Chapter 25 THE OLDER PERSON WITH PERSONALITY DISORDER
INTRODUCTION
Personality disorders are characterised by deeply embedded, inflexible, maladaptive, overt traits characterised by dysfunctional personal relationships and cognitive, emotional, impulse control difficulties. These characteristics result in the older person encountering problems in perceiving and interpreting situations, having blunted or exaggerated emotional responses, ineffectual dealings with other people or a lack of restraint in challenging situations. Old age brings new stressors for people, particularly in relation to losses such as employment, social networks and health. For an older person with a personality disorder, there may be increased stress due to their difficulty in adapting to changes and new situations, rigid behaviours limiting relationship development and their propensity for damaging relationships.
CASE VIGNETTE
Doris, a 68-year-old widow, lived alone in a small cottage in an inner-city suburb. She had a longstanding diagnosis of obsessive-compulsive personality disorder but her severe arthritis was limiting her physical capabilities to the extent she soon required permanent placement in a residential aged care facility (RACF). Doris had one daughter who was affected by depression and they did not have a close relationship, so it was not practical to consider the daughter as capable of supporting her mother on an ongoing basis. Doris’s obsessive-compulsive behaviour was obvious in her excessive and pedantic approach to housework, which was done overnight so that no one saw her. In addition to the impact the arthritis was having on her need to tend to the housework, the anxious aspects of her obsessive-compulsive personality disorder were making her adjustment to the prospect of moving into an RACF very complicated.
PERSONALITY
Personality is defined as a person’s pattern of psychological processes, which includes motives, feelings, thoughts, behaviour patterns, and other areas of psychological functioning. It is expressed through its influences on the body, in conscious experience and through social behaviour. It is generally stable over time (Mayer 2006, cited in Segal et al 2006).
A personality trait is a characteristic of the personality which makes a person unique. To be a trait it has to be a persistent and pervasive characteristic. Each person has a number of traits which contribute to their personality. For example, a person may be described as shy and retiring, whereas another is loud and boisterous; some people are impetuous or insensitive, whereas others are more thoughtful and considerate. The list is endless (Segal et al 2006).
People have a mix of personality traits. Some are flexible and responsive, whereas others are the opposite and not very attractive. In healthily functioning individuals, the positive traits are persistent and pervasive and negative traits are only exhibited when necessary or fleetingly. However, not everyone has an adaptive personality style and with some people negative traits are more prominent. For example, they may be described as aloof, rigid, hostile, egocentric or shallow to the extent that their personality style limits their ability to function appropriately on an everyday basis. This is when a person may be said to have a personality disorder (Segal et al 2006).
EPIDEMIOLOGY
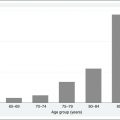
The prevalence of personality disorders in older people living in the community is reported as being between 10% and 20% (Ames & Molinari 1994), up to 33% in older outpatients (Molinari & Marmion 1993) and 61.5% in older inpatients (>Molinari & Marmion 1995). Analyses of data from the North American National Epidemiological Survey on Alcohol and Related Conditions, which studied over 43,000 individuals (Balsis et al 2007), found that older people were more likely to receive diagnoses of obsessive-compulsive and schizoid personality disorders and less likely to receive diagnoses of avoidant, dependent, antisocial, borderline and histrionic personality disorders. These authors were critical of the DSM measurement criteria arguing that it favours younger people. Personality disorders affect similar numbers of older and younger adults, with a higher prevalence of clusters A (odd and eccentric) and/or C (fearful or anxious) for older people (Kenan et al 2000).
CLINICAL FEATURES
The DSM–IV (American Psychiatric Association 2000) classifies 10 personality disorders into three clusters. The usefulness of the DSM–IV nosology for personality disorders in older people is currently being questioned (Balsis et al 2007, van Alphen 2006). It has been suggested that some of the specific DSM–IV criteria such as recklessness, impulsivity and functioning in the workplace are not appropriate for older people, and there is a proposal to develop more specific profiles. However, until firm recommendations are made, it is suggested that mental health workers who work with older people use the DSM–IV criteria albeit cautiously with this age group.
Cluster A personality disorders
Impact on the older person and their mental healthcare provision
The types of behaviour and thought patterns that characterise an older person with a paranoid personality disorder are (American Psychiatric Association 2000, Segal et al 2006):
The older person with a schizotypal personality disorder is easily recognisable as being bizarre or eccentric in their behaviour and dress. These people find any type of social or interpersonal relationship very uncomfortable to the extent where they may experience severe social anxiety. Cognitive or perceptual distortions, including ideas of reference, odd beliefs, magical thinking, suspicious or paranoid ideation, are common. They are reclusive and unfriendly, making relationship development very challenging. A tendency for neglect of personal care and their home environment ensures unpopularity with neighbours and visitors. Older people with this type of personality disorder also have difficulties when poor health necessitates admission to an RACF where they have to endure close contact with staff and other residents. Conversely, their odd behaviour may engender social rejection. Hearing and vision impairments can exacerbate paranoia (American Psychiatric Association 2000, Segal et al 2006).
