FIGURE 7.1
7.2 Strengths of the Risk Prediction Paradigm
The Risk Prediction Paradigm is based on the proposition that the costs and risks of pharmacological therapy are justified only in those who are likely in the immediate future to suffer a clinical event, a proposition that on the face of it seems inarguable. After all, it is clinical events that injure us and therefore it is clinical events we should want to prevent. In this approach, the impact of a limited number of factors – typically, total cholesterol, HDL-C, blood pressure (BP), treatment for elevated BP, smoking and diabetes – are integrated into a multiple regression algorithm that calculates the likelihood of a cardiovascular event over the next decade. Causes are transformed into calculated risk and decisions are based on calculated risk, not causes.
Moreover, based on the Heart Protection Study252 and the meta-analyses of the CTT,230it has been widely accepted that the benefit of LDL lowering by statins is based on the level of risk, not on the level of LDL: the higher the risk, the greater the benefit; the lower the risk, the lower the benefit. In this scheme, the level of LDL is not relevant. Risk is all that matters. Furthermore, the AHA/ACC guidelines250 have stated that the statin clinical trials were tests of regimens, not of targets, and therefore therapy should not be adjusted to achieve any particular level of any particular marker of LDL.
The primary strengths of the Risk Prediction Paradigm are: first, that it works in that the frequency of events over a decade in a group of individuals can be forecast with reasonable accuracy and, second, that it is so broadly accepted by clinical scientists that it has also been broadly accepted by societal decision-makers. Prevention based on risk appears to be a quantitative, inclusive, rational, judicious approach and so, it has become the dominant paradigm to prevent cardiovascular events, appropriately balancing the costs of the adverse clinical events as well as the costs of the therapies against the benefits. Nevertheless, however broadly and deeply accepted, we believe there are major limitations in this approach, which we will set out below.
7.3 Weaknesses of the Risk Prevention Paradigm
7.3.1 The Limitation of Basing the Decision to Treat on the Likelihood of a Clinical Event over the Next Decade
The phrase – Primary Prevention – suggests we are starting with a blank slate: an artery that is normal, pristine, inviolate and that appropriate therapy will prevent the initiation and maturation of atherosclerotic lesions, which invade and destroy the walls of a normal artery, converting it from a soft supple tube to a hard rigid one that may suddenly, without warning, severely narrow or occlude. Unfortunately, in the real world, such a hope of beginning therapy before disease is well seated within the arteries is too often false because advanced intramural atherosclerotic disease is a necessary prerequisite for clinical events. Simply put: a high calculated risk over the next decade reflects a high probability that significant intramural atherosclerotic disease is already present in a substantial number of individuals. Otherwise risk for the group could not be high. This tight and necessary connection between established disease and clinical risk seems so obvious that it should not need saying but a risk-based strategy that initiates prevention only after risk is elevated has ignored this reality.
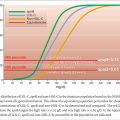
We know that it takes time for advanced intramural disease to develop – almost always decades and decades, extremely rare disorders with extreme elevations of LDL such as homozygous familial hypercholesterolemia being the rare exceptions. Moreover, even though the natural history of atherosclerosis stretches out over decades, there is evidence that it progresses at different rates at different times. Thus, anatomic disease, at least in men, increases rapidly between 30 and 49, but appears to peak in terms of progression between 50 and 59, advancing steadily but less dramatically after that.253For much of this time, dilatation of the artery prevents encroachment of the lesions on the lumen and only after serious injury to the arterial wall has occurred do acute reductions in the lumen of an artery occur. Because significant disease takes so long to develop, cardiovascular events only become common, at least as expressed as a percent of the population, when men are 60 or more and women are 70 or more. Therefore, the risk of a clinical event over the next decade cannot be high until men and women have reached these ages at which point, based on age alone, most will be at high risk.
Not surprisingly, therefore, in the United States, based on the new AHA/ACC Guidelines, 90% of men and 50% of women over 60 will be at ‘high risk’ and eligible for therapy.254 Indeed, a white male with no risk factors for CVD – that is a male who is a non-smoker, non-diabetic with a normal blood pressure and a normal non-HDL-C – will exceed the calculated 7.5% 10-year risk of a cardiovascular event at age 63 as will be the case for a 66-year-old African American man, a 70-year-old African American woman or a 71-year-old white woman. Age alone will take them over the treatment threshold. Age has this commanding power because the rate of events is relatively low before these ages but increases exponentially thereafter.
