Nociceptive processes and the perception of pain are influenced by biologic factors such as primary tumor type, stage of disease, and tumor site, as well as psychological factors such as anxiety and depression.1, 2, 3 With the onset of metastatic disease, approximately one in three patients report significant pain. Although pain tends to reflect the presence of metastases, this is not uniformly the case.4, 5
Tumor-induced pain may occur early in a disease or at an advanced stage. It is rarely one of the early indicators of the onset of disease, and, as such, is not a significant problem for the majority of patients at that stage. Only 5% to 10% of patients with solid tumors at diagnosis report pain at a level that interferes with mood and activity. However, new onset pain may be the concern that prompts the patient to seek medical consultation. Vuorinen et al.6 found that 28% of newly diagnosed unselected cancer patients reported pain. Pain is much more common as disease progresses. Cleeland et al.7 reported that the majority of patients with end-stage disease have pain of a severity that interferes with several aspects of the patient’s quality of life (QoL). Daut and Cleeland8 found that pain was an early symptom of cancer in 40% to 50% of patients with cancer of the breast, ovary, prostate, colon, or rectum, and in about 20% of patients with cancer of the uterus or cervix.
Knowledge of the natural history of a malignant disease facilitates understanding of the pain processes and is important in determining the nature and timing of all aspects of treatment. In addition, treatments can be painful and clinicians should differentiate treatment-associated pain from tumor pain. This chapter describes the more common neoplastic processes that cause pain and how they affect different systems within the body. We describe the basic pathophysiology of different tumor types, as well as the common treatments that may influence pain management and QoL issues.
BREAST CANCER
Breast cancer is a major health problem. It is by far the most frequent cancer of women (23% of all cancers), with 1.15 million new cases in 2002, ranking second overall when both sexes are considered together.9 More than half of the cases are in industrialized countries—about 361,000 in Europe (27.3% of cancers in women) and 230,000 in North America (31.3%). Incidence rates are high in most of the developed areas (except for Japan, where it is third after colorectal and stomach cancers), with the highest age-standardized incidence in North America (99.4 per 100,000).10 The prognosis from breast cancer is generally good, the average estimated survival rate in developed countries is 73% and in developing countries 57%.9 As a result, breast cancer ranks as the fifth cause of death from cancer overall, although still the leading cause of cancer mortality in women (14% of female cancer deaths). Because of its high incidence and relatively good prognosis, breast cancer is the most prevalent cancer in the world today; there are an estimated 4.4 million women alive who have had breast cancer diagnosed within the last 5 years.9 It is estimated that 1.5% of the US female population are survivors of breast cancer.11
The major influences on breast cancer risk appear to be certain reproductive factors, body size or obesity, alcohol, physical activity, exogenous hormones (oral contraceptives, hormone replacement therapy), and, possibly, diet. However, the etiology of this disease is not well known, and the most important risk factor, exposure to endogenous and exogenous estrogen throughout life, cannot explain the heterogeneity of prognoses nor the clinical features of patients. Women with germline mutations in the genes BRCA1 and BRCA2 have a lifetime risk of developing breast cancer of up to 80% and may account for up to 10% of breast cancer cases in developed countries.12 Women who received thoracic radiation therapy for Hodgkin disease after menarche and before 30 years of age also have a substantial increased risk of breast cancer.13
The origin of breast cancers is thought to be the epithelial cells that line the terminal duct lobular unit. Cancer cells that do not penetrate the basement membrane of the elements of the terminal duct lobular unit and the draining ducts are classified as in situ or and are thought to be noninvasive. Invasive breast cancers manifest dissemination of cancer cells outside the basement membrane of the ducts and lobules into the surrounding normal tissues. The histologic types of breast cancer include: carcinoma, ductal, lobular, nipple, and other (undifferentiated). The adverse prognostic factors for patients who have earlystage breast cancer include increasing tumor size and nodal involvement. The breast lymphatics drain via three major routes: axillary, transpectoral, and internal mammary. Intramammary lymph nodes are considered with, and coded as, axillary lymph nodes for staging purposes. Metastases to any other lymph node are considered distant. The diagnosis of breast cancer by triple assessment (clinical, radiologic, and pathologic, increasingly with core biopsy) is established in the context of multidisciplinary management. Positron-emission tomography (PET) scanning is useful in the evaluation of primary lesions, as well as regionally metastatic and systemic metastases of breast cancer. Fluorodeoxyglucose (FDG)-PET in conjunction with magnetic resonance imaging (MRI) offers useful treatment-planning data for patients clinically suspected of having recurrent axillary or supraclavicular breast cancer. FDG-PET can confirm the diagnosis of metastases in patients with indeterminate MRI findings. It also has been reported to reveal unsuspected metastases outside the axilla.14 FDG-PET is better than bone scintigraphy for the detection of osteolytic breast cancer metastases.15 Contrast-enhanced MRI is useful for the detection of the cancer that is occult on mammography or sonography, multifocal or multicentric disease in patients with a known primary, residual disease in patients with positive margins after breast-conserving surgery, response to neoadjuvant chemotherapy, unknown primary in patients with axillary lymph node metastases, early disease in high-risk BRCA1/2 patients, and recurrence in patients after completion of radiation therapy.16 Despite its improved accuracy, contrast-enhanced MRI is not recommended for general screening because of its expense and limited availability. MRI screening may be used for women with a 20% or greater lifetime risk of developing breast cancer.17
Therapeutic strategies for patients with breast cancer depend upon various prognostic variables that include size of the primary neoplasm, the presence and extent of axillary lymph node metastases, pathological stage of disease after primary therapy, and the presence or absence of receptor (estrogen, progesterone) activity. Breastconserving surgery by wide local excision is currently the preferred option, with mastectomy predominantly reserved for tumors not suitable for wide local excision and for patients who request it. Removal of axillary nodes provides prognostic information, guides adjuvant therapy, and may achieve local control. Biopsy of the sentinel lymph node is accepted as the standard of care in early breast cancer, with removal of the first lymph node or nodes that drain the tumor. Radiation therapy is the mainstay of local and regional treatment for breast cancer in women treated both by breast-conserving surgery and by mastectomy. After primary treatment with breast-conserving surgery and radiation, 10% to 20% of patients will have local recurrence in the breast within 1 to 9 years. Between 10% and 25% of these will have locally extensive or metastatic disease. After radical surgery and postoperative radiation, loco-regional recurrences occur in <10%.18
Endocrine manipulation with tamoxifen, ovarian ablation, or both are the preferred options with endocrine-responsive tumors. Hormone receptor status is a well-established prognostic and predictive factor. A meta-analysis of seven cooperative group adjuvant therapy trials confirmed the role of estrogen receptor (ER) status as a prognostic factor.19 Women who had ER-negative tumors showed a peak annual hazard of recurrence 1 to 2 years after surgery of 18.5%. The hazard declined rapidly thereafter to a rate of 1.4% in years 8 through 12. Approximately two thirds of women with breast cancer have ER-positive disease. The selective estrogen modulator, tamoxifen, is the standard first-line therapy for women with ER positive breast cancer. For postmenopausal women, third-generation nonsteroidal aromatase inhibitors are useful alternatives. Aromatase inhibitors and tamoxifen have different spectra of side effects. Tamoxifen causes more vasomotor symptoms, thromboembolism, and strokes, whereas aromatase inhibitors are associated with more arthralgias, bone thinning, and fracture. For some patients the arthralgia associated with an aromatase inhibitor, which is probably caused by estrogen suppression, may lead to discontinuation of therapy. Patients taking aromatase inhibitors should have bone mineral density measured at baseline.
