The incidence of thyroid cancer is rapidly rising in the United States and around the world.1 This is largely related to the routine use of ultrasound and imaging studies including CT scan, MRI, and PET scan in the evaluation of other conditions, which leads to the early identifications of thyroid nodules many of which after further analysis prove to be thyroid cancer. The incidence of thyroid cancer has almost quadrupled in the United States in the last quarter of a century from ˜8,000 cases per year in 1975 to the current incidence of 66,000 new thyroid cancers per annum. A much steeper rise in incidence has been seen in Korea where ultrasound of the neck is performed in a routine health check. The vast majority of these incidentally identified thyroid cancers are papillary carcinomas <2 cm in size, for which the 5-year survival exceeds 99.5%. However, the finding of thyroid cancer in each patient leads to intense concern about the diagnosis of cancer, often leading to aggressive treatment that is costly and, at times, morbid.
There is a current debate as to whether relatively more aggressive treatment will make a difference in long-term outcome, given that the outcome in patients with small papillary carcinomas is excellent. Thus, questions remain as to whether the routine use of total thyroidectomy with such patients is more likely to lead to improvements in survival that would justify the risk of laryngeal nerve palsy and temporary or permanent hypoparathyroidism. There is now a considerable interest both in Japan and in the United States to conduct observation studies on patients with microcarcinoma similar to prostate cancer to determine whether treatment of thyroid cancer is needed in all patients. Given the vast numbers of patients diagnosed and treated for thyroid cancer each year, the prognostic factors and risk group analysis are extremely well defined for patients with thyroid cancer that helps with the selection of how aggressively patients should be treated and which patients could potentially be observed closely rather than treated.
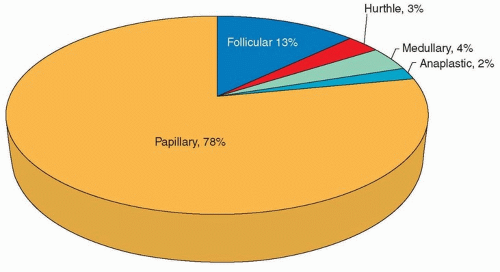
The majority of thyroid cancers are papillary carcinoma with follicular, Hurthle cell, anaplastic, and medullary carcinoma representing the remaining histologies that are most commonly seen (Fig. 19.1). Significant advances in the molecular biology of thyroid cancer have contributed to the way in which thyroid cancer is understood, diagnosed, and managed, as molecular testing now aids in predicting malignancy and prognosis in cytopathology samples. In addition, three drugs recently approved by the FDA for the treatment of advanced thyroid cancer are currently being used. With all of these new technologic developments currently available, it is important to continue to adhere to the principles of management of patients with thyroid cancer to avoid treatment-related complications both medical and surgical.
In this chapter, we will discuss the current understanding of thyroid cancer, pathology, prognostic factors and risk group analysis, available treatments, and overall outcomes. Current recommendations for evaluation, treatment, and surveillance are based on the wide experience of practitioners, investigators, and organizations such as the American Thyroid Association (ATA) and have led to publication of guidelines for the management of thyroid cancer first in 2006 and most recently in 2015.
THYROID CANCER: A UNIQUE HUMAN NEOPLASM
Thyroid cancer is a unique human neoplasm as the overall biologic behavior of thyroid cancer is characterized by slow-growing tumors with progression of disease over many years. Furthermore, this is the only human neoplasm where age is included in the staging system (Tables 19.1 and 19.2). In fact, here is no stage III or IV thyroid cancer in patients below the age of 45, which reflects the excellent outcome of these patients even in the setting of distant metastases. Age is an important prognostic factor, and even though age 45 is used as the general threshold in the staging system, it appears that the better age threshold is at 55.2 The presence of microscopic or “laboratory cancer” has very little clinical significance. It is not uncommon to find laboratory microscopic cancer in a thyroid gland removed for other medical issues. Such microscopic papillary cancers have an excellent prognosis and do not have any implication in the long-term outcome and do not require additional treatment. The presence of nodal metastasis in thyroid cancer is fairly common and is seen in almost 60% to 80% of younger individuals diagnosed with the disease. It has no major bearing in the overall outcome except in selective aggressive thyroid cancers or in older individuals.
