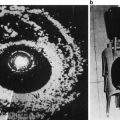
Fig. 1
Overall hospitalizations (a), hospitalizations with infection as primary diagnosis (b), and hospitalizations with noninfectious biopsy-related complications as primary diagnosis (c) within 30 days in biopsy (circles) and control (squares) groups. Reproduced with permission from [53]
Finally, when preoperative prophylactic antibiotics (trimethoprim-sulfamethoxazole or ciprofloxacin) were administered for 5,802 biopsy procedures, 200 patients (3.5 %) developed fever after biopsy and 27 (0.5 %) were hospitalized. Twenty-five of the 27 patients admitted to the hospital had signs of prostatitis and/or urosepsis [11].
Number and Patterns of Biopsy Cores
No study to date has identified significant differences in infection rates based solely on the number of core biopsies taken. Naughton et al. found no difference between 6 and 12 core biopsies in terms of fever or hospitalizations [20]. Furthermore, Berger et al. did not find significant differences when comparing patients who underwent 6, 10, or 15 core biopsies [12].
Preoperative Antibiotics
In 1998 Kapoor et al. studied the effects of ciprofloxacin prophylaxis on patients undergoing prostate biopsy by running a prospective, randomized, double-blind, multi-center study with 537 patients. They gave a 500 mg dose of ciprofloxacin to the study group and found that 6 ciprofloxacin recipients (3 %) and 12 placebo recipients (5 %) had clinical signs and symptoms of UTI (p = 0.15). Even more striking, none of the patients in the ciprofloxacin group were admitted to the hospital compared to four patients (2 %) in the placebo group who were admitted for febrile UTI after the biopsy [54]. Sabbagh et al. and Shigemura et al. both compared the use of fluoroquinolones as prophylaxis as a 1 day versus 3 day dose and found no significant differences in the rates of complications with duration of prophylaxis [55, 56]. Furthermore, a Cochrane review from 2011 concluded that there was no definitive proof that 3-day courses or multiple-dose courses of antibiotics are superior to 1-day courses or single-dose courses. The review also concluded that antibiotic prophylaxis is indeed effective in preventing infectious complications following transrectal prostate biopsy and should be widely used [57].
The AUA Best Practice Policy Statement recommends the use of a fluoroquinolone or 1st/2nd/3rd generation cephalosporin for a duration of less than or equal to 24 h as antibiotic prophylaxis for prostate biopsy. For patients with allergies, the alternative recommended first-line antibiotic is an aminoglycoside (can be substituted with aztreonam if there is renal dysfunction) plus metronidazole or clindamycin (Table 1) [58].
Table 1
Adapted from AUA Best Practice Policy Statement on Urologic Surgery Antimicrobial Prophylaxis (2008) (reviewed and validity confirmed 2011, updated February 2012)
Procedure | Organisms | Prophylaxis | Antimicrobial of choice | Alternative antimicrobial | Duration of therapy |
|---|---|---|---|---|---|
Transrectal prostate biopsy | Intestine | All | Fluoroquinolone 1st/2nd/3rd generation cephalosporin | Aminoglycoside (Aztreonam) + metronidazole or clindamycin | Less than or equal to 24 h |
Adibi et al. reported a rise in hospital admissions related to infection in their prostate biopsy patients who received ciprofloxacin or Bactrim DS prophylaxis. After the addition of a dose of gentamicin intramuscularly to their standard prophylaxis, the rates of hospitalization dropped from 3.8 % (11 patients among 290 biopsies) to 0.6 % (2 patients among 310 biopsies) [59]. Two different observational studies revealed that fluoroquinolones plus amikacin significantly decreased the rate of bloodstream infections compared to fluoroquinolone alone (0.3 % from 2.5 %, p = 0.003, and 1.7 % from 8.0 %, p < 0.001) [60, 61]. While utilization of various regimens of antibiotics may initially contribute to lower levels of infectious complications, caution must be taken in order to promote the development of antibiotic-resistant bacteria [62].
The AUA best practice statement also states that the risk of antimicrobial-associated adverse events related to prophylaxis for infectious endocarditis exceeds the benefit in genitourinary procedures. However, patients who have a history of prosthetic heart valves, previous infectious endocarditis, or certain forms of congenital heart disease may benefit from the addition of agents against enterococci such as amoxicillin or ampicillin [63].