Overexpression of transmembrane peptide growth factor receptors, such as epidermal growth factor receptor (EGFR) or the human epidural receptor 2 (HER2) has been associated with poor prognosis and resistance to hormonal therapy.20 HER2 is amplified and overexpressed in 15% to 30% of newly diagnosed breast cancers and is associated with more aggressive behavior.21 HER2-positive breast cancers manifest resistance to tamoxifen therapy, presumably as a result of cross-talk between intracellular signaling pathways.22 The antibody trastuzumab (Herceptin), which targets HER2 and is generally given for 12 months, reduces the risk of relapse by a further 35% to 52%.23 Biopsies of tumors from breast cancer patients who have relapsed on an antiestrogen show a functional estrogen receptor,24 although women who have become refractory to tamoxifen can respond to further endocrine manipulation with an aromatase inhibitor or fulvestrant (Faslodex).25 Because the ER remains functional and can interact with growth factor signaling pathways, there is a strong rationale for combining novel signal transduction inhibitors with endocrine therapy rather than using them independently. Combining hormonal therapy with angiogenesis inhibitors may be an alternative strategy. Angiogenesis is critical to tumor growth and is principally mediated via tumor secretion of vascular endothelial growth factor (VEGF). The successful use of a monoclonal antibody against VEGF (bevacizumab, Avastin) in combination with chemotherapy has been demonstrated in the treatment of breast cancer.26 A large number of endocrine/targeted combinations are currently in clinical trials and may offer improvement in outcomes for women with ER-positive breast cancer.
Deaths from breast cancer have decreased in the recent years, in part because of improved screening techniques, surgical interventions, understanding of the pathogenesis of the disease, and utilization of traditional chemotherapies in a more efficacious manner. Combination chemotherapy is superior to single agents, and anthracycline-containing regimens are superior to the combination of cyclophosphamide, methotrexate, and fluorouracil (5-FU).27 Compared with single-chemotherapy agents for metastatic breast cancer, combination regimens show a statistically significant advantage for tumor response and time to progression in women with metastatic breast cancer, a modest improvement in overall survival, and significantly worse toxicities.28 Anthracycline (doxorubicin or epirubicin)-based chemotherapy reduces mortality by 38% for women younger than 50 years and 20% for women aged 50 to 69 years.29 Taxanes are now fundamental in the treatment of early and advanced breast cancer. The addition of a taxane (docetaxel or paclitaxel) to anthracyclinebased chemotherapy reduces the relative risk of death further, by about 15%.30 However, tumors vary in their sensitivity to these agents; resistance can be acquired or de novo resistance can occur. Epothilones and associated analogs are novel microtubule-stabilizing agents that induce apoptosis and promote cell death. Research now supports the efficacy of epothilones in breast cancer patients who have progressed on taxanes and anthracyclines.31 Combined endocrine therapy-chemotherapy is the standard adjuvant treatment in high-risk patients with endocrine-responsive tumors.
Widespread metastasis is characteristic of breast cancer and can involve any organ in the body, most commonly bone, lung, liver, and brain. Metastases characteristically appear within a few years of the onset of the primary lesion, but late recurrence (sometimes many years later in bone) is well described. Although metastatic disease may be asymptomatic, the most common site of metastases— bone—typically hurts. Between 40% and 60% of patients with breast cancer will have metastasis to bone, and, in many of these patients, the involved bones (vertebrae, femoral and humoral shafts, the acetabular area) are those that are involved with motion. Moreover, patients with metastatic breast cancer to bone as their only site of metastatic disease have median survival expectations of 27 to 29 months, during which time pain may be the chief manifestation of disease. Even patients with pulmonary metastases have median survivals of the order of 18 to 23 months,32 and patients with only unilateral pleural involvement on the order of 44 months.33 Metastatic breast cancer may be currently incurable, but it certainly is treatable. Survival of patients with metastatic disease has been improving over the decades as treatments have improved. For many women, treatment now resembles that for a chronic disease, with sequential use of different chemotherapy and hormonal therapies to control disease and maintain quality of life. Metastatic breast cancer in many women has become a chronic relapsing and remitting disease that may transiently respond to an array of cytotoxic and endocrine therapies.
TABLE 7.1 CAUSES OF PAIN IN PATIENTS WITH BREAST CANCER
Long interactions are likely between clinicians and patients with metastatic breast cancer. This disease in patients with metastatic breast cancer usually follows one of two patterns: an indolent course or disease not immediately life-threatening, and that which is rapidly progressing or with extensive vital organ disease. Treatment planning, both of the disease itself and of the associated pain, mandates understanding of the natural history and its variances in breast cancer.
Table 7.1 lists some of the common causes of pain in patients with breast cancer.
