Primary tumors in the trachea are relatively uncommon, with an estimated 2.7 new cases per million per year. The rarity of these tumors and their subtle clinical presentation require surgeons to have a high index of suspicion particularly with specific clinical presentations. Patients with a tumor of the trachea will present with a range of symptoms, including dyspnea on exertion and inspiratory wheezing, with a normal chest radiograph. Frequently, these patients will be diagnosed and treated as adult-onset asthma long before further investigations determine the presence of an obstructing tumor of the trachea.
This chapter will review the surgical anatomy of the cervical trachea, clinical presentation and diagnostic evaluation of patients with tumors of the cervical trachea, and anesthetic and surgical approaches to both resection and reconstruction of the cervical trachea. It will also review the role of nonsurgical organ preservation approaches and the role of adjuvant therapy in the management of malignant tumors of the upper airway.
The surgical approach to tumors involving the cervical trachea differs from the approach used for tumors of the distal trachea or carina. Although this chapter is directed toward the special problems of the cervical trachea, generalizations must be made from the total experience with tumors of the trachea.
SURGICAL ANATOMY OF THE TRACHEA
The trachea begins at the lower border of the cricoid cartilage and terminates where the lateral walls of the right and left main bronchi flare out from the lower trachea. The carinal spur is useful as a definite landmark for the termination of the trachea because it is clearly seen both bronchoscopically and radiologically. The average adult human trachea measures 11 cm in length with slight variation in proportion to the height of the individual.1 There are approximately two tracheal cartilaginous rings per centimeter of trachea. With the exception of congenital tracheal stenosis with circumferential rings of the trachea, the cricoid is the only completely circular cartilage in the upper airway.
Direct access to the trachea in the neck is of critical importance both for surgical access and for ease of reconstruction following resection. In young people, hyperextension of the neck frequently delivers in excess of 50% of the trachea into the neck.2 However, in an aged, kyphotic individual, even the most vigorous hyperextension may fail to deliver any of the trachea into the neck. The anatomic position of the trachea changes from an essentially subcutaneous position at the level of the cricoid to a prevertebral position at the level of the carina; thus, the course of the trachea is normally caudad and dorsal.
The blood supply of the trachea is of critical importance in resection and reconstruction of the trachea. The upper trachea is supplied primarily by branches of the inferior thyroid artery, and the lower trachea is supplied by branches of the bronchial artery, with contributions from the subclavian, supreme intercostal, internal thoracic, and innominate arteries. These vessels provide branches anteriorly to the trachea and posteriorly to the esophagus. They have a perforating pattern that arrives at the trachea from its lateral aspect. The longitudinal anastomoses between these vessels are fine, and transverse intercartilaginous arteries branch ultimately into a submucosal capillary network.2,3,4 Excessive division or dissection of these lateral perforators during circumferential dissection of the trachea risks disruption of this network and may lead to devascularization of trachea segments and a failed anastomosis.
The trachea is also intimately related to several critical structures. These include the recurrent laryngeal nerves, the esophagus, and the thyroid gland. Detailed knowledge of these anatomic relationships is essential before attempting any ablative or reconstructive surgery on the cervical trachea.
EVALUATION OF PATIENTS
Symptoms of a tumor in the trachea, even in the presence of a high degree of airway obstruction, may be insidious. Most commonly, patients with a tumor in the trachea present with any of dyspnea, hemoptysis, cough, wheezing, dysphagia, change hoarseness, stridor, and pneumonia. In one series, productive cough and shortness of breath were the most common symptoms. A history of slowly progressive dyspnea on exertion is often present.5 Many patients with a malignant neoplasm will present with hemoptysis often leading to an appropriate bronchoscopic diagnosis. An irritative cough, which may or may not be productive and which may in time be associated with hemoptysis, is sometimes also seen. Change in vocal quality as a result of involvement of one or both recurrent laryngeal nerves is not uncommon and may be insidious in onset. Stridor as a presenting symptom is often reflective of a late presentation of disease. All too often, especially with slowly growing tumors such as adenoid cystic carcinoma, the patient who has developed slowly progressive shortness of breath and wheezing will have an apparently normal chest radiograph. This leads to the diagnosis of adult-onset asthma, with some patients treated with steroids for a prolonged period of time before the slowly growing tumor is discovered.
In general, the more aggressive tumors are diagnosed earlier owing to their propensity to present with prominent symptoms, for example, hemoptysis. In one study, the mean duration of symptoms before diagnosis in patients with squamous cell carcinoma (SCC) of the trachea was 4 months, whereas the mean duration of symptoms before diagnosis in adenoid cystic carcinoma of the trachea was 18 months.
DIAGNOSTIC STUDIES
The primary diagnostic modalities for delineating tracheal abnormalities are radiologic studies and laryngoscopy and bronchoscopy.
The following investigations are helpful:
Chest radiograph (posteroanterior, lateral, and oblique) centered high enough to obtain good views of the trachea.