An understanding of the histologic variations of thyroid carcinoma such as tall cell insular or poorly differentiated tumors and aggressive features is critical in the selection of treatment for patients in order to assure that they have the best possible outcome. In addition, these factors are important for the selection of adjuvant treatment and follow-up testing. The number of mitoses seen per high-power field on histologic examination is also important as a major prognostic feature, as are the findings of extrathyroidal extension and invasion of surrounding structures. It is critically important that the operating surgeon appreciate these clinical features and perform adequate and appropriate surgery including resection of the surrounding involved structures to achieve a complete resection in order to avoid future locoregional recurrence.
Figure 19.1. Histologic distribution of thyroid tumors.
Tumor 2 cm or less in its greatest dimension, limited to the thyroid
T2
Tumor more than 2 cm, but not more than 4 cm in its greatest dimension, limited to the thyroid
T3
Tumor more than 4 cm in its greatest dimension limited to the thyroid or any tumor with minimal extrathyroidal extension (e.g., extension to sternothyroid muscle or perithyroid soft tissues)
Metastasis to level VI (pretracheal, paratracheal. and prelaryngeal/Delphian lymph nodes)
N1b
Metastasis to unilateral, bilateral, or contralateral cervical or superior mediastinal lymph nodes
Distant metastasis (M)
MX
Distant metastasis cannot be assessed
M0
Mo distant metastasis
M1
Distant metastasis
aAll categories may be subdivided: (I) solitary tumor, (ii) multifocal tumor (the largest determines the classification).
bAll anaplastic carcinoma are considered T4 tumors: T4a—intrathyroidal anaplastic carcinoma (surgically resectable); T4b—extrathyroidal anaplastic carcinoma (surgically unresectable).
cRegional lymph nodes are the central compartment, lateral cervical, and upper mediastinal lymph nodes.
Used with the permission of the American Joint Committee on Cancer (AJCC), Chicago, Illinois. The original source for this material is the AJCC Cancer Staging Manual, Seventh Edition (2010) published by Springer Science and Business Media LLC, www.springer.com.
Despite all that is known about the biologic behavior of differentiated thyroid cancer, there are several controversies that remain regarding its management. One major area of controversy has been a subject of debate in national and international conferences and the literature abounds with publications describing the extent of thyroidectomy and whether treatment with thyroid lobectomy versus total thyroidectomy is the most appropriate way to manage patients with early-stage differentiated cancer. Two additional areas of controversy are (1) the use of radioactive iodine ablation in patients with low-risk thyroid cancer and (2) whether prophylactic central compartment dissection should be performed in patients with low-risk thyroid cancers. These controversies generate considerable debate, and this has been reflected in the evolution of the ATA guidelines for thyroid cancer treatment from 2006 to 2015.
aAny anaplastic carcinomas are considered Stage IV.
Used with the permission of the American Joint Committee on Cancer (AJCC), Chicago, Illinois. The original source for this material is the AJCC Cancer Staging Manual, Seventh Edition (2010) published by Springer Science and Business Media LLC, www.springer.com.