LUNG CANCER
Worldwide, the most common cancer is lung cancer, and it is the leading cause of cancer-related mortality in Western countries. Lung cancer has been the most common cancer in the world since 1985, and, by 2002, there were 1.35 million new cases, representing 12.4% of all new cancers.9 It was also the most common cause of death from cancer, with 1.18 million deaths, or 17.6% of the world total. Almost half (49.9%) of the cases occur in the developing countries of the world. Lung cancer remains a highly lethal disease. Survival at 5 years measured by the Surveillance, Epidemiology, and End Results Program (SEER) program in the United States is 15%, the best recorded at the population level. The average survival in Europe is 10%, not much better than the 8.9% observed in developing countries.
A practical classification used by clinicians separates lung cancer into two distinct subgroups: small-cell lung cancer (SCLC) and nonsmall cell lung cancer (NSCLC) (Fig.7.1). NSCLC is responsible for 80% to 85% of all lung cancers, and SCLC the remaining 15% to 20%. SCLC is associated very strongly with smoking. It tends to arise centrally, presenting in the main-stem or lobular bronchi. SCLC probably arises from the basal neuroendocrine Kulchitsky cells. The tumor tends to metastasize early to hilar, mediastinal, and distant sites. The disease is often associated with paraneoplastic syndromes, including the syndrome of inappropriate secretion of antidiuretic hormone (SIADH), ectopic adrenocorticotropic hormone (ACTH) production with Cushing syndrome, and Eaton-Lambert syndrome, a rare neuromuscular disorder characterized by progressive muscular weakness, autonomic dysfunction, and absent deep tendon reflexes. There are three subcategories of SCLC: oat-cell, small-cell, and combined oat-cell carcinoma. NSCLC is a heterogeneous aggregate of histologies. The most common histologies are epidermoid or squamous carcinoma, adenocarcinoma, and large-cell carcinoma. These histologies are often classified together because approaches to diagnosis, staging, prognosis, and treatment are similar. Adenocarcinoma is the predominant histologic subtype in many countries.
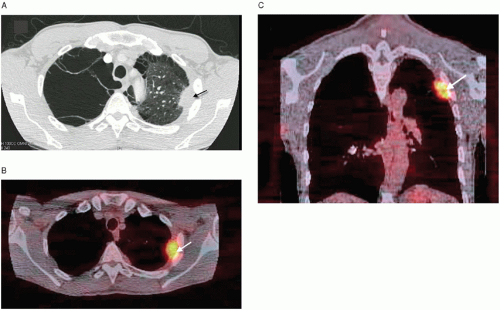
FIGURE 7.1 A: A 53-year-old man with stage IV nonsmall cell lung cancer. Axial CT chest shows a mass in the left upper lobe (arrow). Extensive right upper lobe emphysematous changes are also present. Hypermetabolic uptake within the area of the mass are seen on axial PET CT (B) and on coronal PET CT (C). PET, Positron-emission tomography; CT, computed tomography.
Lung cancers that occur in the apex of the chest and invade apical chest wall structures are called superior sulcus tumors or Pancoast tumors (Fig. 7.2). The classic description of such cases involves a syndrome of pain radiating down the upper extremity as a manifestation of brachial plexus involvement. With improvements in imaging, earlier diagnosis, and a more detailed understanding of the anatomy, a tumor can be classified as a Pancoast tumor when it invades any of the structures at the apex of the chest, including the most superior ribs or periosteum, the lower nerve roots of the brachial plexus, the sympathetic chain near the apex of the chest, or the subclavian vessels. These tumors are now divided into anterior, middle, and posterior compartment tumors, depending on the location of the chest wall involvement in relation to the insertions of the anterior and middle scalene muscles on the first rib. A syndrome of pain radiating down the arm is no longer a prerequisite for an apical tumor to be designated a Pancoast tumor.34 The presence of Horner syndrome is associated with poor survival.35
Staging procedures include history, physical examination, routine laboratory evaluations, chest x-ray, and chest computed tomography (CT) (contrast enhanced). The CT scan should extend inferiorly to include the liver and adrenal glands. MRI scans of the thorax and upper abdomen do not appear to yield advantages over CT scans.36 The combination of CT scanning and PET scanning has greater sensitivity and specificity than CT scanning alone.37 Patients at risk for brain metastases may be staged with CT or MRI scans.
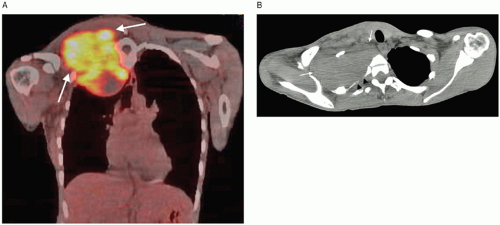
FIGURE 7.2 A 38-year-old woman with severe pain in right upper chest, back, and upper extremity. Patient was diagnosed with Pancoast tumor from a lung adenocarcinoma. Coronal PET CT (A) shows marked FDG uptake (arrows) in right upper chest and supraclavicular region. CT (B) shows the large supraclavicular mass (arrows) with destruction of the first rib (arrow heads). PET, Positron-emission tomography; CT, computed tomography; FDG, fluorodeoxyglucose.
Complete evaluation of a patient with newly diagnosed SCLC is similar. Although the prevalence of brain metastases at diagnosis varies, the brain is a common site of treatment failure; therefore, evaluation of the brain before treatment is usually required. Untreated SCLC is aggressive, with a median survival of 2 to 4 months after diagnosis.38 SCLCs are relatively sensitive to cytotoxic chemotherapy and radiation therapy. Chemotherapy is used for most patients, either as adjuvant therapy for the few patients eligible for surgery, or as primary therapy for patients with inoperable tumors. Surgery is usually limited to patients with smaller tumors without evidence of nodal involvement or spread outside the hemithorax of origin. The benefit of surgery in conjunction with chemotherapy in terms of survival for patients with limited stage disease is uncertain. The role of radiation therapy in extensive disease is less established than in patients with limited-stage disease.39 Patients with limited-stage SCLC should be treated with combined concurrent chemoradiotherapy. Patients eligible to receive early concurrent chemoradiotherapy should be treated with accelerated hyperfractionated radiation therapy concurrently with platinum-based chemotherapy.40 Because brain metastases are so common with this disease, patients with either limited-stage or extensive-stage SCLC with a clinical response should be offered prophylactic cranial radiation.40 Many patients respond to primary therapy but relapse after remissions of varying duration. The prognosis of patients who relapse is poor. Chemotherapy regimens usually involve platinumetoposide combinations in patients with limited stage disease and platinum-based regimens in patients with extensive-stage disease.
