The classification applies to epithelial tumours of the thymus, including thymomas, thymic carcinomas, and neuroendocrine tumours of the thymus. It does not apply to sarcomas, lymphomas and other rare tumours.
There should be histological confirmation of the disease and division of cases by histological type.
Regional Lymph Nodes
The regional lymph nodes for thymic tumours extend from the cervical region to the diaphragm. The lymph node mapping is performed according to the ITMIG/IASLC thymic nodal map.1
The regional lymph nodes are the anterior region (anterior mediastinal and anterior cervical) lymph nodes, the deep region (middle mediastinal lymph nodes and the deep cervical lymph nodes).
Notes
Clinical stage classification:
The reliability of the imaging techniques in assessing involvement of the adjacent structures mostly relies on the radiologist’s best judgement. Standard report terms for CT scan by ITMIG are available.2
Any lymph node ≥ 1 cm in short axial dimension or with PET uptake (when available) should be considered involved for clinical staging and worth being removed at surgery.
Pathological stage classification:
Specific attention should be paid by the surgeon to the intraoperative marking, orientation and handling of the surgical specimen. Also, standard report terms for the description of the surgical and pathological findings are encouraged. Recommendations by ITMIG for the handling of the surgical specimen and reporting of the surgical/pathological findings are available.3
Correlation between clinical and pathological staging:
Analysis of the literature indicates that the correlation between clinical and pathological stage in thymic epithelial tumours is only moderate, with more frequent upstaging than downstaging, particularly for thymic carcinoma.
The most controversial areas are the involvement of major mediastinal structures, the identification of pleural/pericardial nodules and lymph nodal involvement.
Although some imaging characteristics have been found to correlate either with the lack of invasion or the presence of invasion of mediastinal structures (Stage III), the reliability of these features is only moderate, with an error rate ranging from 20% up to 50%. Similarly, the reliability of identifying pleural/pericardial nodules (particularly if small), the involved lymph nodes (most are reactive) and the pulmonary nodules (the majority are benign) is limited.
A detailed description of the CT findings predictive of invasiveness in thymoma is available.4
Notes
1 Bhora FY, Chen DJ, Detterbeck F. et al. (2014) The ITMIG/IASLC thymic epithelial tumors staging project: A proposed lymph node map for thymic epithelial tumors in the forthcoming 8th edition of the TNM classification of malignant tumors. JTO 9:S88–S96.
2 Marom EM, Rosado‐de‐Christenson ML, Bruzzi JF, et al. (2011) Standard report terms for chest computed tomography reports of anterior mediastinal masses suspicious for thymoma. JTO 6:S1717–S1723.
3 Detterbeck F, Moran C, Huang J, et al. (2011) Which way is up? Policies and procedures for surgeons and pathologists regarding resection specimens of thymic malignancy. JTO 7: S1730–S1738.
4 Marom E, Milito M, Moran C, et al. (2011) Computed tomography findings predicting invasiveness of thymoma. JTO 6(7):1274–1281.
