Treatment of Locally Advanced, Metastatic and Recurrent Breast Cancer
|

Locally advanced disease of the breast is characterized by features suggesting infiltration of the skin, dermal lymphatics, involvement of chest wall by tumour, or matted involved axillary nodes. The clinical features include:
Peau d’orange.
Erythema (skin inflammation).
Direct skin involvement.
Satellite nodules.
Chest wall involvement.
Fixed or matted axillary nodes.
Large operable breast cancers and resectable tumours fixed to muscle should not be considered as locally advanced. A cancer may be locally advanced because of:
Biological aggressiveness (including inflammatory cancers).
The position in the breast (for example, peripheral or superficial).
As a consequence of neglect.
Locally advanced breast cancers require multidisciplinary management. The patient’s fitness and wishes are important in decision making.
Primary systemic therapy is often used initially in an attempt to downstage the tumour, which may allow such cancers to become operable. Conventional surgical resections are performed, most often mastectomy with axillary clearance, but breast conserving surgery is sometimes possible. Chemotherapy is preferred in the majority of fit patients but endocrine therapy, usually with letrozole, is an option for postmenopausal women with oestrogen receptor-rich cancers. Following surgery, patients will usually receive radiotherapy either to the breast or to the chest wall, due to the high risk of recurrent disease in these cases. Local radiotherapy can be of particular use in those women with large areas of skin involvement and to control areas of cancer which are fungating or bleeding.
Surgical resection of large areas of skin and underlying tissue is sometimes performed in an attempt to completely excise locally advanced tumours, but the resulting defect may require coverage with a myocutaneous flap, and consideration should be given to the involvement of a plastic or thoracic surgeon in the treatment of such women.
There is a major contribution from neglect in many elderly patients where the cancers often behave in a rather indolent manner and may be well-controlled by endocrine therapy alone if surgery is not feasible due to general frailty.
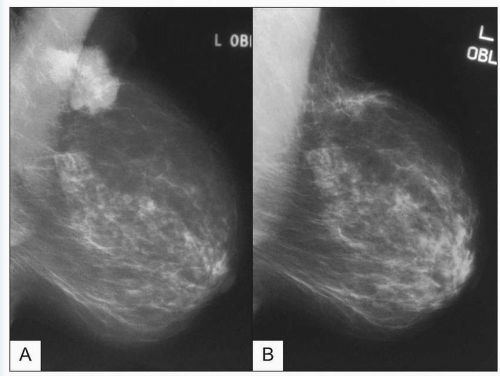 11.1A, B Mammograms showing response of an oestrogen receptor-bearing breast cancer to 3 months of hormonal therapy using the aromatase inhibitor, letrozole. |
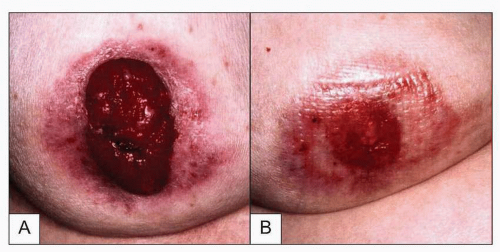 11.2 Locally advanced breast cancer before (A) and after (B) three months of treatment with letrozole showing a good response. A response to endocrine therapy like this may allow previously inoperable disease to become resectable. |
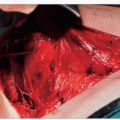
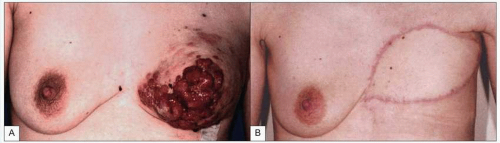 11.3A, B Latissimus dorsi flap for skin coverage. This patient presented with a locally advanced breast cancer with a large mass and multiple skin nodules. Following systemic therapy a mastectomy has been performed. The extent of disease required extensive skin resection leaving a wound which would not close primarily. To achieve skin closure and allow adequate resection, a latissimus dorsi myocutaneous flap has been performed. |