Urethral carcinoma is a rare tumor with predominantly poor survival. Both the disease and its treatment can affect both sexual and urinary function. The natural history of urethral carcinoma varies, therefore the appropriate application of surgery, radiation, and chemotherapy remain unknown. Management of this disease remains driven by individual clinician experience and data derived from small case series. This article discusses the histology and anatomy of the male and female urethra, as well as their natural history. In addition, the epidemiology, clinical presentation, diagnosis, staging, treatment, and future directions of management of cancer arising in the urethra are addressed.
Key Points
- •
Outcomes of urethral cancer are heavily influenced by location, with distal (anterior) cancers presenting earlier and at lower stage with better chance of cure.
- •
Current epidemiologic data suggest that urothelial carcinoma (formerly called transitional cell carcinoma) is the most common diagnosis, and that men are affected more commonly than women. Recurrent lower urinary tract symptoms or persistent urethral stricture should warrant further urologic work-up including thorough physical examination, imaging of the lower urinary tract, and cystoscopy.
- •
Magnetic resonance imaging provides the best anatomic detail to define the local extent of urethral cancer in both men and women.
- •
Localized anterior tumors in both men and women may be managed primarily with endoscopic resection, segmental resection of the urethra, or partial penectomy in men. Radiation may represent an alternative in women or in cases in which surgical resection would negatively affect functional outcomes.
- •
Posterior tumors are best managed with multimodal therapy. Primary chemotherapy and/or radiation for locally advanced tumors based on histology should be considered, followed by endoscopic and radiologic assessment of response. In complete response, radiation (+/− radiosensitizer) could be considered for local control. For incomplete response, surgery with or without postoperative radiation (+/− radiosensitizer) should be considered. Systemic chemotherapy should be considered for metastatic disease.
- •
Rare tumor registries are needed to better optimize care for patients with rare cancers. Regionalization of care for rare cancers may improve outcomes.
Introduction
The differences in the anatomy and histology of the male and female urethra create challenges for the clinician in diagnosing and treating patients with urethral cancer. Gender, cause, location of the disease within the urethra, histology, and extent of the disease when it is diagnosed can strongly influence what treatment options are available to the patient, as well as the ultimate prognosis.
The difficulty in treating primary urethral cancer is multifactorial. Although the rarity of the disease has prevented prospective studies, the problem is more severe in that most data on treatment are derived from case studies and small case series. As such, it has been necessary to extrapolate treatment from different cancers and general oncologic principles to guide therapy. In addition, the morbidity of the disease and impact of treatment options on urinary and sexual function heavily influence treatment decisions and disease prognosis. There has been no research into the impact of the disease or treatment on quality of life. Perhaps the greatest limitation is that urethral carcinoma is not a single entity. The anatomy of the urethra makes treatment options different in men and women. Within gender, differences in where the tumor arises in the urethra influence histology, treatment options, and prognosis. Therefore, it is difficult to develop adequate experience considering the subtleties of these different entities to make progress in optimizing outcomes for patients with this disease.
This article first describes the anatomy of urethral cancer, which is critical in understanding the natural history of this disease. It also describes the epidemiology, possible risk factors, diagnosis, and staging of urethral cancer. Because of the rarity of this disease and lack of evidence guiding treatment, treatment is discussed using a case-based format with best practices and alternatives for each scenario. Our management of urethral cancer and review recent studies are also described. In addition, possible ways to improve treatment outcomes for this rare and challenging disease are discussed.
Introduction
The differences in the anatomy and histology of the male and female urethra create challenges for the clinician in diagnosing and treating patients with urethral cancer. Gender, cause, location of the disease within the urethra, histology, and extent of the disease when it is diagnosed can strongly influence what treatment options are available to the patient, as well as the ultimate prognosis.
The difficulty in treating primary urethral cancer is multifactorial. Although the rarity of the disease has prevented prospective studies, the problem is more severe in that most data on treatment are derived from case studies and small case series. As such, it has been necessary to extrapolate treatment from different cancers and general oncologic principles to guide therapy. In addition, the morbidity of the disease and impact of treatment options on urinary and sexual function heavily influence treatment decisions and disease prognosis. There has been no research into the impact of the disease or treatment on quality of life. Perhaps the greatest limitation is that urethral carcinoma is not a single entity. The anatomy of the urethra makes treatment options different in men and women. Within gender, differences in where the tumor arises in the urethra influence histology, treatment options, and prognosis. Therefore, it is difficult to develop adequate experience considering the subtleties of these different entities to make progress in optimizing outcomes for patients with this disease.