For early-stage and locally advanced NSCLC (stages I through III), a multimodality treatment approach is appropriate, because it improves survival. Treatment options include surgery (lobectomy, pneumonectomy, or segmental, wedge, or sleeve resection as appropriate), radiation therapy with curative intent (for potentially operable tumors in patients with medical contraindications to surgery), and adjuvant chemotherapy with or without other modalities after curative. In general, patients with an early-stage NSCLC without mediastinal nodal involvement (stage I and II) are treated primarily with surgery, whereas those with a locally advanced lung cancer with mediastinal nodal involvement (stages IIIA and IIIB) are treated with chemotherapy and radiation. Approximately 40% of patients with newly diagnosed NSCLC have stage IV disease.41 Chemotherapy improves survival and palliates disease-related symptoms in patients with good performance status. Palliative chemotherapy typically involves a cisplatin-based or carboplatin-based regimen. Bevacizumab (Avastin) improves survival combined with carboplatin and paclitaxel (Taxol) in a clinically selected subset of patients with stage IV NSCLC and good performance status (nonsquamous histology, lack of brain metastases, and no hemoptysis).41 Clinical trials show efficacy for agents such as docetaxel (Taxotere) and pemetrexed (Alimta) in the second line setting for refractory disease.42 Preliminary data also shows some efficacy for erlotinib (Tarceva) in patients with advanced NSCLC.43 Recurrent NSCLC may be treated with chemotherapy or radiation therapy.
Radiation therapy may be effective in palliating symptomatic local involvement with NSCLC, such as tracheal, esophageal, or bronchial compression; bone or brain metastases; pain; vocal cord paralysis; hemoptysis; or superior vena cava syndrome. In some cases, endobronchial laser therapy and/or brachytherapy has been used to alleviate proximal obstructing lesions.44 Thoracic radiation therapy is an effective treatment modality to relieve symptoms from intrathoracic disease, either after disease progression during chemotherapy or in patients who are not candidates for or decline chemotherapy.
Paraneoplastic syndromes frequently are associated with lung cancers, in particular SCLS. Paraneoplastic syndrome implies the ability of certain tumors to produce signs and symptoms at a distance from the site of the primary tumor or its metastases. These syndromes are typically caused by ectopic hormone production or immune-mediated tissue destruction caused by neural antigen expression from cancer cells. Cancer cachexia and SIADH occur in approximately 40% of cases. Cushing syndrome can result from increased serum and tissue levels of immunoreactive ACTH. Often seen in patients with NSCLC, hypercalcemia is uncommon in patients with SCLC. About 10% of all lung cancer patients have hypercalcemia, and this is not associated with bone metastases in 10% to 15%. Humoral hypercalcemia of malignancy is more common in NSCLC, and especially squamous cell carcinoma. Malignancy-associated hyponatremia is commonly associated with production of arginine vasopressin (AVP) by tumor cells. A significant proportion of the new cases of syndrome of SIADH in elderly smokers are due to SCLC. The neurological syndromes associated with lung cancer can be rare disorders such as subacute cerebellar degeneration, optic neuritis and retinopathy, subacute necrotizing myelopathy, and peripheral neuropathy. Paraneoplastic neurologic syndromes also include Lambert-Eaton myasthenic syndrome.
Pain is a major symptom in the patient with lung cancer.45, 46 The duration of pain before diagnosis can vary. Huhti et al.47 reported that 20% of patients had pain for more than 6 months before the diagnosis. Portenoy et al.48 found that the median duration of pain experienced by lung cancer outpatients was 4 weeks, but there was a wide range, from 1 week to 177 weeks. Ischia et al.49 found that 30% of patients with locally advanced disease had pain for more than 6 months before the diagnosis was established. Lung cancer can cause pain either locally by invasion of the parietal pleura, ribs and chest soft tissue, thoracic spinal column and cord, or brachial plexus, or remotely by its propensity to metastasize. Nociceptive or somatic pain is the major pathophysiologic subtype in lung cancer pain (weighted mean prevalence 73%; range: 75% to 86%), but in approximately one third of cases, the pain is a visceral or neuropathic subtype (weighted mean prevalence 32% and 30%, respectively).45,50, 51, 52 Watson and Evans51 reported that the three main causes of pain in 221 lung cancer patients were skeletal metastatic disease (34%), Pancoast tumor (31%), and chest wall disease (21%) and together comprised 78% of tumor-related problems in these patients. The chest area is the most common site of pain in patients with small-cell lung cancer. Patients often complain of pain that is poorly localized, dull in character, which may radiate to the neck or back, and is exacerbated by coughing. Mercadante et al.45 reported that patients with advanced lung cancer commonly reported chest wall (including ribs and shoulder blade) pain, followed by lower extremities and lumbar regions, then abdomen and upper extremities, and the head area.
PROSTATE CANCER
Prostate cancer is an age-associated disease. Over 70% of all cases of prostate cancer are diagnosed in men over 65 years of age, and the median age of men with prostate cancer is 79 years.53, 54 The risk of developing prostate cancer increases from 1 in 45 for those aged 40 to 59 years to 1 in 7 for those aged 60 years or older.55 This is the fifth most common cancer in the world and the second most common in men (11.7% of new cancer cases overall, 19% in developed countries, and 5.3% in developing countries).9 The prognosis is relatively good; it is a less prominent cause of mortality, with 221,000 deaths per year (5.8% of cancer deaths in men and 3.3% of all cancer deaths).