EPIDEMIOLOGY
The National Cancer Institute has reported that 62,980 people will be diagnosed with thyroid cancer, and 1,890 people will die of this disease in the United States this year. The risk for thyroid cancer is three times more prevalent in women than men and more common in Caucasians. The probability of being diagnosed with thyroid cancer peaks between 35 and 44 years of age. Although the diagnosis of thyroid cancer affects young patients, the percent of thyroid cancer deaths is highest among older patients with the median age of death being 73 years. Rates for new thyroid cancer cases have been rising on average 5.5% each year over the last 10 years. This increase in incidence is not isolated to the United States as the rise in thyroid cancer has been observed over the last three decades all over the world. The exception to this trend is in Africa, where detection may be insufficient. Importantly, death rates have also been rising on average 0.8% each year over 2002 to 2011.3 Many have hypothesized on the reasons behind the rising incidence of thyroid cancer, and explanations for the worldwide increase in thyroid cancer incidence are a source of controversy. The recent advances in imaging studies such as ultrasound, CT scan, MRI, and PET scan have identified exceedingly high number of incidental thyroid cancers, which are generally microcarcinomas. This is directly related to the increased usage of ultrasound and other imaging studies of the neck in the evaluation of other conditions including carotid vascular disease, cervical spine problems, and trauma. Many institutions have routine health checks with ultrasound of the neck as well as ultrasound of the breast. This practice of performing routine ultrasound of the neck has led to an exceedingly high incidence of thyroid cancer in South Korea where the incidence has risen almost 15-fold in the last 15 years.1 Although it is generally accepted that early detection of cancers is generally associated with better outcomes and has led to screening for prostate and breast cancer, the impact of the early identification of papillary microcarcinomas on patient survival remains unclear at this time, and further studies are needed to determine the most appropriate management that will lead to good survival, low morbidity, and appropriate utilization of health care resources.
INCIDENTALLY DIAGNOSED THYROID CANCER
Many thyroid cancers are identified as an incidental finding during the evaluation of other conditions or during screening tests, and these otherwise asymptomatic cancers can therefore be referred to as “incidentalomas.” Incidentalomas are fairly common in the thyroid gland. This terminology was previously used routinely for adrenal lesions, and it is now commonly used for thyroid nodules found “incidentally” without clinical symptoms or suspicion. Approximately 5% to 10% of individuals have thyroid nodules; however, many of these may remain clinically silent in the lifetime of the individual.
Clinical incidentalomas are commonly noted in routine clinical examination either by a primary care physician or during an ENT examination. Imaging incidentalomas can be divided into ultrasound of the neck, CT scan, MRI, or PET. These are more common when a patient undergoes routine imaging of the neck for other medical problems such as trauma, neck pain, or neurovascular conditions. Once a thyroid nodule has been identified by one of these studies, further evaluation including an ultrasound and needle biopsy may lead to the diagnosis of cancer.
We are seeing more and more incidentalomas related to the use of PET, which raises a suspicion of cancer in the mind of the radiologist and the oncologist. Incidentalomas identified by PET need to be divided into those with diffuse and those with focal uptake. Diffuse uptake is more likely related to nodular hyperplasia and Hashimoto thyroiditis, although the latter condition may also have areas of focal uptake, suggestive of malignancy.
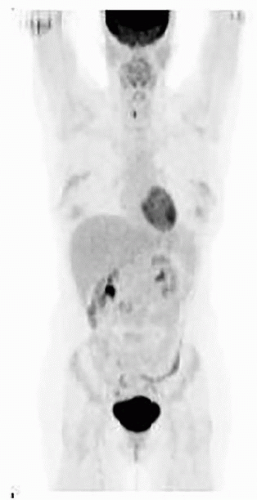
Once a focal incidentaloma is noted on PET, it is important to proceed with ultrasound and based on the findings of the ultrasound consider ultrasound-guided needle biopsy. Katz and Shaha4 have described their experience and review of PET-associated incidental neoplasms (PAIN) and have noted that the incidence of malignancy in selectively operated patients is ˜50%, whereas a large number of these patients have aggressive histology such as tall cell tumor, Hurthle cell tumors, or oncocytic malignant tumors. Figure 19.2 demonstrates a thyroid nodule indecently found by PET scan. In summary, the focal PET hypermetabolic thyroid nodule needs to be further evaluated with ultrasound and possible ultrasound-guided needle biopsy.