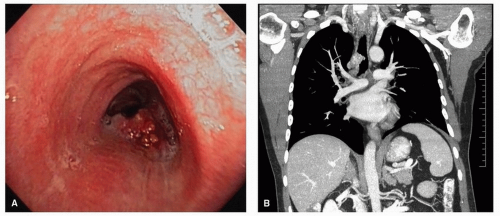
Computed tomography (CT), with multiplanar reconstruction is the gold standard for assessing extent of disease and defining extratracheal involvement as well as detecting the presence of lymph node involvement6(Fig. 17.1A and B).
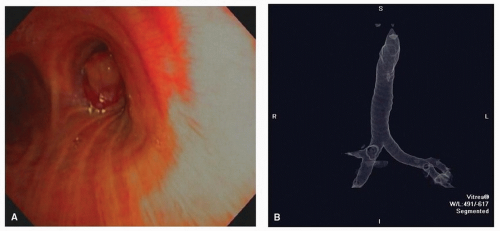
Three-dimensional reconstructions from CT can be useful in visualizing and planning surgery (Fig. 17.2A and B).
Barium esophagram may demonstrate esophageal involvement by extrinsic compression and/or invasion. Magnetic resonance imaging offers the advantage of soft tissue delineation of the trachea; however, it offers little advantage over CT.
Figure 17.1. CT imaging of tracheal SCC including endoscopic view (A) and coronal CT (B).
Figure 17.2. Endoscopic (A) and virtual endoscopic (B) views of tracheal tumor.
Functional studies are of limited usefulness. They may, at times, call attention to an obstructing lesion when clinical signs and symptoms are subtle. Functional studies may also give information about the status of the lung parenchyma.
All patients suspected of having or known to have a tumor of the trachea require endoscopy at some point during their evaluation. Great caution must be taken with the use of flexible laryngoscopy and bronchoscopy in these patients. Instrumentation of a nearly obstructed trachea may lead to bleeding, edema, or increased secretions that may precipitate sudden airway compromise. No effort should be made to employ instrumentation or to pass beyond a tumor if there is a high degree of obstruction unless preparations have been made to proceed directly with surgical intervention. It is preferable to simply identify the presence of the tumor and to defer any further evaluation and biopsy until appropriate arrangements have been made to manage the airway in the event of problems.
In general, the rigid bronchoscope is preferred when tumors of the trachea are studied. The need to establish an airway by tumor debulking or to obtain more adequate biopsy for diagnosis by frozen section justifies the use of the rigid bronchoscope (with appropriate magnifying telescopes). If necessary, the flexible bronchoscope may be passed through the rigid instrument for the evaluation of disease distal to the main obstruction. Careful measurements must be taken to determine the extent of tracheal involvement as well as to determine the amount of trachea remaining for reconstruction. It is important to establish the distance from the vocal cords to the superior aspect of the tumor, the length of the lesion, and distance from the inferior extent of the mucosal changes to the carina to facilitate surgical planning.
HISTOLOGY AND STAGING OF TUMORS OF THE TRACHEA
The common primary neoplasms of the trachea are listed in Table 17.1. The majority of tumors are either SCC or adenoid cystic carcinoma with SCC representing ˜50% of the histology in most series. Other less common tumors include adenocarcinoma, carcinoid, or neuroendocrine and other rare tumors including sarcoma.
Tumors are staged according to the AJCC staging system, which is illustrated in Table 17.2.10
Spread outside the trachea but not to adjacent organs or structures
T4
Spread to adjacent organs or structures
Tx
Unknown or cannot be assessed
N Stage
N0
No evidence of regional nodal involvement
N1
Positive nodal involvement
Nx
Unknown or cannot be assessed
Used with the permission of the American Joint Committee on Cancer (AJCC), Chicago, Illinois. The original source for this material is the AJCC Cancer Staging Manual, Seventh Edition (2010) published by Springer Science and Business Media LLC, www.springer.com.
Presentation
Primary SCC of the trachea may present as an exophytic mass that is circumscribed or as a spreading lesion that involves a considerable length of the trachea. It may also present as an ulcerative lesion. The cancer may grow into the mediastinum and may be noted radiographically as a bulky extratracheal mass. Metastases to paratracheal and subcarinal lymph nodes as well as direct invasion of mediastinal structures may also occur. This cancer occurs predominantly in males, and the majority of patients will have a smoking history.
Adenoid cystic carcinoma may present as an exophytic mass, frequently with poorly defined margins. A bulky extratracheal mass may be present. In the cervical trachea, the thyroid gland may be directly invaded as well as the esophagus. It is extremely unusual for adenoid cystic carcinoma of the trachea to present with regional lymph node metastases; if present, it suggests a high-grade subtype of this cancer. This tumor is histologically characterized by submucosal extension and perineural invasion over long distances of the trachea. The submucosal extent is often not visible, even after transection of the trachea. Frozen section control during surgery is critical, and the extent of the cancer may present the surgeon with a problem not predictable preoperatively. The hallmark of this cancer is frequent, and late presentation of metastases to the lungs is sometimes 5 to 10 years following presentation.
Only gold members can continue reading. Log In or Register to continue