TNM Clinical Classification (cTNM)
T – Primary Tumour
TX
Primary tumour cannot be assessed
T0
No evidence of primary tumour
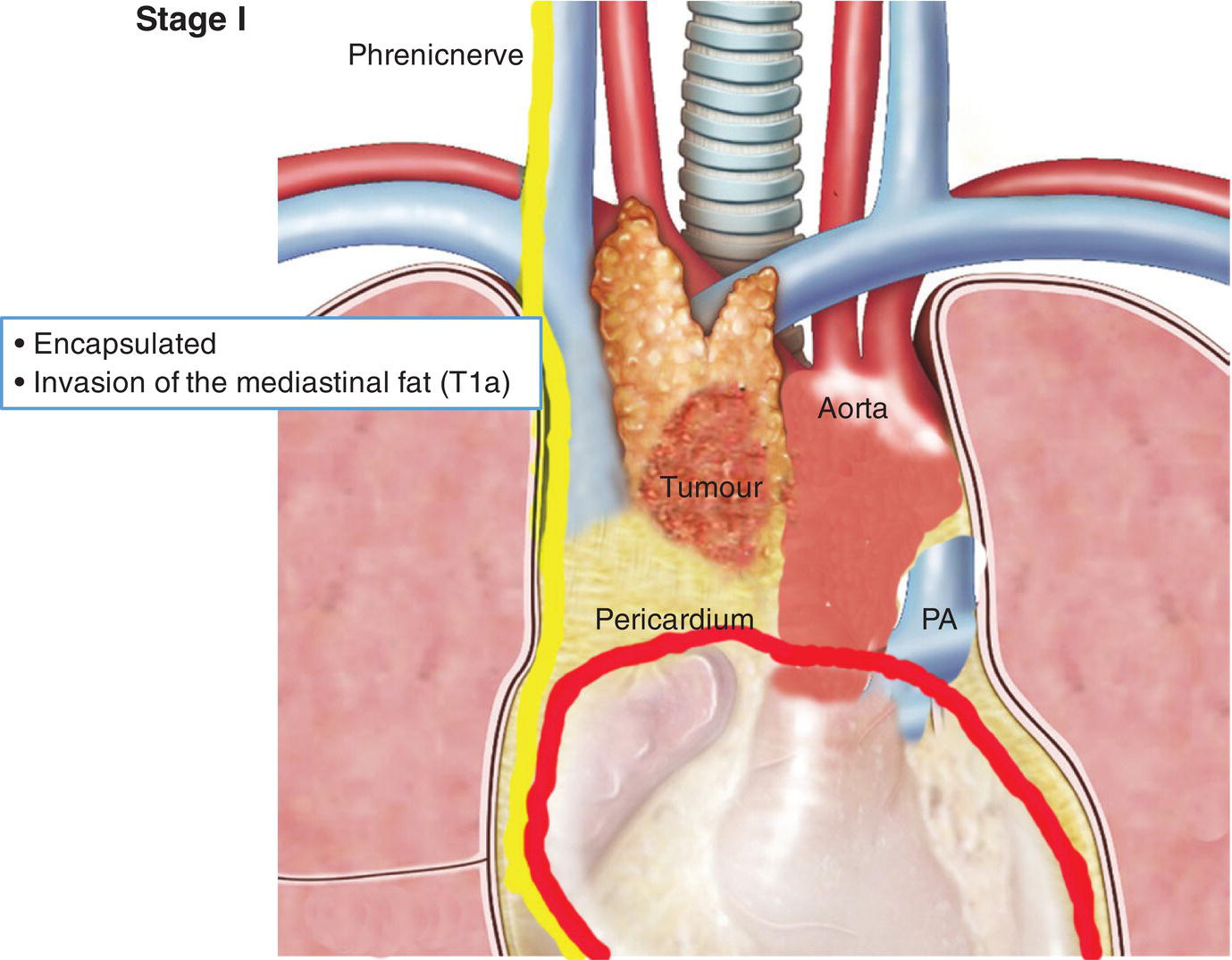
T1
Tumour encapsulated or extending into the mediastinal fat, may involve the mediastinal pleura
T1a
No mediastinal pleura involvement