ANATOMY
The thyroid gland includes two lateral lobes, connected by a central isthmus. Often, a vestigial remnant of the thyroglossal duct tissue extends as a finger-like projection superiorly from the thyroid isthmus to make up a third, “pyramidal lobe” of the gland. Two ligaments “attach” the thyroid from the cartilaginous airway. The anterior suspensory ligament arises from the anterior aspects of tracheal rings and inserts on the posterior aspect of the thyroid isthmus. Condensation of the thyroid capsule forms the posterior suspensory ligament (ligament of Berry) and connects the posteromedial aspect of the gland to the tracheal rings and cricoid cartilage. In contrast to the avascular plane characteristic of the anterior suspensory ligament, an arterial and venous plexus course through the posterior suspensory ligament and can be a source of bleeding during thyroidectomy.
Figure 19.2. PAIN (PET-Associated Incidental Neoplasm). Lesions found incidentally on PET scan have a higher rate of malignancy.
The arterial and venous supply to the thyroid must be meticulously dissected and ligated during thyroid surgery. Arterial anatomy includes paired superior thyroid arteries arising as the first branch of the external carotid artery and paired inferior thyroid arteries arising from the thyrocervical trunks. An unpaired thyroid ima artery may arise from the innominate artery, carotid artery, or directly off the aortic arch. Attention to hemostasis and keen attention to vascular structures associated with the thyroid gland are important in avoiding postoperative hematoma.
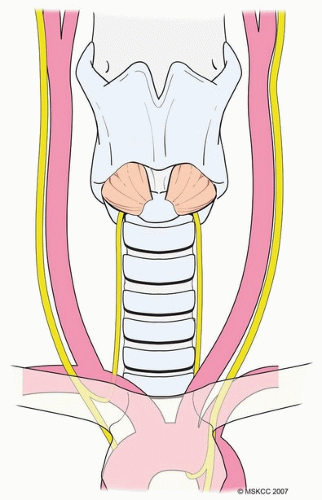
Identification and preservation of the nerves arising from the vagus nerve during thyroid surgery require a thorough knowledge of the anatomy as well as surgical skill. The recurrent laryngeal nerve (RLN) innervates all intrinsic muscles of the larynx except the cricothyroid muscle. The left RLN branches from the vagus nerve and then descends into the chest passing inferior and posterior to the aortic arch. In contrast, the right RLN leaves the vagus nerve at the base of the neck and loops around the subclavian artery. This results in the more lateral location of the right RLN versus the left RLN in the neck as both nerves ascend in tracheoesophageal groove before entering the larynx at the cricothyroid joint (Fig. 19.3). The nerve may be split into multiple branches or into two major branches anterior and posterior. It is the anterior branch that carries motor fibers and is more functionally important for the mobility of the vocal cord.
Figure 19.3. The left RLN branches from the vagus nerve and then descends into the chest passing inferior and posterior to the aortic arch. The right RLN leaves the vagus nerve at the base of the neck and loops around the subclavian artery. This results in the more lateral position of the right RLN.
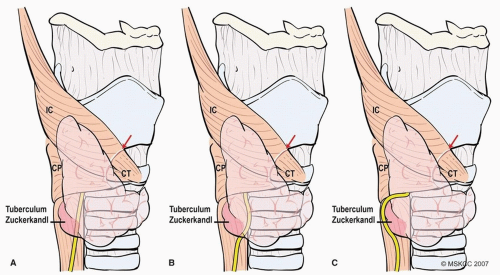
Most of the time, nerve injury is related to thermal injury or traction injury rather than direct transection of the nerve. It is also important to recognize that the entry point of the RLN is a fixed point, and therefore, stretch injury when retracting the thyroid medially during surgery can also occur. The anatomical identification of the tuberculum Zuckerkandl can aid in the identification of the RLN. This anatomic structure is present in majority of the patients with thyroid pathology. It is a small outpouching of the thyroid tissue, which forms a tiny tubercle near the ligament of Berry. Often, the nerve is posterior and slightly medial to the tuberculum Zuckerkandl and is a good landmark for identification of the RLN (Fig. 19.4A and B). Occasionally, the tuberculum of Zuckerkandl may displace the RLN laterally around it, placing the nerve at risk for injury if this variation is not recognized (Fig. 19.4C). The nerve may be intimately adherent to this region, which could also predispose it to injury.
