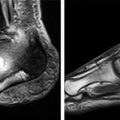
Figure 12.1
(a) Charcot changes in the tarso-metatarsal joints with subluxation of the lateral four rays, going laterally, so that the space between the first and second metatarsals is increased (arrowed). This foot is unstable, although the forefoot and hindfoot are virtually unaffected. (b) Collapse at the midfoot in the same patient is obvious, and the bony prominences in the midfoot are indicated with arrows. There is fragmentation dorsally and dorsal subluxation of the base of the first metatarsal. (c) The foot has been stabilised with screws across the second and third tarsometarsal joints and a locking plate to reduce and hold the first tarsometatarsal joint
Clinical Management
The Infected Diabetic Foot
Osteomyelitis is common in diabetics with an established ulcer, but the diagnosis and management present challenges and must be tackled in a multi-disciplinary way to optimise the chance of clearing the infection. This will involve input from vascular and orthopaedic teams, as well as a microbiologist, diabetologist and a nursing/tissue care team. Some form of surgery is usually required, be it surgical sampling and debridement of the wound, or more extensive resection, amputation or stabilization.
It is unusual to have a diabetic foot infection without an obvious portal of bacterial entry, most commonly a neuropathic ulcer. It is important to distinguish superficial colonisation from true infection, so superficial swabs are of little value; tissue samples are needed, from the soft tissues and from bone if this is accessible through the wound or ulcer [2].
For acute sepsis or spreading infection, empirical antibiotic therapy might be used, aimed at Gram-positive cocci. It is better, however, to have tissue culture and antibiotics targeted at the appropriate organism, which is often antibiotic-resistant, especially in chronic or previously treated cases. Locally agreed protocols are important in guiding the acute care teams who may be initially admitting these cases, and should be agreed by the multi-disciplinary team.
If the foot is mechanically unstable as well as infected, the orthopaedic surgeon may have a particular part to play in providing stability through the limited use of internal or external fixation. The techniques of fixation will include standard plates and screws, as well as potentially some novel stabilization with long bolts and screws specifically designed for use in the diabetic foot. These provide intramedullary support from the metatarsals in the forefoot through into the midfoot and on into the talus. This offers cantilever beam support for the foot. Techniques are being developed to place a fixation plate on the plantar aspect of the foot skeleton, the tension side of the collapsing foot, working as a tie-beam support. The normal concerns about not putting metalwork into an infected area might be set aside in these cases, as stability is itself important in providing an environment in which the infection can be treated effectively. If the foot heals and infection is controlled, then the metalwork could potentially be removed later if there are fears that it is itself colonised with bacteria.
Suspected Charcot Disease
Diabetes is the most common cause of Charcot foot in the developed world, but it is still a relatively rare complication, affecting approximately 1 % of diabetics. The patient has usually had known diabetes for more than a decade, and is in their fifth or sixth decade of life. The presentation is often with a hot, warm and swollen joint or foot, without much pain. The mismatch between minimal pain but severe disruption and fragmentation on x-ray is typical.
There is sometimes a debate as to whether or not the foot is infected or whether there is inflammation from a Charcot foot – the former is unusual unless there has been a breach of the skin, and in the latter the redness goes when the foot is elevated for 10 min.
The most characteristic x-ray pattern is one of fragmentation or fracture around the ankle and forefoot, with subluxation or dislocation in the mid-foot, particularly at the mid-foot/fore-foot junction (the Lisfranc joints).
Special investigations such as MRI or bone scanning are difficult to interpret, as they do not give a reliable distinction between Charcot and infection; they are sensitive, but lack specificity. These investigations may, however, be useful in assessing the extent of either of those processes.
Related posts:
 Foot Deformity and Pressure Management in the Diabetic Foot
Foot Deformity and Pressure Management in the Diabetic Foot
 Screening and Treatment of Early Complications in the Diabetic Foot
The Role of the Multidisciplinary Team in the Management of Diabetic Foot Complications
Screening and Treatment of Early Complications in the Diabetic Foot
The Role of the Multidisciplinary Team in the Management of Diabetic Foot Complications
 Imaging in the Patient with Foot Complications
Imaging in the Patient with Foot Complications
 Neuro-osteoarthropathy: The Charcot Foot – Pathology, Diagnosis, and Treatment
Neuro-osteoarthropathy: The Charcot Foot – Pathology, Diagnosis, and Treatment
 Endovascular Revascularisation: When and How
Endovascular Revascularisation: When and How
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