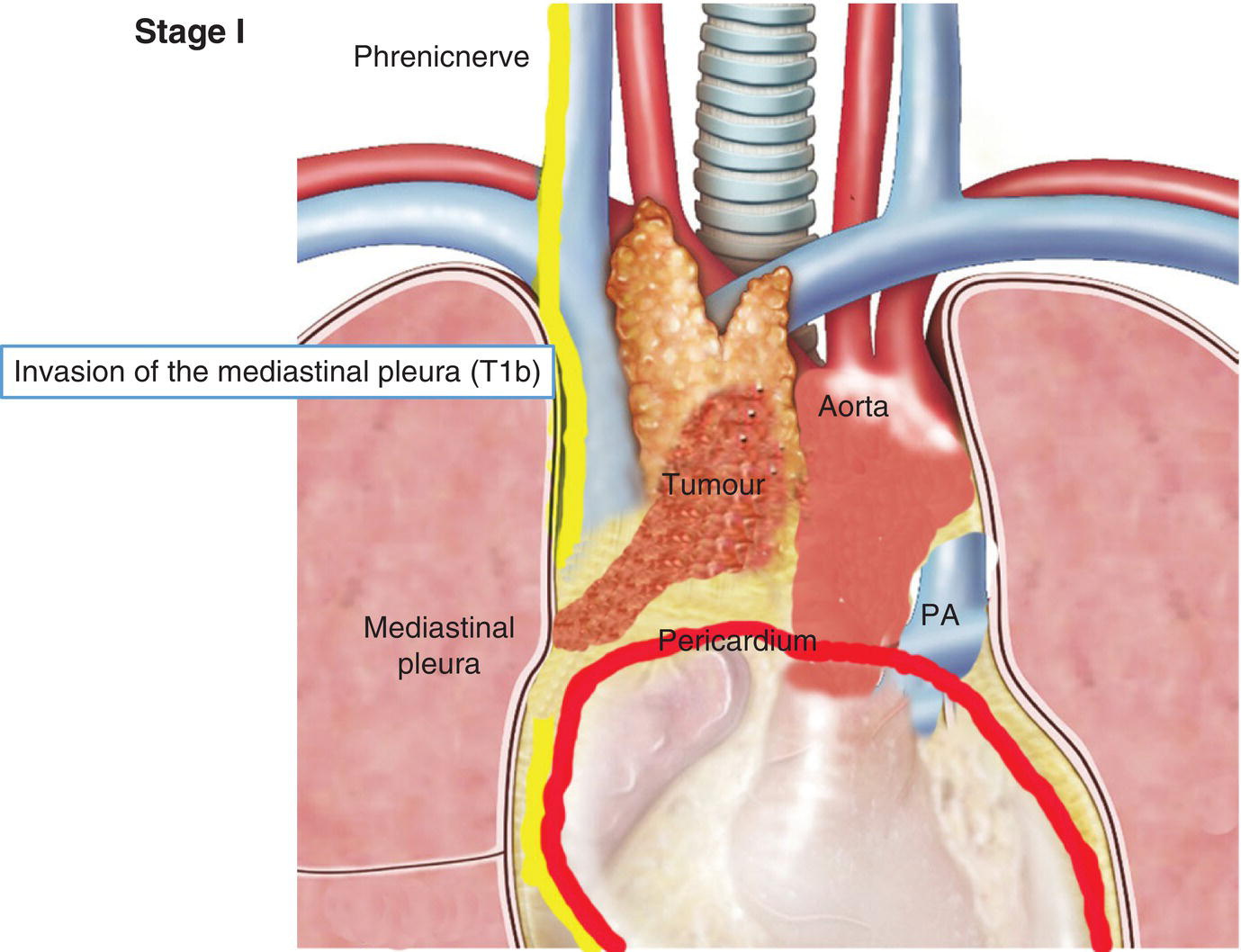
T1b
Direct invasion of the mediastinal pleura
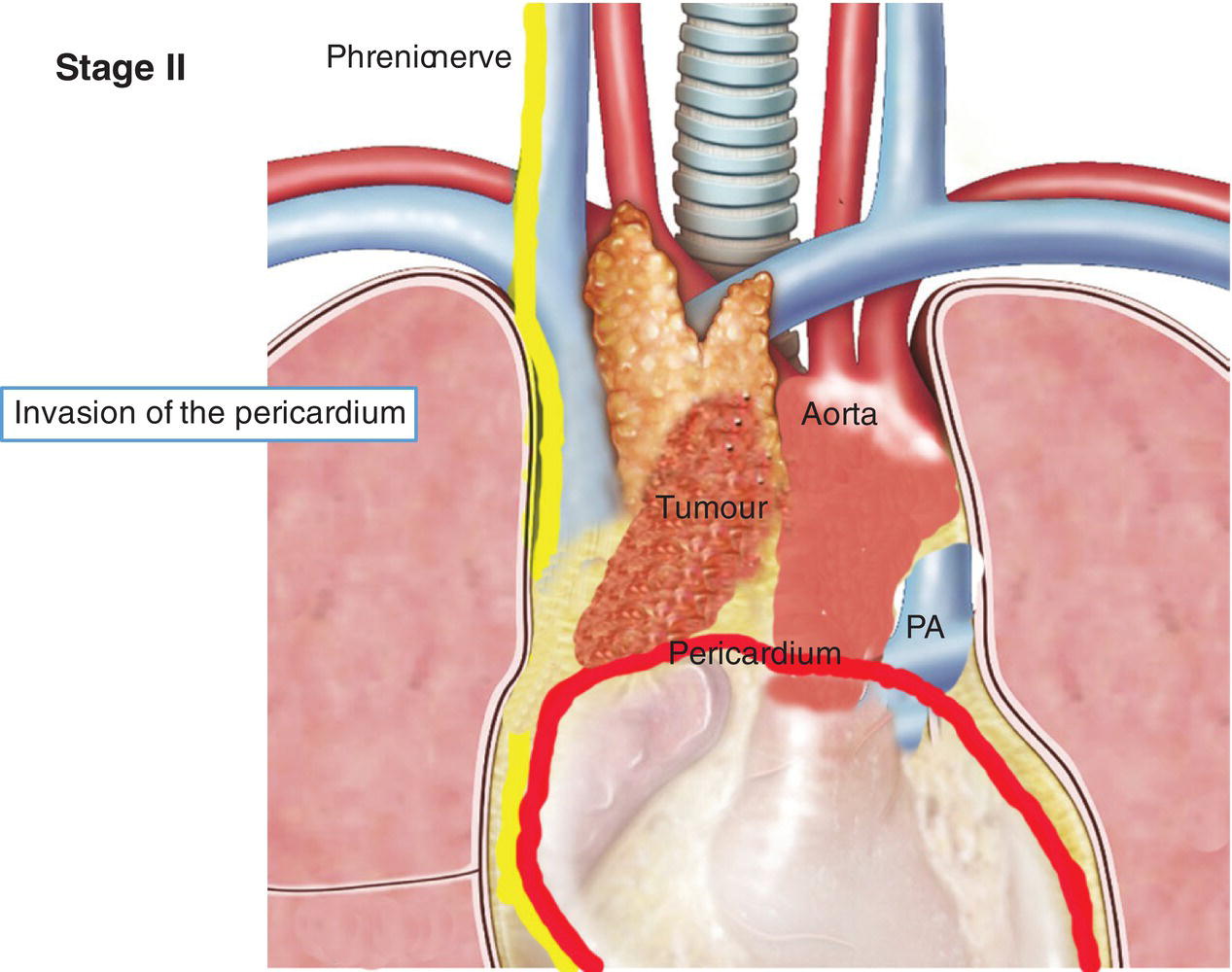
T2
Tumour with direct involvement of the pericardium (partial or full thickness)
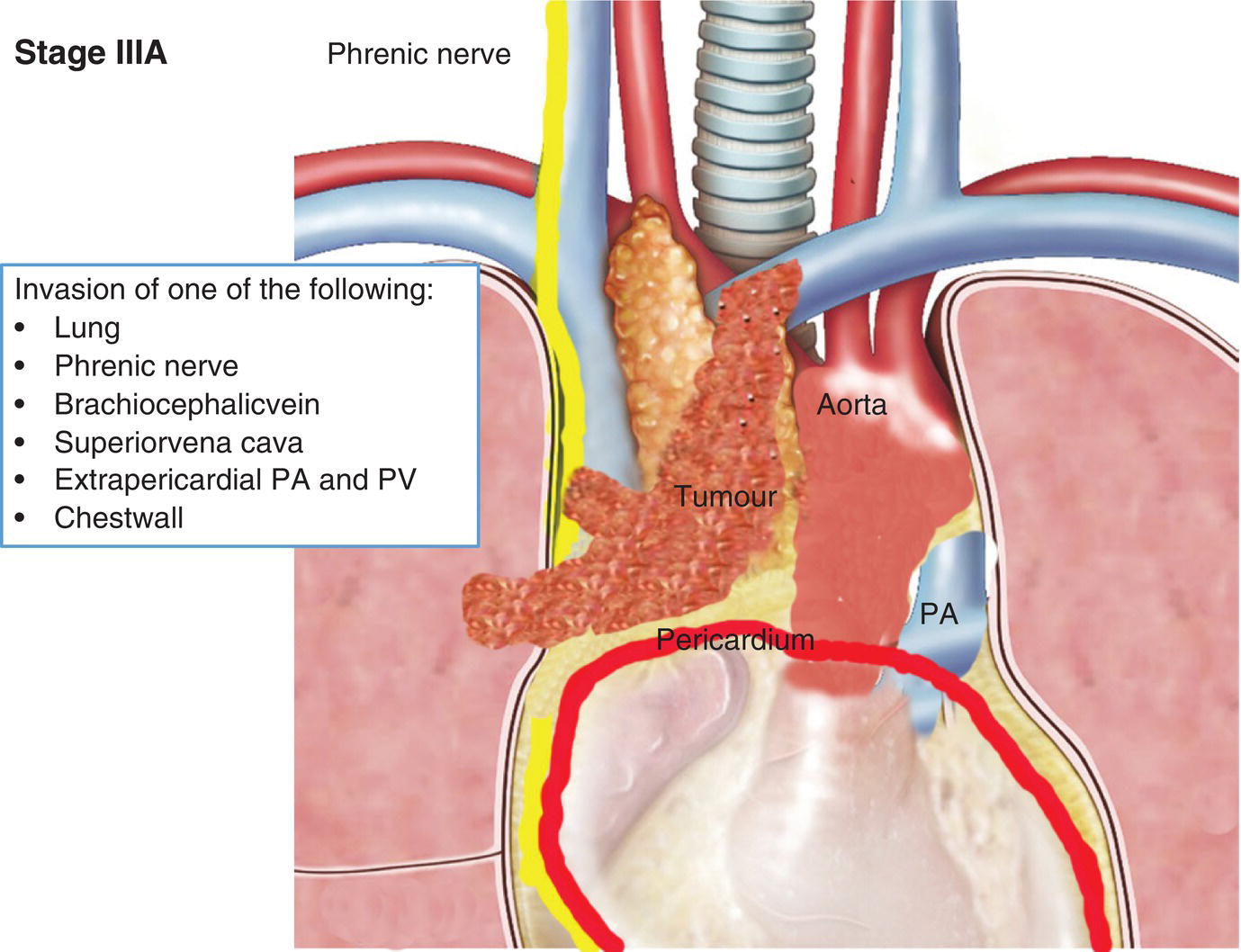
T3
Tumour with direct invasion into any of the following:
Lung
Brachiocephalic vein
Superior vena cava
Phrenic nerve
Chest wall
Extrapericardial pulmonary artery or vein.
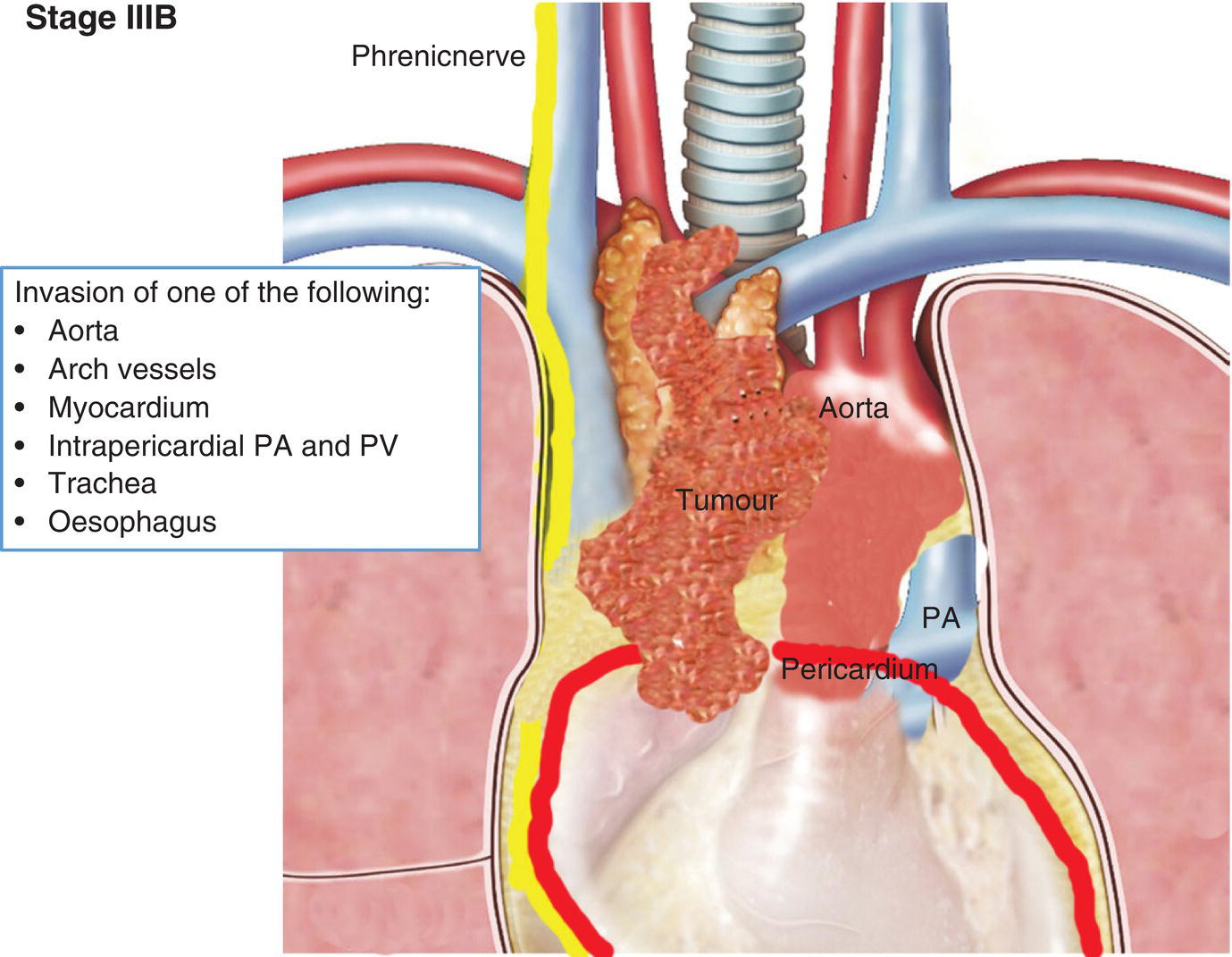
T4
Tumour with direct invasion into any of the following:
Aorta (ascending, arch, or descending)
Arch vessels
Intrapericardial pulmonary artery or vein
Myocardium
Trachea
Oesophagus
Notes
For pathologic T classification involvement of any structure should be microscopically confirmed. Adhesion of the tumour to an adjacent structure identified by the surgeon should not be considered for the T classification.
The T category is determined by the level of involvement. The T category is assigned to the highest level of involvement, regardless of involvement of structures of a lower level.
Direct invasion of the lung and the pleura is assigned to the T category and should be distinguished from separated lung and pleural nodules (see M category).