This article first describes the anatomy of urethral cancer, which is critical in understanding the natural history of this disease. It also describes the epidemiology, possible risk factors, diagnosis, and staging of urethral cancer. Because of the rarity of this disease and lack of evidence guiding treatment, treatment is discussed using a case-based format with best practices and alternatives for each scenario. Our management of urethral cancer and review recent studies are also described. In addition, possible ways to improve treatment outcomes for this rare and challenging disease are discussed.
Anatomy/histology
There are major differences between the female and male urethras. Anatomic differences give insight into the cause of the disease in some patients. These differences influence the underlying histology of urethral cancers by gender and also the patterns of disease spread. Understanding the anatomy and histology of the urethra also affects the selection of treatment with surgery (and type), radiation (and type), and chemotherapy (and regimen), including the use of multimodal strategies, which is often crucial in the successful management of the disease.
Female Urethra
The urethra extends from the bladder neck to the urethral meatus and measures from 3 to 5 cm ( Fig. 1 ). The urethra is surrounded by the anterior vagina posteriorly, the bladder superiorly, and the pubic symphysis anteriorly where the distal one-third of the urethra is fixed. Paired Skene glands insert on the urethra on either side. The proximal urethra closest to the bladder neck comprises predominantly transitional epithelium similar to the bladder and upper urinary tract. However, the female trigone has a greater tendency to develop squamous metaplasia as a normal variant, and thus the proximal urethra may have a percentage of cells with squamous features. The distal urethra has more squamous and glandular features predominated by nonkeratinized stratified squamous epithelium. The urethra is surrounded by a layer of smooth muscle. A layer of striated muscle surrounds the distal two-thirds or anterior urethra and is involved in conscious urinary control. Urethral mucosal coaptation as well as the bladder neck also contribute to urinary continence. These factors are important when considering partial resection of the urethra for localized tumors.
The blood supply to the urethra is from the internal pudendal artery and venous drainage is via the pelvic plexus. Lymphatic drainage for the distal (anterior) urethra is to the inguinal lymph nodes with the proximal urethra draining to the pelvic lymph nodes. This difference in drainage influences patterns of locoregional tumor spread.
Male Urethra
The male urethra extends from the bladder neck to the penile meatus and is divided into an anterior and posterior urethra ( Fig. 2 ). The posterior urethra extends distally from the bladder neck, and includes the portion of the urethra traversing the prostate (prostatic urethra) as well as the portion extending across the urogenital diaphragm (membranous urethra). The prostatic urethra is composed of transitional cell epithelium, whereas the membranous urethra is composed of stratified columnar cells. The anterior urethra includes the bulbar urethra and the penile urethra. The bulbar urethra is between the membranous urethra and the penile urethra, traverses most of the length of the penis, and is composed of columnar epithelium and pseudostratified cells. The most distal portion of the urethra (penile urethra) traverses the glans and is composed predominantly of stratified squamous epithelium.
The prostatic urethra is surrounded by the transition zone of the prostate. Paired ejaculatory ducts drain into the prostatic urethra at the verumontanum, which is in the middle of the prostatic urethra. This is the primary entry point of prostatic secretions, seminal vesicle secretions, and sperm into the urethra. Cowper glands are paired glands that drain into the membranous urethra. The glands of Littre are found on the dorsal surface of the pendulous urethra.
The arterial supply to the urethra comes from the paired bulbourethral arteries, which are branches of the internal pudendal artery. Venous drainage is into the deep dorsal vein of the penis and ultimately into the pelvic venous plexus. Lymphatic drainage from the urethra in the male is similar to that in the female, with the anterior urethra draining predominantly to the inguinal lymph nodes, and the posterior urethra draining to the hypogastric, internal iliac, and remaining pelvic lymph nodes.
Epidemiology
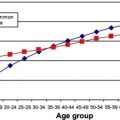
The historical assumption has been that urethral cancers are more common in women than in men. However, most of the literature has consisted of single-center case reports and case series, so there is an inherent bias in the literature toward reporting population(s) typically seen at tertiary care centers. To address this bias, Swartz and colleagues used the United States National Cancer Institute Surveillance, Epidemiology and End Results (SEER) database from 1973 to 2002 to identify patients with primary urethral carcinoma. This data source comprised 9 reporting centers from across the United States. They concluded that the commonly held belief was incorrect: 67% of all urethral cancers reported to the database (N = 1615 total cases) occurred in men. They also challenged the previously held assumption that squamous cell carcinoma was the most common histologic subtype. Their results showed that 55% of cases were urothelial carcinomas, 22% were squamous cell carcinomas, and 16% were adenocarcinomas. The remaining 5.3% of cases comprised rare (eg, melanoma [1.4%]) or unclassified entities (1.7%).