There are three areas where the RLN can be injured. The first is in the tracheoesophageal groove, which is often encountered during the dissection of the lymph nodes in the tracheoesophageal groove. This is the same area where the nerve may be traumatized due to adherence of the lymph nodes or more importantly while dissecting the nerve off the lymph nodes. The nerve may also be injured at the crossing of the inferior thyroid artery. In the majority of the time, the nerve crosses behind the inferior thyroid artery; however, in ˜25% of patents, the nerve may be superficial to the inferior thyroid artery where the identification of the nerve may be difficult and inadvertently traumatized. The most common injury to the RLN occurs near the ligament of Berry. The most common reason for injury to the RLN in this region is that small blood vessels travel through the ligament of Berry causing excessive bleeding during surgery, and the nerve injury may occur in an effort to control the bleeding in this region especially when electrocautery is used. Occasionally, the laryngeal nerve may be nonrecurrent, and identification of the nonrecurrent nerve is critical in order to avoid unanticipated injury. As this anatomic variant is associated with an aberrant innominate artery or retroesophageal subclavian artery, a preoperative CT scan revealing these vascular anomalies can raise the surgeon’s vigilance for identification of a nonrecurrent nerve. Generally, the presence of a retroesophageal innominate artery (arteria lusoria) leads to the innominate abnormality of being a nonrecurrent RLN. In such patients, extreme care must be undertaken to evaluate the area between the carotid artery and ligament of Berry to avoid injury to the nonrecurrent nerve. The use of a nerve monitor may be extremely helpful in such patients. Generally, the nonrecurrent nerve is identified either at the ligament of Berry or in the region lateral to the superior pole of the thyroid. Occasionally, the vagus nerve may be medial to the carotid artery, which is also an indication of patient having nonrecurrent RLN.
Figure 19.4. A and B: The RLN lies posterior and slightly medial to the tuberculum Zuckerkandl and is a good landmark for identification of the RLN. C: Occasionally, the tuberculum of Zuckerkandl may displace the RLN laterally around it, placing the nerve at risk for injury.
Another important nerve to identify during thyroid surgery is the external branch of superior laryngeal nerve (EBSLN), which has also been called the “Amelita Galli-Curci,” nerve after the famous Italian opera singer whose career declined after she underwent a thyroidectomy. Although less discussed, injury to the (EBSLN) has been estimated to occur in 0% to 53% of thyroidectomies.5,6 The superior laryngeal nerve originates from the vagus nerve just below the jugular foramen. It then divides into an internal and external branch. The EBSLN descends inferiorly to innervate the cricothyroid muscle. Cernea anatomically classified variants of the EBSLN.7 Type 1 nerves cross >1 cm above the upper border of the thyroid gland. Type 2a nerves cross within 1 cm of the upper border of the thyroid. Type 2b nerves cross below the upper border of the gland. The external branch of the superior laryngeal nerve is at risk for injury during ligation of the superior thyroid vascular pedicle most often in patients with the type 2b variant. Patients with injury to the EBSLN during thyroidectomy will complain of inability to yell or “hit a high note.”
The superior parathyroid glands (“deep” parathyroids) are derived from the fourth branchial pouch.