Prostate cancers (95%) are almost all adenocarcinomas. The remaining 5% are squamous cell carcinoma, signet-ring carcinoma, transitional carcinoma, neuroendocrine carcinoma, or sarcoma. Prostate adenocarcinoma typically invades regional structures, including the seminal vesicles, urinary bladder, or surrounding tissues. Distant metastases can arise from lymphatic spread or hematogenous dissemination, which is usually to bone. Tumor aggressiveness can be determined by an examination of the microscopic pattern of the cancer cells. The most commonly used tumor grading system is the Gleason grading, which assigns a grade for each prostate cancer from 1 (least aggressive) to 5 (most aggressive) based on the degree of architectural differentiation of the tumor. Tumors often show multiple different grade “patterns” within the prostate or even a single core biopsy. To account for this, the Gleason score is obtained by assigning a primary grade to the most predominant grade present and a secondary grade to the second most predominant grade. An exception to this is in the case where the highest (most aggressive) pattern present in a biopsy is not either the most predominant or second most predominant pattern; in this situation, the Gleason score is obtained by combining the most predominant pattern grade with the highest grade. The Gleason score is then displayed as, for example, 3 + 4, where 3 would be the most common pattern of tumor and 4 the second most common pattern (or highest pattern) of tumor seen in the core. Given that the individual Gleason value can range from 1 to 5, the added values (Gleason scores or “sums”) can range from 1 + 1 to 5 + 5 or from 2 to 10. Generally, Gleason scores of 2 to 4 are uncommon; the majority of biopsied tumors range from 5 to 10. The regional lymph nodes for the prostate are the pelvic nodes below the bifurcation of the common iliac arteries. Distant lymph nodes are outside the confines of the true pelvis. They are the aortic (para-aortic, periaortic, lumbar), common iliac, inguinal, superficial inguinal (femoral), supraclavicular, cervical, scalene, and retroperitoneal nodes.
Serum prostate-specific antigen (PSA), digital rectal examination (DRE), and transrectal ultrasonography (TRUS) are the three major diagnostic tools for prostate cancer. PSA is an organ-specific glycoprotein which originates in the cytoplasm of ductal cells of the prostate. Its function is the liquefaction of seminal fluid. PSA is prostate tissuespecific, but not tumor-specific. This limits its utility, because elevated PSA levels may also be the sign of benign disorders such as benign prostatic hyperplasia (BPH), or prostatitis. Moreover, there is no consensus as to what PSA level constitutes disease recurrence following prostatectomy. Nonetheless, rising PSA levels are a cause of concern in a patient who has had prostate cancer. Men presenting initially with PSA <1.0 ng/mL may not have to be rescreened for a period of 8 years. With a PSA in the range of 1.0 to 2.9 ng/mL, prostate biopsies may detect many cancers, with a proportion of 20% to 30% showing aggressive patterns by Gleason score.56
Prostate gland neoplasms can lead to local rectal, urethral, suprapubic, and penile pain due to expansion and inflammation of the prostate. Pain referred to the back, lower extremities, and abdominal area can result from tumor growth within the pelvis. Distant bone pain with associated neurological dysfunction can be found with long bone, vertebral, and skull metastases (Table 7.2).
TABLE 7.2 CAUSES OF PAIN IN PROSTATE CANCER
Causes of Pain
Examples/Clinical Syndromes
Bone metastasis
Single metastasis to pelvis or long bone
Vertebral body metastasis, spinal cord compression
Base-of-skull metastasis, cranial nerve palsies
Perineal pain syndromes
Soft tissue metastasis
Lumbosacral plexopathy
Pelvic tension “myalgia”
Pelvic visceral pain
“Prostatitis” pain
(From Payne R. Pain management in the patient with prostate cancer. Cancer. 1993;71 (3 Suppl):1131-1137. Copyright 1993 American Cancer Society. This material is reproduced with permission of Wiley-Liss, Inc., a subsidiary of John Wiley & Sons, Inc. )
Prostate cancer has a predilection for bone: the majority of patients with metastatic disease will have bone pain (Fig. 7.3). Vital organs are rarely the sites of metastasis, and disease progression is usually slow. Rapid evolution can be seen with spinal cord compression due to vertebral metastasis and collapse, or epidural metastasis, or with ureteral obstruction secondary to retroperitoneal lymph node metastases.
The majority of symptomatic patients with prostate cancer present either bone pain, other bone-related symptoms, or symptoms related to urethral obstruction. Clinical syndromes can be identified by the site of bony involvement, the development of mechanical instability secondary to fractures, and by the neurologic dysfunction caused by tumor infiltration of contiguous neurologic structures. Metastases to bones of the hip and pelvis often produce local pain that is exacerbated by movement, especially during weight bearing. The syndrome of perineal pain consists of perineal and perirectal pain that is accentuated by pressure on the perineal region, such as that caused by sitting or lying prone. Such a patient may not be able to sit or lie flat because of the pain. Invasion of the parasympathetic sacral innervation to bladder and bowel may lead to early incontinence. Local spread of tumor from the prostate into other pelvic and abdominal structures often produces visceral and neuropathic pain, particularly if the lumbosacral plexus is involved. Stage IV prostate cancer includes patients with locally advanced tumors (T4, indicating invasion of the bladder, rectum, pelvic wall), involvement of lymph nodes (N1) or presence of distant metastasis (M1), which includes nonregional lymph-nodes or metastasis to other organs, usually bones. Imaging studies of some patients may not reveal metastatic disease, although patients may present with a high PSA. A PSA level above 20 ng/mL is highly suggestive of advanced disease, and a level >50 ng/mL is virtually diagnostic of metastatic disease.
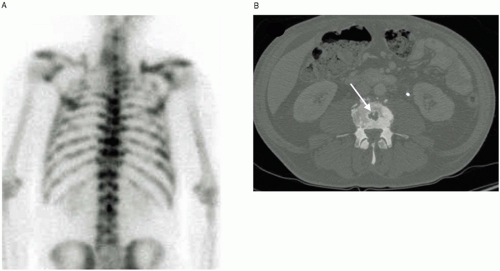
FIGURE 7.3 A 61-year-old man with castration-resistant prostate adenocarcinoma with extensive skeletal metastases. Patient complained of diffuse achy back pain. Bone scan (A) shows diffuse tracer uptake throughout the spine. Axial CT of lumbar spine (B) shows an osteoblastic lesion in the vertebral body (arrow). CT, Computed tomography.