Another more recent epidemiologic study from the National Cancer Registry of the Netherlands confirmed that, even in women, urothelial carcinoma is the predominant cell type (45%), with adenocarcinoma being the second most common (29%), followed by squamous cell carcinoma (19%).
The incidence of primary urethral carcinoma during the study period in the study by Swartz and colleagues was 4.3 cases per million in men and 1.5 cases per million in women, with a higher incidence seen in African American men (5 cases/million). Adenocarcinoma was more common in African American women and squamous cell carcinoma was more common in African Americans than in American white people. The incidence of primary urethral carcinoma increased for all populations and histologic subtypes with advancing age (peak age 75–84 years) but the overall incidence of all forms of primary urethral cancer decreased during the study period, suggesting that this is becoming an even rarer cancer.
Clinical presentation
Primary urethral cancer can represent a diagnostic dilemma to the treating physician, leading to delays in diagnosis. Almost all men present with symptoms, and the presentation of a younger man (40s) with obstructive urinary symptoms should raise suspicion in the treating physician. Men typically present with symptoms of obstructive voiding symptoms, hematuria, and a palpable urethral mass. Although the cause is unknown, chronic inflammation is thought to be a primary driver in the development of urethral cancer. Up to 50% of men with urethra cancer have a history of urethral stricture disease and almost 25% report a history of sexually transmitted infections. Human papilloma virus 16 has been reportedly linked to the development of squamous cell carcinoma of the urethra.
In patients with a known preexisting diagnosis (eg, stricture, infection, urethritis), the diagnosis of urethral cancer can often be delayed because men continue to be treated based on the assumption that their symptoms are caused by the preexisting disease. In this setting, rapid recurrence of symptoms following treatment or worsening symptoms despite intervention should lead the clinician to investigate for the possibility of primary urethral carcinoma.
In men without a history of inflammation, the diagnosis is often delayed because the patient is treated for other more common causes such as benign prostatic hyperplasia (BPH) or urinary tract infection. Again, further investigation is warranted if a urinary tract infection recurs quickly or symptoms do not fully resolve. The initial diagnosis of BPH creates a greater challenge because, despite medical therapy, men often do not have improvement of their symptoms for 4 to 6 weeks; during this time, a masquerading urethral cancer can undergo disease progression. A thorough physical examination is necessary when evaluating this patient population. This examination should include a complete genital and rectal examination, as well as inspection and palpation of the perineum. Because the disease initially spreads by direct extension, palpation of the entire urethra as well as visual inspection of the urethral meatus is critical.
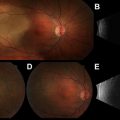
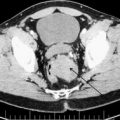
Roughly 98% of women with urethral cancer present with symptoms. Similar to men, women can present with urinary obstructive or irritating symptoms, hematuria, or a palpable mass. Many women are initially treated for a urinary tract infection because this represents the overwhelming cause of lower urinary tract complaints in women. Similar to urothelial cancer of the bladder in women, urethral cancer is often diagnosed late because of repeated treatment of urinary tract infections. There is a critical need to obtain a urine culture before treating women with lower urinary tract symptoms and hematuria. Absence of a positive urine culture or failure to resolve symptoms despite appropriate antibiotic coverage in women should prompt referral to urologist. Although stricture disease is less common in women, chronic inflammation or irritation in the form of infection, urethral polyps, caruncles, or urethral diverticula ( Fig. 3 ) can give clues to the presence of urethral carcinoma.
Thorough pelvic examination of women with persistent symptoms is important. A palpable mass can indicate a urethral cancer ( Fig. 4 ), diverticulum (see Fig. 3 ), or polyp. In addition, extension of urethral cancer to the vulva and anterior vaginal wall is common, and can be readily identified by a speculum examination.
Diagnostic studies
The diagnosis of urethral cancer requires a high level of suspicion for a primary urethral problem. Similar to urinary bladder cancer, diagnosis requires history and physical examination, laboratory evaluation, direct visualization, tissue diagnosis, and imaging to assess the local and systemic extent of the disease.
