofeedback, weight loss, and intravaginal weighted cones, are possibilities. In men, urinary incontinence following prostatectomy can be treated with a penile clamp, penile sheath, or condom catheter. In some women, pessaries may be helpful, but these must be changed frequently. Other possibilities for women include an artificial sphincter and polytetrafluoroethylene (Teflon) injections of the sphincter.
The major drug (for women only!) for outlet incompetence is estrogen. This can be given orally, transdermally, or vaginally, with the usual precautions. Some women may benefit from relatively low doses of vaginal cream given two or three nights per week (Evidence Level B). Paradoxically, recent studies suggest that estrogen replacement in postmenopausal women may actually increase the risk of urinary incontinence.4,15 Wide-open stress incontinence does not usually respond to estrogens and may require surgery.
Other drugs are not generally recommended in the elderly with outlet incompetence. α-Agonists (ephedrine or pseudoephedrine) may strengthen the urinary sphincter, but these drugs have too many vascular side effects. Anticholinergic drugs have been used to weaken bladder contractions, but this does not address the underlying problem.
In many cases, there will be treatment failures. For most elders, the incontinence will not be cured; it will be managed. Patients, families, and caregivers may need access to adult diapers such as Depends or Attends. These cost less than a dollar each, but if several are used per day, costs can be considerable. Patients may need launderable bed pads, and men may consider using external collection devices such as the sheath or condom catheters.
Only gold members can continue reading. Log In or Register to continue