Patients with clinically localized prostate cancer may be considered candidates for interstitial prostate brachytherapy, but practitioners differ with respect to which risk groups are offered this approach. Some practitioners will use this treatment option for low-risk disease only, whereas others will treat both low- and intermediaterisk patients. Before initiating therapy, a transrectal ultrasound-based volume study is performed to assess prostate volume and to determine the number of needles and corresponding radioactive seeds, the isotope, and the isotope strength necessary for the procedure. Radioactive needles are implanted via a transperineal approach under guidance of transrectal ultrasound or magnetic resonance imaging. Common regimens employ 120 Gy (palladium) or 140 Gy (125I), with postoperative dosimetry performed for each patient. Radical prostatectomy involves removal of the entire prostate and the attached seminal vesicles with the ampulla of the vas deferens. The procedure may be performed using a retropubic or perineal incision or by using a laparoscopic or robotic-assisted technique. Depending on tumor characteristics and the patient’s sexual function, either nerve-sparing or nonnerve-sparing surgery is performed. Pelvic lymphadenectomy may be performed concurrently particularly for patients at higher risk for nodal involvement.
Five-year relative survival rates are a function of the stage at diagnosis: from 80% or more when malignancy is confined to the prostate to about 25% where bone metastases have already occurred. Adenocarcinoma of the prostate is dependent on hormonal stimulation (by testosterone) until a very late stage of the disease, at which point new clones of hormone-independent cells arise.57 Treatment starts with hormone manipulation while the disease is hormone sensitive. Androgen deprivation therapy is the mainstay of initial therapy for systemic disease, whether it is biochemical recurrence (ie, PSA-rise only) after definitive localized therapy or overt metastatic disease. Though hormone manipulation can control the disease for several years, eventually addition of cytotoxic medication is required due to development of hormone-independent tumor cells. For patients with localized or local advanced prostate cancer, neoadjuvant and adjuvant hormone therapy combined with prostatectomy or radiation therapy is associated with significant clinical benefits.58 First-line hormone therapy consists of blocking testosterone synthesis, either by orchiectomy or by using a gonadotrophin-releasing hormone analog (aLHRH) such as leuprolide (Lupron). The most common side effects of leuprolide are hot flushes, decreased libido, sexual impotence, and osteopenia. Because therapy is associated with low testosterone levels, additional problems may occur. Low testosterone levels have been shown to affect mood and self-esteem. Androgen deprivation therapy may be associated with an increased risk of depression. In a pilot cross-sectional study of 45 men, 13% of men receiving androgen deprivation therapy had major depressive disorder, eight times the normal rate of depression {Pirl, 2002 #2318}. Men with a previous history of depression were more likely to develop a major depressive disorder. Furthermore, cognitive issues, particularly in older men, may occur with therapy.59
Patients who want to try to maintain sexual function (seldom possible with use of an aLHRH) could try to use nonsteroidal androgen receptor blockers such as Cyproterone first, although the effectiveness of treatment may not be as good.60 Hormone manipulation is effective, but not curative in 80% to 85% of cases. Chemotherapy has a well-recognized role in the management of hormonerefractory prostate cancer but results are not impressive. Chemotherapeutic agents in use include estramustine, 5-FU, cyclophosphamide, doxorubicin, mitoxantrone, and docetaxel. In a review of chemotherapy for hormonerefractory prostate cancer, Mike et al.61 noted that only studies using docetaxel reported a significant improvement in overall survival compared to best standard of care, although the increase was small (<2.5 months). The mean percentage of patients achieving at least a 50% reduction in PSA compared to baseline was as follows: estramustine 48%, 5-FU 20%, doxorubicin 50% (one study only), mitoxantrone 33%, and docetaxel 52%. Pain relief was reported in 35% to 76% of patients receiving either single agents or combination regimens. A regime of docetaxel given every three weeks significantly improved pain relief compared to mitoxantrone plus prednisone. All chemotherapeutic agents, either as single agents or in combination, were associated with toxicities, the major ones being myelosuppression, gastrointestinal toxicity, cardiac toxicity, neuropathy, and alopecia. QoL was significantly improved with docetaxel compared to mitoxantrone plus prednisone.
External beam radiation therapy for the treatment of locoregional prostate cancer yields similar survival rates to radical prostatectomy (10-year survival: 90% to 95%, 60% to 70%, and 50% to 60% in T1, T2, and T3-stages, respectively).62 Postoperative radiation therapy in highrisk prostate cancer may improve the local and distant disease-free survival of patients. The relative role of radiation therapy in metastatic disease is to deal with isolated symptoms, which may persist despite systemic treatment. Palliative radiation provides pain relief in up to 80% of prostate cancer patients with single or at most a few sites of localized bone pain.63 A single large hemibody radiation field (typically 8 Gy) is as effective in the alleviation of pain for patients with widespread bone metastasis64, 65 compared to the more standard treatment of fractionated therapy of 30 Gy delivered in 10 treatment fractions over 2 weeks,66 although patients receiving a single treatment fraction have a higher rate of retreatment and less acute toxicity. Bisphosphonates should be considered for patients with metastatic prostate cancer for the treatment of refractory bone pain and prevention of skeletal events.67 In addition, androgen deprivation can be considered a risk factor for the development of osteopenia, osteoporosis, and bone fracture, which can be mitigated by appropriate bisphosphonate therapy.68
COLORECTAL CANCER
Colorectal cancer is a common malignancy in the Western world and is responsible for about 10% of all cancer deaths in both Europe and the United States.69 Approximately 30% of all patients with colorectal cancer have metastatic disease at diagnosis, and 50% of early-stage patients will eventually develop metastatic or advanced disease70 (Fig. 7.4). In terms of incidence, colorectal cancers rank fourth in frequency in men and third in women. Survival estimates (in men) at 5 years are 65% in North America, 54% in Western Europe, 34% in Eastern Europe, and 30% in India. The overall relatively good prognosis means that mortality is about one half that of incidence, whereas prevalence is second only to that of breast cancer worldwide, with an estimated 2.8 million persons alive with colorectal cancer within 5 years of diagnosis.9
There are strong correlations between risk of colon cancers and consumption patterns of meat,71 fat (specifically animal fat),72 and fiber.73 In addition, physical inactivity, excess body weight, and a central deposition of adiposity have a major influence on risk of colon cancer.74 Adenocarcinoma (>90%) is the most common histologic type, followed by carcinoid tumors, leiomyosarcomas, and lymphoma. Spread to regional lymph nodes is usually correlated with depth of invasion by the primary tumor and its grade of differentiation. Tumors apparently confined to the bowel wall may have nodal spread in 10% to 20%. Hematogenous spread via portal venous transmission is usually to the liver. Age is one of the strongest risk factors for colon cancer, particularly age over 50 years.75 Higher-risk groups include patients with a family history of colorectal cancer or adenomatous polyps, a past history of successful resection of colorectal cancer or adenomatous polyp, and a long-standing history of ulcerative colitis or Crohn disease. More than 95% of colorectal cancers arise in benign adenomatous polyps (adenomas) that develop in the large bowel over several years.76 Tumors are staged with the TNM universal system or a modification of the Dukes system for colorectal cancer. The Astler and Coller-modified Dukes staging system uses the following designations: A, a tumor limited to the mucosa; B1, tumors extending into the muscularis propria that do not breach the serosa; B2, tumors that penetrate the bowel wall without lymph node or distant metastases; and C, tumors with regional lymph node involvement without distant metastases. Many allocate cancer with distant metastases or local spread into other organs as stage D. The stage-related 5-year survival of cancers reported in different series is as follows: A, 85% to 95%; B, 60% to 80%; C, 30% to 60%; and D, less than 5%.