By the same token, age eliminates most of those who are under 60 as candidates for prevention, whether or not one of the cardinal causes of vascular disease – elevated LDL or blood pressure – is present. Consider a man with an LDL-C of 4.42 mmol/l (170 mg/dl), a level that is equivalent to the 94th percentile of the American population. At age 40, his 10-year risk is 2%, at age 50, 5%.223 Only at age 60 would his calculated 10-year risk exceed the threshold at which prevention with statins would be definitely re commended.
But this delay may cost him dearly since sudden death or substantial and irreversible injury to his left ventricle may be the first clinical manifestations of cardiovascular disease. Early cardiovascular events are the most costly in personal and societal terms because the victim is cut down within the most productive phase of their life and those who depend on him or her and the society that profits from his or her contributions are also profound losers. Unfortunately also, such tragic events are by no means as rare as most believe. Yet because, at the moment, prevention is based on calculated risk, the majority of early victims would not have been eligible for therapy simply because they were too young.
However, an equally, if not even more important, argument against the Risk Prediction Paradigm – because it involves a so much larger number of people – is that the ultimate total benefit of prevention by LDL lowering will be diminished if preventive therapy is initiated only after advanced intramural atherosclerotic lesions have developed. The risk of a clinical event in the 40-year-old man with the markedly elevated LDL-C might well be only 2% over the next decade and only 5% over the decade to follow. But during all of these 20 years, his arterial tree is under continuous assault from the LDL particles, which will enter and be trapped within the wall and which will drive the development and maturation of complex advanced intramural disease. The disease, which develops during this time, is the reason that his risk rises at age 60. Delaying LDL-lowering therapy has allowed this to occur unchallenged.
The cost in terms of events that might have been avoided may be considerable since clinical events may result from statins from multiple pathophysiological mechanisms, only some of which are inhibited or interfered with by statins. Thus the endothelium can be eroded and platelets adhere and clump to the denuded surface.255 This can produce a platelet-rich thrombus, which then detaches and embolizes downstream occluding a smaller vessel infarcting the muscle it supplies. A sequence such as this is a particularly common cause of sudden death and statins are unlikely to reduce the likelihood of this unhappy event. Alternatively, the fibrous cap can rupture, tearing the endothelium above it, exposing the thrombogenic lipid core directly to the blood, producing an acute occlusive thrombosis at the site. The likelihood of cap rupture is determined by multiple independent factors that affect its integrity: deposition of cholesterol in the core, the collagen production by smooth muscle cells, the activity of metalloproteinases from inflammatory cells, which can hydrolyze the collagen, systolic blood pressure and sympathetic stimulation of the heart, which alter mechanical stress and strain on the artery.256,257 Hemorrhage in the subadventitial space from the neovascularization that has developed in response to the injury within the arterial wall is yet another possibility.258 The hemorrhage can swell the thickness of the wall and reduce or occlude the lumen of the vessel.
Thus, there are multiple mechanisms of clinical events, each of which has a specific pathophysiology and therefore a specific set of inciting factors, and what finally happens depends on many intermediate steps. Statins are a potent therapy to reduce clinical events. But they are an imperfect therapy. Only a portion of the events recorded in the clinical trials are ever avoided, presumably because statins are effective against only some of the mechanisms that produce events. Thus, statins are likely to reduce the risk of plaque rupture because the deposition of cholesterol is reduced and the fibrous cap may consequently be strengthened but they are less likely to affect spontaneous intramural hemorrhage or endothelial denudation.
The bottom line is that once extensive intramural atherosclerotic disease is present, statins or any other form of LDL lowering will only be partially successful. This argues strongly that prevention should begin when we identify the causes of intravascular disease not when risk is high because disease will already be far advanced at this point. This is too often the fatal flaw in the Risk Prediction Paradigm.
Related posts:
 ApoB Lipoprotein Particles: the preferred Treatment Target in Primary and Secondary Prevention
ApoB Lipoprotein Particles: the preferred Treatment Target in Primary and Secondary Prevention
 Secondary ApoB Dyslipoproteinemias
Secondary ApoB Dyslipoproteinemias
 ApoB in Cardiovascular Risk Prediction
ApoB in Cardiovascular Risk Prediction
 Diagnosis of the ApoB Dyslipoproteinemias: The ApoB Algorithm
Diagnosis of the ApoB Dyslipoproteinemias: The ApoB Algorithm
 The Primary ApoB Dyslipoproteinemias
The Primary ApoB Dyslipoproteinemias
 The Life History of ApoB Lipoprotein Particles
The Life History of ApoB Lipoprotein Particles
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


