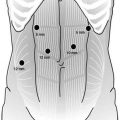
Fig. 16.1
Arrangement of ports in thoracoscopic approach. AAL anterior axillary line, MAL midaxillary line, PAL posterior axillary line
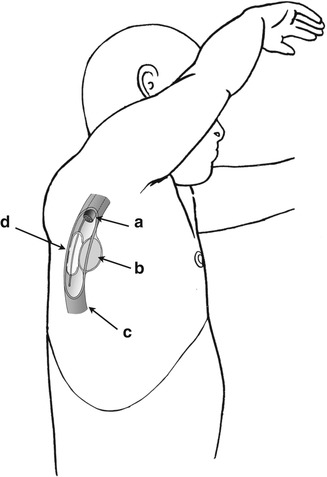
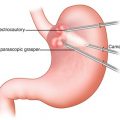
Fig. 16.2
The esophageal tumor is pushed away from the esophageal wall using a balloon-mounted esophagoscope. (a) esophagoscope, (b) esophageal leiomyoma, (c) esophagus, and (d) balloon
After that blunt dissection was performed separating the tumor from the mucosa, followed by applying traction suture to the tumor to aid in tumor elevation as well as in the dissection which was done mostly by blunt dissection (Fig. 16.3a). After tumor enucleation, the specimen was placed in a retrieval bag introduced through anterior 10-mm trocar and was delivered through this trocar wound. The dissected area is thoroughly examined by endoluminal endoscopic inspection after air insufflation of the esophagus. Finally, the esophageal muscle layer is carefully closed using interrupted sutures to prevent the development of a pseudodiverticulum; a chest tube is also routinely inserted via a thoracoscopic approach (Fig. 16.3b). An alternative method for thoracoscopic resection of an esophageal leiomyoma is demonstrated in Video 16.2.
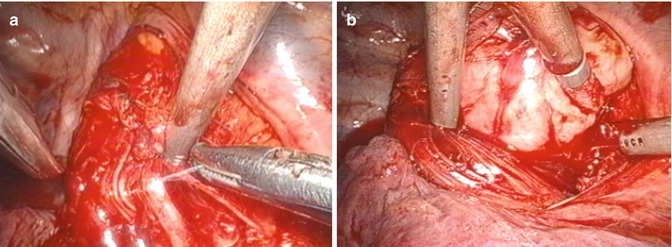
Fig. 16.3
Thoracoscopic enucleation for an esophageal leiomyoma. (a) The tumor was removed gently with particular attention for not damaging mucosa. (b) The esophageal muscle layer was carefully closed using interrupted sutures to prevent the development of pseudodiverticulum
Laparoscopic Transhiatal Approach
A laparoscopic transhiatal approach is routinely used for tumors of the lower third of the esophagus. With the patient in a supine position, a pneumoperitoneum is established after the placement of a 12-mm trocar into the subumbilical area, using an open technique; CO2 insufflation, to a pressure of 10 mmHg, is then maintained. Five trocars are inserted into the upper abdomen, and the phrenoesophageal ligament and the short gastric vessels are divided using a Harmonic scalpel (Johnson & Johnson Medical, Cincinnati, OH, USA). After dissection of the abdominal esophagus, a Penrose drain is placed around the esophagus to aid in esophageal retraction; dissection of the abdominal esophagus is very similar to a fundoplication dissection. After the esophageal SMT is identified, it is enucleated via a laparoscopic transhiatal approach, and a Dor or Toupet fundoplication was performed to restore the integrity of the anti-reflux mechanism.
Clinical and Technical Points
The first successful resection and enucleation of a benign esophageal tumor was reported by Sauerbrach in 1932 [10]. Traditionally, tumors of the upper and middle thirds of the esophagus have been approached by a right thoracotomy and tumors of the lower third have been approached by a left thoracotomy. Surgical enucleations of esophageal leiomyomas by video-assisted thoracoscopic surgery have also been reported and have contributed to the growing interest in the use of this approach in recent years [5, 11, 12]. There are some clinical and technical points that should also be considered during thoracoscopic/laparoscopic enucleations of esophageal leiomyomas. First, the myotomy must be performed in the correct direction and at the right level, and appropriate traction must be applied on the tumor to facilitate its subsequent enucleation. Second, a balloon-mounted esophagoscope allows the localization of small tumors and permits the confirmation of mucosal integrity and ensures safety. Third, an anti-reflux operation needs to be performed to restore the integrity of the anti-reflux mechanism, following dissection and mobilization of the esophagogastric junction and as a means of covering the myotomized esophageal mucosa. Finally, the difficulty of the cases, and thus, patient selection should be carefully considered. Conversion to an open procedure should be considered in cases in which technical problems or limitations are noted.
Related posts:
 Multimodality Therapy in Gastric Cancer
Multimodality Therapy in Gastric Cancer
 Minimally Invasive Feeding Tube and Esophageal Stent Placement
Minimally Invasive Feeding Tube and Esophageal Stent Placement
 Robotic Utilization in Esophageal Cancer Surgery
Robotic Utilization in Esophageal Cancer Surgery
 Standards for Surgical Therapy of Gastric Cancer
Standards for Surgical Therapy of Gastric Cancer
 Laparoscopic Partial Gastrectomy
Laparoscopic Partial Gastrectomy
 Laparoscopic and Thoracoscopic Transhiatal Esophagectomy with Cervical Anastomosis
Laparoscopic and Thoracoscopic Transhiatal Esophagectomy with Cervical Anastomosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