The essential characteristics of schizoid personality disorder are a pervasive pattern of detachment from social relationships and a restricted range of emotions. These people are seen as being aloof, cold and detached, with no desire for close relationships. They engage in solitary activities, have little or no interest in sexual experiences, derive very little pleasure from activities and are indifferent to praise or criticism. Not having any close friends also comes under the criteria for schizoid personality disorder. However, this may not be considered as a maladaptive personality trait for older people who have outlived all their friends. The same could be said for ‘little or no interest in sexual experiences’ where this could be related to physiological and social changes (Balsis et al 2007). Additionally, hearing, vision and mobility impairments could hinder the development and maintenance of relationships. The older person with this type of personality disorder will usually resist offers of help, particularly if it involves contact with other people. They can become distressed if their independence is threatened and find it very difficult fitting into communal living situations (American Psychiatric Association 2000, Segal et al 2006).
Cluster B personality disorders
Impact on the older person and their mental healthcare provision
The older person with an antisocial personality disorder has a pervasive pattern of violating the rights of others. They unashamedly lie, steal, con and will even physically assault other people. Impulsivity with reckless disregard for the safety of self or others and engagement in illegal activities that end with imprisonment are other features of this disorder. A person with antisocial personality disorder can present as ingratiating and charming, but relationships tend to be shallow and exploitative. As these people age, physical decline will moderate some of the more aggressive and risk-taking behaviours. If they seek treatment, it is important to explore what their motivation is to ensure it is not exploitative, and interventions will focus on helping them to think through the consequences of their behaviour and to plan constructive behaviours (American Psychiatric Association 2000, Segal et al 2006).
Older women with histrionic personality disorder who are living among predominantly other women in an RACF that has mostly female staff may not display the flirtatious and sexualised behaviour. A tendency for suggestibility and being easily influenced by other people could be very problematic, particularly if cognitive impairment is present, as it could leave the older person open to abuse (American Psychiatric Association 2000, Segal et al 2006).
It has been suggested that borderline personality disorder diminishes as people age, whereas other theories suggest that it is a mortality effect, burnout and age-related changes in neurobiological substrates that impact on these behaviours or that the criterion for diagnosis does not fit older people (Devanand et al 2000). Either way, if pathological symptoms exist, they can be targeted for treatment. A central feature of borderline personality disorder is frantic efforts to avoid real or imagined abandonment. For an older person, this behaviour may translate into unjustified fears that their caregiver will abandon them or in the situation where an older person has great difficulty coming to terms with no longer being a lifelong caregiver when their children have left home. People with borderline personality disorder have a very unstable self-image or sense of self, and long patterns of unstable interpersonal relationships. Relationship interaction fluctuates from frantically seeking attention and support, to hostility and avoidance, to seeking forgiveness and support again. This pattern wears other people down; therefore, social support wanes. A commonly used defence mechanism is splitting, where everything and everyone is either ‘good’ or ‘bad’ and then this assessment abruptly changes for no sound reason. Such behaviours create a great deal of havoc, particularly in situations where there are a lot of people involved, such as in an RACF.
When young, these people are extremely impulsive and engage in self-damaging behaviours around sexual activity, spending, substance abuse and binge eating. However, with older age, these self-damaging behaviours may become less overt and intense, and may be replaced by acts of self-prescribing polypharmacy and refusing or sabotaging medical care. These people have chronic feelings of emptiness and have difficulty regulating and controlling their emotions such as anger. Suicidal behaviours, threats and self-mutilation are also prominent. They may also experience transient, stress-related paranoid ideation (American Psychiatric Association 2000, Segal et al 2006).
The older person with a narcissistic personality disorder typically has a grandiose sense of self-importance and entitlement, and is arrogant. They have fantasies of success, power, intelligence, beauty and ideal love. They believe they are special, should be admired by others and only associate with other special or high-status people. Lack of empathy is particularly noticeable and rage is often the response to negative feedback. To the narcissistic person, most people are considered unimportant and unworthy, so manipulating or taking advantage of them is seen as reasonable behaviour. This behaviour soon deters other people and the narcissistic person often ends up lonely and bitter. Ageing brings physical changes, loss of power, prestige, praise and independence, making this time of life exceptionally hard for these people to negotiate (American Psychiatric Association 2000, Segal et al 2006).


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