N – Regional Lymph Nodes
NX
Regional lymph nodes cannot be assessed
N0
No regional lymph node metastasis
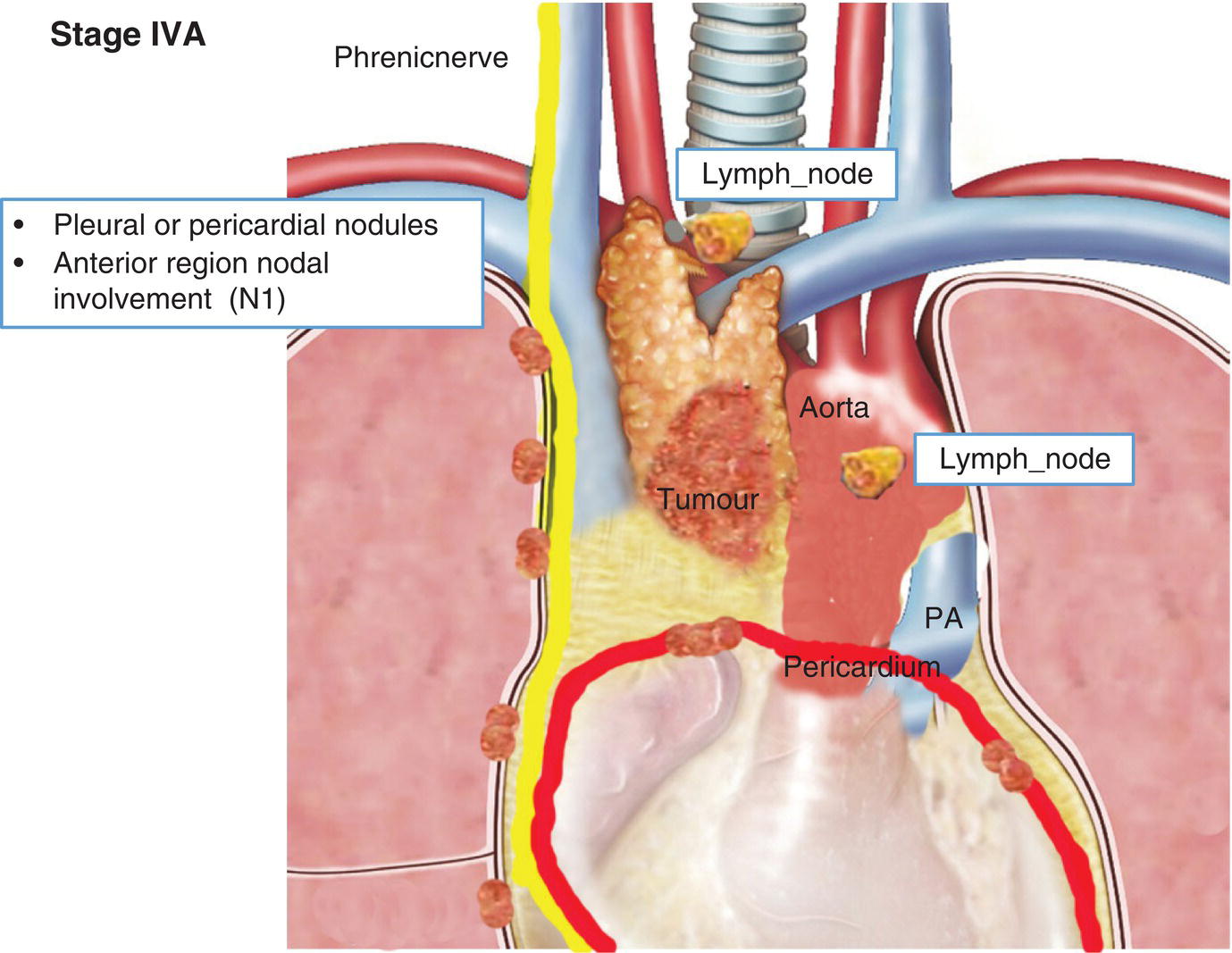
N1
Metastasis in anterior (perithymic) lymph nodes
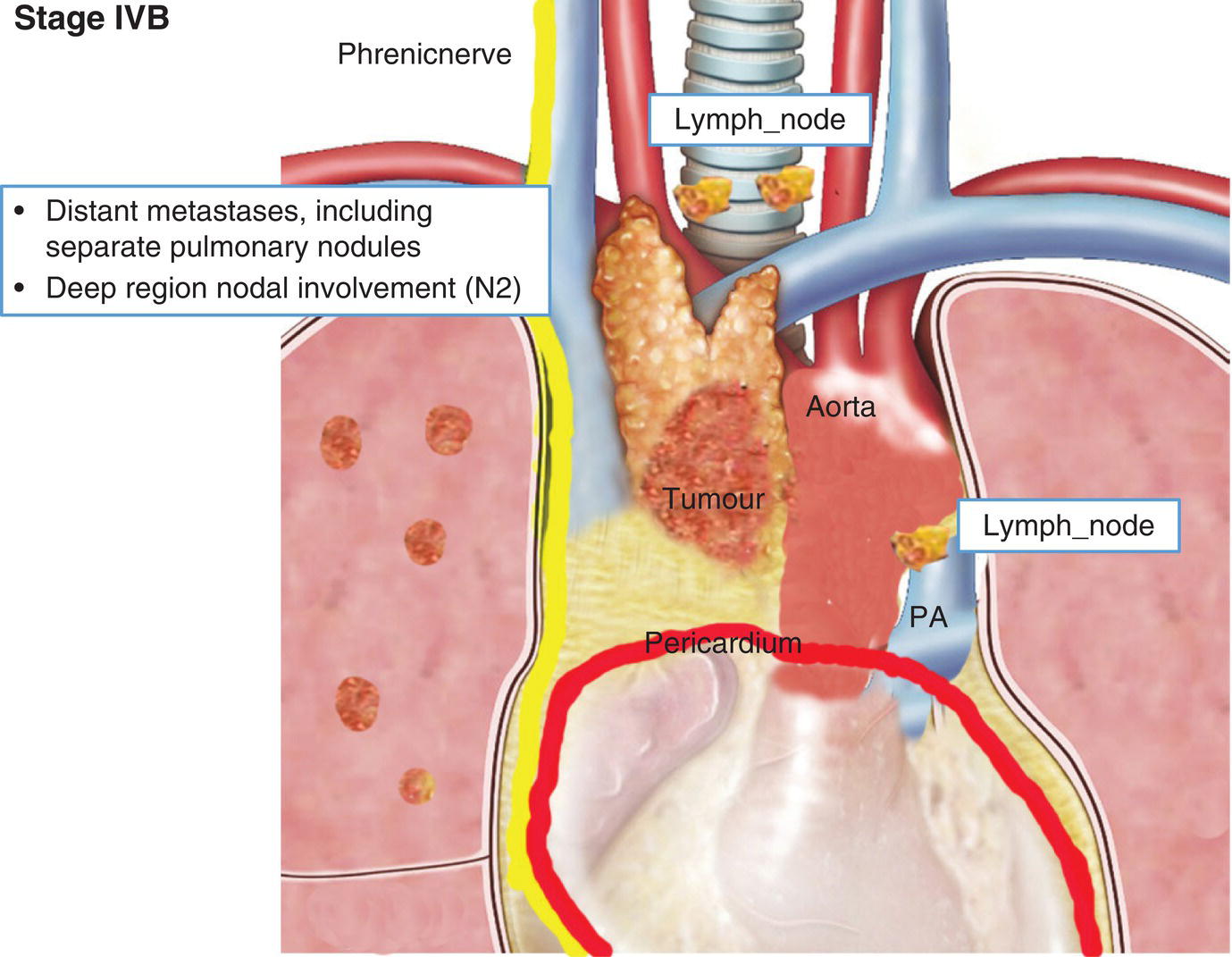
N2
Metastasis in deep intrathoracic or deep cervical lymph nodes
Notes
Direct extension of the primary tumour into a lymph node is considered as nodal involvement.
Lymph node dissection or sampling during resection of thymic tumours is strongly recommended, and the pathologists should specifically examine and report on the presence of nodal involvement. ITMIG/IASLC recommendations for lymph node dissection are as follows:◦
Any suspicious lymph node at surgery or at preoperative imaging should be removed.
For T1–T2 thymomas removal of adjacent nodes and anterior mediastinal nodes.
For >T2 thymomas systematic anterior mediastinal node dissection and sampling of deep mediastinal appropriate areas (paratracheal, aortopulmonary).
For thymic carcinomas a systematic sampling of N1 and N2 regions according to the ITMIG/IASLC nodal map (anterior mediastinal, intrathoracic, supraclavicular and lower cervical lymph nodes).
M – Distant Metastasis
M0
No pleural, pericardial or distant metastasis
M1
Distant metastasis
M1a Separate pleural or pericardial nodule(s)
M1b Distant metastasis beyond the pleura or pericardium, including separate pulmonary nodules
Notes
Pleural or pericardial nodes that are completely separated from the primary tumour are to be classified as M1a.
Lung nodules that are surrounded by normal parenchyma (and not in direct extension to the primary tumour) are to be classified as M1b.
TNM Pathological Classification (pTNM)
The pT, and pN categories correspond to the T and N categories.