Anatomically, these glands exist “deep” to the RLN anatomically. This relationship can change when retracting the thyroid medially during surgery. Classically, the superior parathyroid glands are described as located 1 cm above the intersection of the RLN and inferior thyroid artery. Inferior parathyroid glands (“superficial” parathyroids) are derived from the third branchial pouch. These glands exist superficial to the RLN and are more variable in location. The thymus is also derived from the third branchial pouch, which is why inferior parathyroids are sometimes located in the anterior mediastinum within the thymus.
EVALUATION OF THE THYROID NODULE
Thyroid nodularity is quite common and has been reported to be detected as a palpable nodule in 4% to 7% of the adult population. When imaging is used to evaluate the thyroid, the incidence of nodules identified increases to >50%.8 Most clinically detected nodules are benign, and the incidence of occult cancer within the thyroid gland ranges from 4% to 35% in adults in autopsy studies. Strikingly, this number approaches 100% in elderly patients.
Generally, nodules >1 cm should be further evaluated for the presence of cancer. However, there are nodules that do not meet this size criterion that should also be evaluated based on suspicious features. Table 19.3 highlights these features including suspicious ultrasound (US) findings, associated lymphadenopathy, a history of head and neck irradiation, or a history of thyroid cancer in one or more first-degree relatives. Additionally, nodules found incidentally on PET scan have a risk of malignancy of about 33% and may be more aggressive and therefore should be evaluated even if <1 cm.9 Importantly, the new version of the ATA guidelines recommend not biopsying lesions under 1 cm given the increased interest in observation as a treatment option for subcentimeter PTCs.
Evaluation of a thyroid nodule should include a full history and physical examination. Risk factors, summarized in Table 19.4, include radiation to the head and neck during childhood for cancer or dermatologic pathology such as acne or dermatitis, exposure to radiation secondary to fallout from nuclear accidents such as occurred in Chernobyl, a family history of thyroid carcinoma, or thyroid cancer syndromes such as Cowden, familial polyposis, or type 2 multiple endocrine neoplasia (MEN 2). A history of rapid growth or hoarseness should raise suspicion for malignancy. Physical examination should include the thyroid gland, lateral cervical lymph nodes, and laryngeal examination.
Table 19.3 Indications for FNA of Thyroid Nodules <1 cm
Suspicious US findings
Associated lymphadenopathy
History of head and neck irradiation
History of thyroid cancer in first-degree relatives
18FDG-positive nodules
Adapted from ATA Guidelines 2009 version.
Table 19.4 Clinical Features of a Malignant Thyroid Nodule
Age—Very Young or Very Old
Sex—Male
History of thyroid cancer syndromes
Hoarseness-vocal cord paralysis
Hard, Fixed Nodule
Rapid Growth
New onset of rapid growth in a longstanding stable nodule
Cervical Metastases
Pulmonary Metastases
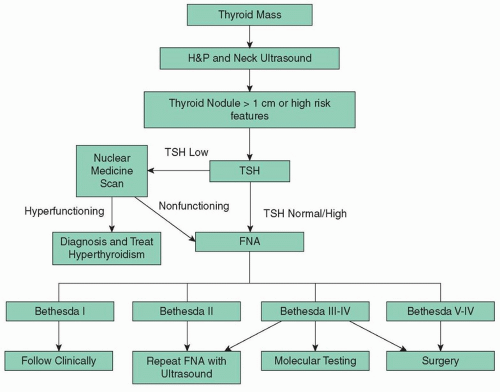
In the clinically apparent or incidentally found thyroid nodule, a TSH level should be ordered to differentiate functioning from nonfunctioning nodules. If the TSH is low, then a hyperfunctioning nodule should be considered and a radionuclide thyroid scan can be obtained. Hyperfunctioning nodules rarely harbor malignancy, if one is found that corresponds to the nodule in question, no cytologic evaluation is necessary. In contrast, if the TSH is normal or low, further cytologic evaluation is indicated. Interestingly, high TSH has been associated with a higher risk of malignancy.10 With biochemical evaluation, radiographic assessment is essential in the evaluation of thyroid nodules. Ultrasound of the thyroid gland and lateral neck provides valuable information. First, is there a nodule that correlates to a palpable or radiographic abnormality? If so, how big is it, where is it located with regard to the strap muscles, RLN, or airway? Is it cystic or solid? Completely cystic nodules have a low likelihood of malignancy.11 Are there other nodules within the gland? Does the nodule have any suspicious findings? Ultrasound characteristics associated with a higher rate of malignancy include hypoechogenicity, increased intranodular vascularity, irregular infiltrative margins, microcalcifications, an absent halo, and taller than the wider diameter. Findings of isoechogenicity and spongiform appearance are more common in benign nodules.12Table 19.5 summarizes ultrasound findings, which are useful in distinguishing benign from malignant lesions. Is there concerning lymphadenopathy? Ultrasound can also help guide fine-needle aspiration (FNA) in nodules that are nonpalpable, partially cystic, or posteriorly located. FNA is the workhorse for cytologic and molecular assessment of thyroid nodules. Cytologic evaluation is classified by the Bethesda System for Reporting Thyroid Cytopathology13(Table 19.6).