Post-complication Antibiotics
Patients must be instructed that the development of fever, lethargy, difficulty voiding, testicular swelling, or symptoms suggestive of a urinary tract infection should be followed by an immediate call to their physician [49]. Signs or symptoms of sepsis should result in intravenous hydration as well as intravenous broad-spectrum antibiotics that cover E. coli, the most common cause of infectious complications following prostate biopsy. A urine culture should be obtained before the start of antibiotics, as well as blood cultures if the patient has a fever. When deciding on the broad-spectrum antibiotic to be employed, the physician must be aware that the bacteria responsible may be resistant to ampicillin and/or fluoroquinolones.
In a retrospective study of 1,273 patients who underwent prostate biopsy within the Veterans Affairs New York Harbor Healthcare System, 31 (2.4 %) patients presented with infectious symptoms within a month of the biopsy. Of these 31 patients, 23 had positive cultures, 18 of which were fluoroquinolone-resistant E. coli. The cultured E. coli also tended to have moderate to high resistance to ampicillin, trimethoprim/sulfamethoxazole, piperacillin, and gentamicin but were still susceptible to cephalosporins, ticarcillin/clavulanate, imipenem, aztreonam, tobramycin, and amikacin (see Table 2) [48]. Two additional studies, one from Israel and one from Egypt, found similar resistance and susceptibility patterns to these antibiotics, highlighting how widespread the antibiotic resistance problem has become [64, 65]. The authors of the Veteran Affairs study recommended empirical treatment with ceftriaxone, ceftazidime, or amikacin, antibiotics that they found to have 100 % susceptibility, until culture-specific therapy be implemented.
Table 2
Susceptibility of fluoroquinolone resistant E. coli to antibiotics in 18 samples (adapted from [48])
Antibiotic | % Susceptible |
|---|---|
Trimethoprim/sulfamethoxazole | 56 |
Ampicillin | 6 |
Ampicillin/sulbactam | 50 |
Peperacillin | 28 |
Ticarcillin/clavulanate | 94 |
Aztreonam | 94 |
Imipenem | 94 |
Cefazolin | 100 |
Cefotaxime | 100 |
Cefotetan | 100 |
Cefuroxime | 94 |
Ceftazidime | 100 |
Ceftriaxone | 100 |
Gentamicin | 78 |
Amikacin | 100 |
Tobramycin | 94 |
We have recently shown that immediate intervention by emergency department physicians can determine the eventual length of stay for a prostate biopsy patient with infectious complications. When we looked retrospectively at 17 patients who were admitted for infectious symptoms after having prostate biopsy with ciprofloxacin prophylaxis, we found that the patients who were given ceftriaxone by the emergency room personnel while in the emergency department were on average admitted for 2.8 days compared to 3.8 days for patients who were given an antibiotic other than ceftriaxone (p = 0.029) (unpublished results). A similar trend may occur in emergency departments that use other well-established antibiotics that are effective against fluoroquinolone-resistant bacteria such as amikacin and carbapenems [1, 48].
Preparation of the Patient Prior to Biopsy
Rectal Swab
Taylor et al. tailored pre-biopsy antibiotics for 112 patients undergoing prostate biopsy based on rectal culture results [66]. They compared the targeted prophylaxis group to a group of 345 patients who were not swabbed and received standard empirical ciprofloxacin prophylaxis. Of the patients who received targeted prophylaxis, 22 (19.6 %) grew fluoroquinolone-resistant organisms and none experienced an infectious complication. In the control group there were nine cases of infectious complications, seven of which were due to fluoroquinolone-resistant organisms and one of which was sepsis. Although the targeted antimicrobial prophylaxis resulted in a notable decrease in the incidence of infectious complications caused by fluoroquinolone-resistant organisms compared to empiric therapy, the difference was not statistically significant (p = 0.12).
Iodine Suppositories, Laxatives, Enemas, and Bowel Prep
While intuitively it would seem that cleansing the rectum before a biopsy would reduce the rate of infectious episodes, results supporting this notion are mixed. For example, Carey et al. reported no difference in the rate of hospitalization due to infections in patients who had a pre-procedure enema versus those who did not and the authors did express concern about the possible added cost and discomfort from enemas [67]. Similarly, Ruddick et al. sought to determine the benefits of enemas. In addition to an established antibiotic regimen that both groups adhered to, the first group had nothing by mouth starting at midnight the night before the biopsy. Group two, on the other hand, received nothing by mouth for 24 h before biopsy and underwent an enema the night before biopsy and another the morning of the procedure. The study found that the rate of infection in the first group of 190 patients was approximately 2.11 % (confidence interval, ±2.04 %). Of the 217 patients who underwent the enemas and the 24-h diet of clear fluids, only one case of sepsis was reported, resulting in a 0.46 % infection rate (confidence interval, ±1.32 %). The difference in infection rates was suggestive but lacked statistical significance (p = 0.189) [68].