History should include a complete review of systems to elicit potential causes for the symptoms, prior urologic history and procedures, and history of prior radiation therapy for pelvic malignancies. Inquiry about the character, intensity, timing, frequency, and duration of urinary symptoms can be helpful. Constitutional symptoms related to malignancy, such as fatigue, weakness, fever, anorexia, night sweats, or cachexia, should be queried. History of medical comorbidities, family history of cancer, as well as immunosuppression is important. In addition, the history of other malignancies such as melanoma may raise suspicion for possible metastasis to the lower urinary tract. The use of quality-of-life instruments such as the American Urological Association symptom score and the Incontinence Symptom Index may add additional insight into the details of the urinary complaints and the extent to which they affect a patient’s life.
As stated earlier, a more extensive physical examination should be performed when common symptoms present in an unusual patient population or when there is persistence of symptoms despite appropriate treatment. In addition to a complete physical examination, a male genital examination should include direct visualization of the urethral meatus, palpation of the urethra and scrotal contents, inspection of the perineum, and a digital rectal examination. Bladder palpation can help identify urinary retention in patients with obstructing masses. Palpation of inguinal lymph nodes can identify lymphatic spread in up to one-third of patients.
Appropriate physical examination in women includes a bimanual examination, which includes assessment of the cervix, bladder, and urethra, and a speculum examination, which includes direct visualization of the urethral meatus and anterior vaginal wall. A protruding mass can occasionally be inspected. Women with urethral diverticula may have pain related to a stone, tumor, or infection within an obstructed diverticulum.
Laboratory studies are occasionally helpful, but should include a comprehensive metabolic panel including serum electrolytes, glucose, creatinine, urea, and liver function panel. A complete blood count as well as coagulation panel should be ordered in anticipation of potential endoscopy with biopsy. Urine microscopy and analysis can identify microscopic or gross hematuria that might lead to cystoscopy. Urine culture should be obtained in women, because urinary tract infection is still the most common diagnosis in women of all age groups with irritating voiding symptoms. The absence of a urinary tract infection in men or women with irritating voiding symptoms should lead to the consideration of cystourethroscopy using a flexible cystoscope. Urine cytology should be performed in all patients with gross or confirmed microscopic hematuria. Although the sensitivity of urine cytology for urethral carcinoma is low, if positive, it can reinforce additional evaluation with imaging as well as direct visualization with cystoscopy. Serum prostate-specific antigen (PSA) should be considered, especially if prostate cancer or prostatitis is in the differential diagnosis.
The next most frequent step is direct visualization of the urethra with a flexible cystoscope. For patients reporting poor emptying, an ultrasound scan to assess the postvoid residual may help identify urinary retention. Urinalysis can allow identification and treatment of a superimposed urinary tract infection before performing cystoscopy.
Before taking a patient to the operating room to confirm the diagnosis with tissue sampling, imaging should be performed. Most patients diagnosed during a hematuria evaluation have already undergone computed tomography (CT) urogram. This study is not adequate for assessment of the urethra (primarily because of poor soft tissue contrast resolution), but it is useful in detecting lymph node enlargement and visceral metastasis.
Magnetic resonance imaging (MRI) is typically the imaging modality of choice in the evaluation of patients with urethral cancer because, unlike CT, it provides exquisite soft tissue contrast. However, because this is a rare disease and the imaging protocols are nonstandard, image interpretation requires special expertise. Detailed descriptions of appropriate imaging protocols are beyond the scope of this article, but have been described in other reports.
In both men and women, MRI can assess the local disease extent, including extension into the corpora spongiosum or cavernosum in men, and involvement of the vagina in women. In addition, invasion of pelvic bones and adjacent organs (prostate and rectum) can be identified. In women who are suspected of having a urethral diverticulum, MRI can confirm the diagnosis, assess the location of the diverticulum, and help determine whether it contains neoplastic tissue.
Additional imaging studies should be directed to evaluate the presence of metastases. Depending on the degree of suspicion, chest radiograph or CT can be used to detect potential lung nodules. CT is more sensitive for lung nodules than chest radiography, but it carries a higher cost and greater radiation exposure. A radionuclide bone scan is indicated in patients with an increased serum alkaline phosphatase or serum calcium, or in patients with unusual bone pain or tenderness on palpation. Other imaging should be based on the patient’s history, suspicion that the urethral mass represents a metastasis instead of a primary malignancy, and/or underlying tumor histology. Although there is no strong evidence to support this for primary urethral cancer, CT of the brain should be considered in patients with small cell histology or neurologic symptoms/signs. CT positron emission tomography (PET) is generally not indicated for patients with primary urethral cancer, but may be useful if there is concern for metastases.