Table 19.5 Ultrasound Finding in Thyroid Nodules
Benign Features
Malignant Features
Pure cystic nodule
Spongiform appearance
Benign nodules
Micro- or Macrocalcifications
Marked hypoechogenicity
Taller-than-wide shape
Spiculated margin
From Moon WJ, et al.; Thyroid Study Group, Korean Society of Neuro- and Head and Neck Radiology. Benign and malignant thyroid nodules: US differentiation—multicenter retrospective study. Radiology. 2008;247(3):762-770.
Table 19.6 Bethesda Criteria
Bethesda Criteria
FNA Result
Chance of Malignancy
I
Nondiagnostic or Unsatisfactory
1%-4%
II
Benign
0%-3%
III
Atypia of Undetermined Significance Follicular Lesion of Undetermined Significance
5%-15%
IV
Follicular Neoplasm or Suspicious for a Follicular Neoplasm
15%-30%
V
Suspicious for Malignancy
60%-75%
VI
Malignant
97%-99%
From Cibas ES, Ali SZ. The Bethesda system for reporting thyroid cytopathology. Am J Clin Pathol. 2009;132(5):658-665.
Molecular testing may provide further information on thyroid nodules including risk of malignancy and prognosis. Afirma is a molecular test used in indeterminate nodules by FNA (Bethesda III and IV) as a “rule out test.” This test takes into account mRNA expression levels in a 164-gene panel. This Gene Expression Classifier (GEC) provides results that are either benign (<6%) or suspicious (40% chance of malignancy) with a negative predictive value of 94%.14 The majority of the clinicians will use this information to consider surgery especially if the Afirma is reported to be suspicious.
However, it is important to appreciate the risk of malignancy is still ˜40% and not 100%. Afirma is also more likely to be positive in patients presenting with Hashimoto thyroiditis, and it is always confusing in Hurthle cell lesions as it invariably turns out to be suspicious. Obviously, some of these decisions are best made by the clinician based on other clinical and radiologic features and parameters. ThyroSeq Thyroid Cancer Next-Generation Sequencing Panel is also used in indeterminate nodules by FNA (Bethesda categories III, IV, V) and malignant nodules when molecular testing is expected to affect the decision to perform surgery or extent of surgery. Mutations in thyroid cancer-related genes and gene fusions are detected by next-generation sequencing. This may also be useful in clinical decision making with regard to administration of radioactive iodine, intensity of follow-up, and targeted therapies.15 An algorithm for the evaluation of the thyroid nodule is provided in Figure 19.5.
Figure 19.5. Evaluation of thyroid nodule.