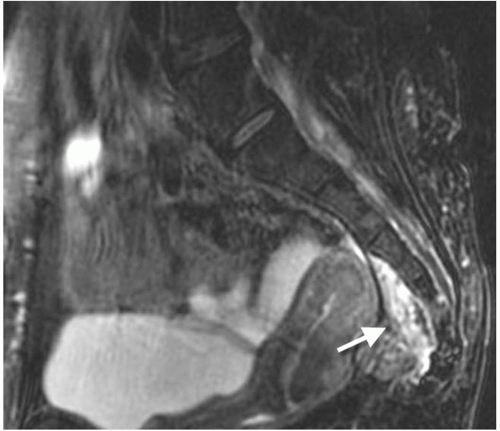
FIGURE 7.4 A 52-year-old woman with pelvic recurrence of rectal cancer (T3 N0 MO). Patient was initially treated with abdominoperineal resection and adjuvant chemoradiation. Three years later, patient presented with increasing pelvic pain and dyspareunia with an elevated CEA level. Axial MRI shows a 2-cm soft-tissue mass behind the uterus, extending from the coccyx to the level of mid-S3 (arrow). This mass was surgically resected with a posterior exenteration, sacrectomy, and rectus myocutaneous flap. CEA, carcinoembryonic antigen; MRI, magnetic resonance imaging.
Metastatic spread to the liver is most common (65%); extra-abdominal metastases in the lungs (25%) and brain and bone (10%) are less frequent. Approximately one in five patients has metastatic colorectal cancer at diagnosis, which, at best, is associated with a 5-year survival rate of just 10%.77 Recurrences usually appear within 2 years (about 70%) and almost all (90%) within 5 years.
Complete resection of all malignant tissue offers the only reasonable chance of cure or long-term survival and is the treatment of choice for most patients with colorectal cancer. The goal of surgery is a wide resection of the involved segment of bowel together with the removal of its lymphatic drainage. The surgical approach to rectal cancers is determined by the location and size of the tumor. Radical surgery for rectal cancer is associated with potential mortality as well as significant morbidity associated with poor bowel or sexual function, and possibly a stoma. An abdominoperineal resection is reserved for patients without such a margin or for some with large bulky tumors deep in the pelvis, extensive local spread of rectal cancer, or a poorly differentiated cancer. In patients who underwent a low anterior resection for rectal cancer, bowel continuity was classically restored with a straight colorectal anastomosis. In 1986, J-pouch coloanal anastomosis was developed in order to increase colonic reservoir function and improve QoL.
There is no well-defined role for radiation therapy in colon cancer. The response rates to chemotherapy (usually 5-FU) in recurrent and metastatic cancer remain poor and of limited duration. In addition to staging systems, independent prognostic factors include histologic type, histologic grade, serum carcinoembryonic antigen (CEA) level, and extramural venous invasion. Elevated CEA levels are found in a variety of cancers other than colonic, such as breast, lung, pancreas, stomach, and ovary. Postoperative serum CEA testing should be performed every 3 months in patients with stage II or III disease for at least 3 years after diagnosis.78 Because 5-FU therapy may falsely elevate CEA values,79 adjuvant treatment should probably be completed before initiation of surveillance. Patients who are at higher risk of recurrence and who are surgical candidates should undergo annual CT scanning of the chest and abdomen for 3 years after primary treatment. FDG-PET has utility in the initial staging of colorectal cancer and for evaluation of recurrent disease. Contrast-enhanced CT and FDG- PET imaging appear to increase the sensitivity, specificity, and accuracy for staging. Contrast-enhanced CT increases the spatial localization, and FDG-PET adds functional information.80
Ten years ago, 5-FU was the only treatment for metastatic colorectal cancer. With the development of new drug combinations, both the response rate and median overall survival have doubled, approaching 50% and 20 months, respectively.81 Neoadjuvant chemotherapy may be used with the goal of inducing tumor shrinkage so that the disease becomes resectable and thereby potentially curable. Chemotherapy plus newer biologic agents such as bevacizumab or cetuximab might additionally improve survival.82 Both oxaliplatin combined with bolus and continuous infusion 5-FU plus leucovorin (FOLFOX) and irinotecan combined with bolus and continuous infusion 5-FU plus leucovorin (FOLFIRI) are recognized as standard first-line therapies for metastatic colorectal cancer, with FOLFOX emerging as the preferred upfront treatment option in the United States.77 Colorectal cancer can lead to severe pain from bowel obstruction, rupture of a viscus or from metastatic disease, most often in the liver.
