Addiction
Cessation
Cigarettes
e-Cigarettes
Nicotine
Smoking
Tobacco
Cigarette smoking continues to decline and is now at the lowest levels recorded in the history of the survey.
e-Cigarettes: This new product has made significant inroads among adolescents. Its prevalence among adolescents is now higher than the prevalence of tobacco cigarette smoking.
College students who use tobacco are more likely to be single, White, and engaged in other risky behaviors involving substance use and sexual activity. Based on the Surgeon General report from 2012, of every three young smokers (i.e., AYAs), one will quit and one will die from tobacco-related causes.1 The tobacco industry has overtly and heavily targeted young adult smokers, sponsoring events in bars and clubs, musical events, and movies popular with young adults.
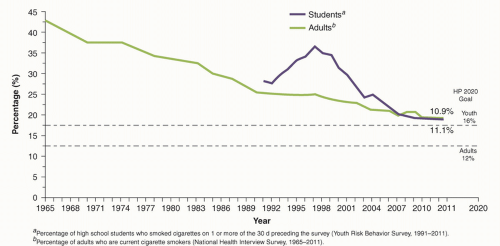 FIGURE 65.1 Trends in current cigarette smoking among high school students and adults, in the US, 1965 to 2011. (From the Centers for Disease Control and Prevention. Updated November 2013. Available at http://www.cdc.gov/tobacco/data_statistics/tables/trends/cig_smoking/) |
Each cigarette delivers 1 to 2 mg of nicotine to the smoker.
Each dose of the drug acts on the user within seconds of being inhaled.
smoking is even more dangerous than previously thought. Use of tobacco products can adversely affect virtually every organ system in the body (http://www.surgeongeneral.gov/library/reports/50-years-of-progress/). Some of these adverse effects include the following:
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Cardiovascular disease—coronary heart disease, stroke, atherosclerotic peripheral vascular disease, aortic aneurysm, early abdominal aortic atherosclerosis in young adults
Cancers—oropharynx, larynx, esophagus, trachea, bronchus, lung, stomach, pancreas, kidney and ureter, bladder, acute myeloid leukemia, colorectal
Diminished bone density and hip fractures
Pulmonary effects—chronic obstructive pulmonary disease and worsening asthma
Gastrointestinal effects—gastroesophageal reflux and peptic ulcer disease
Cataracts, blindness, and age-related macular degeneration
Premature wrinkling of the skin
PeriodontitisRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