MOLECULAR BIOLOGY OF WELL-DIFFERENTIATED THYROID CANCER
Noteworthy advances in the understanding of the molecular biology of thyroid cancer are beginning to be incorporated into clinical practice. The Cancer Genome Atlas Research Network recently reported on genomic landscape of 496 papillary thyroid cancers (PTCs).16 The genome of PTC is described as relatively “quiet,” as compared to other cancers as defined as a low frequency of somatic alterations, and this may offer a biologic basis for the indolent clinical behavior of PTCs. Common known drivers will be discussed in greater detail.
Proto-oncogenes Associated with Thyroid Cancer
Chromosomal Rearrangements (RET/PTC)
Rearrangement of the RET proto-oncogene RET results in the aberrant production of chimeric forms of the receptor (RET/PTC) in thyroid cells, which leads to constitutive activation of several downstream pathways, including mitogen-activated protein kinase (MAPK), extracellular signal-related kinase (ERK), and phosphatidylinositol 3-kinase (PI3K). This rearrangement has been observed in post-Chernobyl pediatric thyroid cancers (RET/PTC1) and has been associated with classical PTC, as well as solid variant PTCs (RET/PTC3).17
Ras Oncogenes
The 3 classical Ras proto-oncogenes encoding Hras, Kras, and Nras belong to an extended family of small G proteins. Ras mutations are found in follicular adenomas and carcinomas18 and are also observed in 13% of PTCs.16,19 Ras mutations are thought to be an early event in thyroid cancer genesis and some have shown they follow a more aggressive clinical course.20
BRAF and MAP Kinase Signaling Pathway
The BRAF missense mutation in exon 15, which leads to the substitution of the amino acid valine for glutamic acid at residue position 600, is the most frequent genetic change in PTC and has been observed in 60% of tumors.16 Mutant BRAF is a potent activator of the downstream effectors, the MAP kinases in the Raf-MEK-ERK pathway, which mediate cellular responses to growth signals. Clinically, PTCs with BRAF mutations are more common and are associated with an aggressive clinical course including extrathyroidal invasion, greater rates of recurrence, and treatment failure,21 which translates into worse clinical outcomes.22
BRAF mutation has also been shown to be responsible for the suppression of expression of the sodium/iodide symporter (NIS) leading to RAI resistance.23 Inhibitors of the BRAF kinase have been developed and show promise in treating several cancer types. However, development of resistance to BRAF kinase inhibitors is common. In addition, inhibitors of the MAP kinase pathway have been developed and are beginning to be used clinically.
Well-Differentiated Thyroid Cancers
Papillary and follicular carcinomas collectively grouped as differentiated thyroid cancer constitute more than 90% of all malignant neoplasms of the thyroid gland. These two entities share similar diagnostic and treatment algorithms and have an overall excellent prognosis of 97.8% at 5 years when diagnosed and treated appropriately.
Staging and Prognostic Schemas
Cancer staging is an essential prognostic tool that is integral part of cancer management. The familiar tumor-nodal-metastasis (TNM) staging system is the most widely applied staging system in thyroid cancer. Unique to thyroid cancer, age at diagnosis is incorporated in the staging system reflecting its marked influence on outcome. The American Joint Committee on Cancer (AJCC) 7th edition (Tables 19.1 and 19.2) has been shown to predict differentiated thyroid cancer-related death.24 The prognostic factors in thyroid cancer are well defined and reported from several independent datasets, starting from the EORTC study published in 1979.25 In the United States, Cady of the Lahey Clinic and Hay et al. of the Mayo Clinic reported similar prognostic factors in the 1980s.26,27 The Mayo Clinic revisited their data and included completeness of resection as an important prognostic factor leading to their acronym of MACIS.28 Memorial Sloan Kettering Cancer Center subsequently also suggested similar prognostic factors with the acronym GAMES (grade of the tumor, age, distant metastasis, extrathyroid extension, and size of the tumor).29 These schemas are summarized in Table 19.7. A risk-stratified approach has also been adopted in the ATA guidelines and is summarized in Table 19.8.
Only gold members can continue reading. Log In or Register to continue