Huang et al. performed a retrospective study in which all patients received the same antibiotics pre- and post-procedure. Patients in group 1 self-administered a phosphate enema the day before biopsy while patients in group 2 received a phosphate enema and rectal povidone-iodine on the day of the procedure performed by a doctor at the hospital. In group 1, 9.23 % were found to have a symptomatic infection with leukocytosis or chills while none were found in group 2 (p = 0.001) [69]. This study attributed the difference to the povidone-iodine preparation, but the difference could also be attributed to the timing of the phosphate enema (day before versus day of biopsy). Park et al. also looked at povidone-iodine preparation, but as a suppository. The group took cultures from the rectum before and after the suppository and found that the mean number of colony-forming units decreased 99.9 % after the rectal povidone-iodine preparation. The researchers administered a suppository to 360 patients, while 121 patients received none, with a resulting infectious complication rate of 0.3 % and 6.6 %, respectively [70].
Association Between Infection and Periprostatic Analgesia
Despite the extra injection sites that result from local anesthetic injection, no study has found an association with increased risk of serious infection [24, 26, 28, 30, 33]. However, Öbek et al. did report that the incidence of bacteriuria was significantly higher in the anesthesia group. High fever and hospitalization due to infectious complications were also more common in the local anesthesia group, although this was not statistically significant [71].
Risk of Repeat Biopsies and Infection
When Nam et al. examined the hospital admission rates for patients who underwent repeat prostate biopsy, the admission rates were not higher than those with first-time biopsies. However both groups did show an increase in the rate of infectious complications in recent years [10]. Similarly, a study of SEER and Medicare databases from 1991 to 2007 in which 13,883 men were identified who had undergone a single prostate biopsy and 3,640 who had undergone multiple biopsies showed no significant difference between their rates of hospitalization, serious urological infections, or noninfectious urological complications [72].
Risk of Erectile Dysfunction After Prostate Biopsy
In a study 211 men who were to undergo prostate biopsy, 7 % reported erectile dysfunction attributed to anxiety in anticipation of the procedure. In addition, up to 15 % of men who were potent prior to prostate biopsy reported erectile dysfunction at days 7 and 30 after the procedure. Taken together, a total of 42 patients who were previously potent reported acute erectile dysfunction either before or after the prostate biopsy. Of the 42 episodes of erectile dysfunction, only 21 were resolved by post-op day 30 [2]. Klein et al. also found a change in erectile function. Their study consisted of three groups of patients. The first group included men who received a saturation biopsy, where 20 biopsy cores were obtained. The saturation biopsy was performed after a previous negative prostate biopsy. Groups two and three both consisted of men who underwent 10 core biopsies, one of which received a periprostatic lidocaine injection. All three groups reported a statistically significant decrease in their International Index of Erectile Function (IIEF) score at the end of the first week. The decrease in IIEF score persisted into week 4 in the two groups receiving the 10-core biopsies. Notably, by week 12, there were no longer any significant decreases in potency for any of the three groups [8].
Fujita et al. found that an increased number of core biopsies as well as an increased number of biopsy procedures were associated with a decrease in Sexual Health Inventory for Men (SHIM) score (p = 0.04 and p = 0.02, respectively). Fujita et al. also found that patients without preexisting erectile function (SHIM score 22–25) had a steeper decrease in SHIM score after three or more biopsies compared to men with mild to moderate erectile dysfunction (SHIM score 8–21) [73].
The potential reasons for transient erectile dysfunction are debatable and remain uncertain. From a physiological standpoint, erectile dysfunction may be secondary to anatomical disruption of the neurovascular bundle or nerve compression from a hematoma or edema [2]. Beyond the impact of the physical effects of the biopsy there are certainly possible psychological causes of erectile dysfunction in men concerned over the potential diagnosis of a prostatic malignancy.
Voiding Dysfunction
Zisman et al. performed a study looking at 204 patients who voided via urethra at biopsy. The average number of cores taken was 8.4 ± 1.7. The group noted that 52 (25 %) of patients reported subjective voiding impairment on post-op day number 7, including 12 % who rated the difficulty as mild (1–2 points on a 0–5 scale), 8 % as moderate (3/5), and 5 % as severe (4–5/5). Five patients (2.5 %) went into acute urinary retention that required a urethral catheter for relief. Patients with a transitional zone volume greater than 42 ml were at a significantly higher risk of acute urinary retention (p = 0.03). Finally, patients with a baseline International Prostate Symptom Score (IPSS) greater than 20 points reported an increase in their IPSS on post-op day 7 [9].
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