Cystourethroscopy is the most sensitive test for detecting cancer of the lower urinary tract. In patients with a presentation of gross or microscopic hematuria, a hematuria evaluation should include a urine cytology, CT urogram (assuming no contraindication), and visual inspection with cystoscopy. In patients with an obvious lesion in the lower urinary tract on CT urogram, visualization with flexible cystoscopy in the office can be skipped in favor of a rigid cystoscopy under anesthesia, which allows better visualization and the ability to confirm the diagnosis with biopsy. However, in the absence of an obvious mass, flexible cystoscopy in the office provides a sensitive means of identifying tumor within the lower urinary tract. Identification of mucosal irregularity, erythema, or friability warrants further investigation with a cystoscopy in the operating room under general anesthesia.
Under a general or regional (spinal) anesthetic, patients are placed in the dorsal lithotomy position and prepped and draped in the usual sterile fashion. Antibiotics are given to cover typical urogenital flora. Typically, a 22-French rigid cystoscope is introduced into the urethra and direct visualization of the mucosa is performed as the scope is directed toward the bladder. Flexible biopsy forceps can be introduced to biopsy concerning lesions. Hemostasis is achieved with Bugbee electrocautery. For early discrete tumors, a resectoscope with an electrified cutting loop can be introduced per urethra to completely resect the tumor. Care must be taken if the tumor appears close to the striated external sphincter in both men and women because aggressive resection can result in urinary incontinence. In the distal urethra of men, endoscopic resection can be challenging because of the limited working space in the urethra. In women, the shorter urethra creates greater risk of incontinence if aggressive resection is performed. Because many urethral cancers create and/or arise in the setting of urethral stricture(s), it is often not possible to directly visualize the entire urethra. In the setting of known urethral cancer, it is not advisable to dilate the urethra, because this may result in further pain, bleeding, and disruption of the tumor. In patients with associated urinary retention, tissue diagnosis should be combined with placement of a suprapubic catheter (if possible) to alleviate urinary tract obstruction. Optimal renal function is important for the delivery of systemic chemotherapy (when indicated) and urinary diversion is important in patients who are considered for organ preservation with radiation therapy.
A critical portion of the cystoscopy procedure is a physical examination under anesthesia. Patients with locally extensive or advanced disease are often difficult to examine in the office setting because of pain. Anesthesia allows careful inspection and palpation of the external genitalia and urethra to localize disease, which may be crucial in women with cancer arising in a urethral diverticulum because the tumor may not be visualized during endoscopy. In this circumstance, palpation with percutaneous biopsy may be the best way to obtain a tissue diagnosis.
A bimanual examination in women should include palpation of the anterior vaginal wall and pubic arch to assess tumor involvement. In men, a rectal examination can be used to assess involvement of the prostate as well as potential extension to involve the membranous urethra and pubic arch.
Palpation under anesthesia can also allow better assessment of inguinal lymphadenopathy. Enlarged nodes can sometimes be biopsied in the operating room under ultrasound guidance, particularly if there is concern that the urethral lesion may represent metastatic disease from another primary tumor.
Pathology and staging
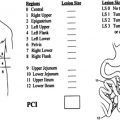
Results of the tissue diagnosis have implications for both treatment and prognosis. Similar to other cancers, grade and pathologic stage are obtained from the biopsy specimen and/or resection of the lesion. Combined with the examination under anesthesia and imaging results, the clinical stage can be assessed. Staging for primary urethral cancer is listed in Table 1 . As discussed later, staging is the primary factor influencing the type and extent of treatment.
| Primary Tumor (T) | |
| Tx | Primary tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| Ta | Noninvasive papillary, polypoid, or verrucous carcinoma |
| Tis | Carcinoma in situ |
| T1 | Tumor invades subepithelial connective tissue |
| T2 | Tumor invades corpus spongiosum, prostate, or periurethral muscle |
| T3 | Tumor invades corpus cavernosum, beyond prostatic capsule, anterior vagina, or bladder neck |
| T4 | Tumor invades other adjacent organs (eg, bladder) |
| Regional Lymph Nodes (N) | |
| Nx | Regional lymph nodes cannot be assessed |
| N0 | No regional lymph node metastasis |
| N1 | Metastases in a single lymph node, ≤2 cm in greatest dimension |
| N2 | Metastases in a single node >2 cm but ≤5 cm in greatest dimension, or in multiple nodes (≤5 cm) |
| N3 | Metastases in lymph node >5 cm in greatest dimension |
| Distant Metastases (M) | |
| Mx | Distant metastases cannot be assessed |
| M0 | No distant metastases |
| M1 | Distant metastases |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