Preoperative or postoperative radiotherapy with concurrent chemotherapy is the standard of care for patients with Stage II and III rectal cancer. Patients with locoregional recurrence have a poor prognosis. The median overall survival in some series was just over 2 years from the time of recurrence, with an estimated 3-year survival rate of 41%.83 Yu et al.83 reported on the patterns of locoregional recurrence after surgery and radiation therapy or chemoradiation in 554 patients with rectal cancer. The estimated 5-year locoregional control rate was 91%. Thirty-six patients had locoregional recurrences at 43 sites. There were 28 (65%) in-field, 7 (16%) marginal, and 8 (19%) out-of-field recurrences. Of the in-field recurrences, nearly 80% occurred in the low pelvic and presacral regions. Fifteen (56%) occurred in the low pelvis, 6 (22%) in the presacral region. Presacral tumors may cause significant low back pain (Fig. 7.4). With disease progression and sacral infiltration, patients may experience severe lower extremity pain from nerve root involvement and bladder/bowel dysfunction. In patients with a history of colorectal cancer complaints of back pain in combination with neurological symptoms, pain persisting and gradually worsening over time and coccygeal pain that fails to resolve should prompt further investigations such as pelvic MRIs and/or PET CT scans.
HEAD AND NECK CANCER
Head and neck cancer (oral cavity, pharynx, and larynx) is the eighth most common cause of cancer-related deaths worldwide.84 In the United States, 47,560 new head and neck carcinomas were diagnosed in 2008, and this disease accounts for 5% of all newly diagnosed cases of cancer.85 These cancers comprise 5% of all cancer cases worldwide and result in 6% of cancer deaths in men and 3% in women.9 The majority of cases present with potentially curable but locally advanced disease. Despite advances in the treatment of these patients, long-term disease-free survival and overall survival remain poor. Approximately 40% to 60% of patients develop local recurrences, and 20% to 30% will be diagnosed with distant metastatic disease.86 Patients with head and neck cancers are at increased risk of developing a second primary cancer of the oral cavity and pharynx, esophagus, larynx and lung; these cancers are largely due to shared risk factors such as tobacco and alcohol.87 The 5-year survival for head and neck cancer patients is approximately 50% and only 20% if these patients develop a second primary cancer.87
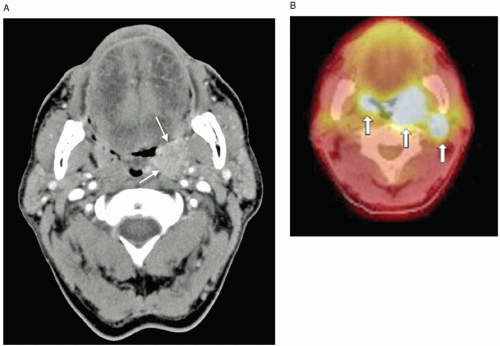
FIGURE 7.5 A 58-year-old man with bilateral squamous cell carcinoma of the tonsils treated with concurrent radiation therapy and cetuximab. Patient had a long history of alcohol and tobacco abuse. Presented initially with a debilitating and progressive sore throat. A: CT head shows a 2.0- × 2.9-cm left tonsillar mass (arrows).B: PET CT shows bilateral tonsillar masses (arrows). CT, Computed tomography; PET, positron-emission tomography.
Squamous cell carcinomas arise from tissues lined by squamous epithelium. Squamous cell carcinomas of the head and neck, regardless of site, share similar etiologies, pathogenesis, and response to therapy. In addition, the lymphoid tissues, neuroendocrine cells, melanocytes, and minor salivary glands may give rise to neoplasms. Such tumors are biologically distinct from squamous cell carcinomas and have different natural histories. Approximately 90% to 95% of oropharyngeal neoplasms are squamous cell carcinomas of the head and neck. Most oropharyngeal cancers originate from the base of the tongue and tonsils, and more than 90% of these are squamous cell carcinomas (Fig. 7.5). The majority (60%) of patients present with stage III/IV poor-prognosis disease.
Nasopharyngeal carcinoma is a unique form of head and neck cancer. It occurs at high frequencies in China and Southeast Asia. Nasopharyngeal cancer is a rare malignant disease in the Western world, with an incidence well under 1 per 100,000 persons per year in whites from North America and other Western countries. By contrast, the highest incidence is found among Southern Chinese (approximately 25 to 30 per 100,000 persons per year), especially those of Cantonese origin.88 The average age at diagnosis for this cancer is in the sixth decade of life, but a significant proportion of patients are diagnosed earlier, in their 20s and 30s. Nasopharyngeal carcinoma tends to metastasize early; distant metastases are found in 5% to 10% of patients at the time of initial diagnosis.89
Presenting signs and symptoms for head and neck cancers vary with the location of the primary tumor. Nasopharyngeal cancer frequently presents late with nodal neck metastasis. Nasal cavity and paranasal sinuses tumors often present with epistaxis or nasal obstruction. Diagnosis may be delayed as local symptoms may be attributable to other causes such Eustachian tube obstruction or cranial nerve dysfunction. Oral cavity cancers can present as nonhealing, painful ulcers. Laryngeal tumors may present as persistent hoarseness. Later symptoms include dysphagia, chronic cough, hemoptysis, stridor, and respiratory distress. Tumors of the oropharynx and supraglottic larynx usually present late with cervical lymph node enlargement, pain, otalgia, dysphagia, or dysphonia. Endoscopy with biopsy, such as laryngopharyngoscopy, is often used to facilitate the evaluation of the primary tumor. Approximately 15% to 30% of patients present with early-stage disease, and 60% to 80% present with locoregionally advanced disease. Distant metastasis at the time of presentation is not common, but preferential sites include the lung, mediastinal lymph nodes, bones, and liver. PET has a higher sensitivity than CT scan to detect occult metastasis.90, 91
Treatment of patients with locoregionally advanced or unresectable squamous cell carcinoma of the head and neck is complex and associated with significant toxicities. Local recurrences without evidence of distant metastases may be salvaged surgically if the primary therapy was radiation therapy or with radiation therapy if the primary therapy was surgery. Locally advanced, unresectable disease is best treated with concurrent chemotherapy and radiation therapy,92 particularly if patients have adequate functional status.
Surgery and radiation therapy are the primary treatment modalities for squamous cell carcinoma of the head and neck. Treatment options for cancers of the larynx present a somewhat unique situation because of patients’ desire to preserve vocal ability. In 1991, induction chemotherapy followed by radiotherapy became a standard treatment option for patients with advanced cancer of the larynx who wanted to preserve their voices.93
Only gold members can continue reading. Log In or Register to continue