The Beginnings: Past and Present
J. Robert Dille
Stanley R. Mohler
Thus do men serve history and history the ages.
—Eddie Rickenbacker
History started today, not only yesterday.
—Anon.
EARLIEST CONCEPTUALIZATIONS
As prehistoric people made grueling trips across trackless lands, they surely must have envied the swift, graceful, and seemingly effortless flight of birds. Fantasies and legends involving wings and flight by gods, angels, rulers, and guardians occur in the folklore of nearly every culture. Windmills, kites, parachutes, and the rocket (the latter from China where gunpowder was invented about 900 AD) were early inventions bearing upon the pursuit of human flight.
The legend of father and son, Daedalus and Icarus, states that they made wings of feathers held together by wax to escape from King Minos’ Crete. During escape, Icarus ignored Daedalus’ admonishments, and flew too near the sun: the wax melted and he fell into the sea.
Roger Bacon, a 13th century Franciscan monk, was quoted as hearing about artificial wings that turned about a sitting person and beat the air “after the manner of a flying bird.”
Leonardo da Vinci designed a parachute in 1500. He also drew pictures of hypothetical human-powered helicopter and ornithopter flying machines. Leonardo died in 1519 AD, and his approximately 500 pages of notes and 1,500 sketches were forgotten for more than 300 years.
If available earlier, these writings could possibly have accelerated the course of aeronautical development.
Many legends, figures, and fantasies attest to our early predecessors’ fascination with the possibilities of human flight, an achievement that awaited the coalescence of intuition, technologic advances, and goal-driven experimentation. Of course, human tolerances to higher altitudes and in-flight acceleration forces awaited actual flight experiences before awareness of these aspects arose. In addition, the need for occupant restraint systems, crashworthiness protection, and a means to deal with in-flight spatial disorientation under conditions of loss of outside visual reference, also awaited flight experience.
The general sequence of topics in this chapter proceeds from the earliest conceptualizations by century, flowing through the 16th century. This latter European “Age of Reason” launched the 17th century “Age of Enlightenment.” Topics to be covered include the aeromedical implications of the first “mountain sickness” reports along with early laboratory gas studies and the hypoxic experiences of balloonists. The December 17, 1903 first flight of a heavier-than-air powered aircraft piloted by the Wright Brothers launched the basis for an explosive growth of aviation and the need for medical support of aviators. The April 12, 1961 earth-orbiting flight of Yuri Gagarin, of the Union of Soviet Socialist Republics (USSR), opened the era of human space flight.
The chapter concludes citing the development of space medicine, bringing us to the July 20, 1969 Apollo 11 moon landing by the National Aeronautics and Space Administration (NASA). The moon landing was conducted by Neil Armstrong and Edwin Aldrin Jr., the first two humans to walk on a heavenly body other than the earth, while Michael Collins, their orbiting Command Module Pilot circled overhead.
SIXTEENTH CENTURY EXPERIENCES
Discomfort with mountain travel was documented after the Spanish army under Cortez attacked Mexico in 1519. In addition, the Spanish army under Pizarro experienced mountain sickness 25 years later while conquering areas subsequently known as Ecuador, Chile, and Peru.
Later in the century, Jesuit Father Jose de Acosta blamed the air of lofty places. On five crossings over the Andes, he noted a loss of appetite, the presence of nausea and abdominal pain, in addition to vomiting of food, phlegm, bile, and blood. Father Acosta had profound weakness and had to be supported on his horse; he also had dizziness and was panting. Upon return to lower altitude, the symptoms shortly disappeared.
Acosta wrote “Not only men feel this, animals do too, and sometimes stop so that no spur can make them advance.” Acosta was “convinced that the element of the air is in this place so thin and so delicate that it is not proportioned to human breathing which requires it denser and more temperate.”
Acosta’s account was published in Seville in 1590 but is best found in the Hitchcock (1) translation of Bert’s Barometric Pressure. The book, originally published in French in 1878, contains 264 references on mountain sickness. Scientific studies on the effects, prevention, and treatment of acute and chronic mountain (altitude) sickness, pulmonary edema, and cerebral edema have been conducted in the Andes, on Mt. McKinley, and in the Himalayas. Scientists who conducted this research included McFarland, Hurtado, Hultgren, and Krakauer.
SEVENTEENTH AND EIGHTEENTH CENTURY PROGRESS
Evangelista Torricelli (1608-1647), an Italian physicist, invented the mercury barometer 50 years after Acosta’s observations. He studied the response of small animals to vacuum. Otto von Guericke (1602-1686), engineer, of Germany, invented the pneumatic pump in 1672. He studied how candle flames were extinguished, animals could not live, and sounds would not travel under vacuum. He also showed that horses could not pull apart two vacuumcontaining hemispheres. Robert Boyle (1627-1691), Irish natural philosopher, observed bubbles in the eye of a viper following its decompression in a vacuum environment. He discovered that at a constant temperature the volume of gas varies inversely with pressure—the famous “Boyle’s Law.”
Joseph Priestly (1733-1804), English scientist, and Antoine Lavoisier (1743-1794), French chemist, are separately credited with discovering oxygen.
During 1783, brothers Joseph and Etienne Montgolfier of France successfully launched hot air balloons, using burning damp straw, wool, and occasionally old shoes and even old meat in the mix. A rooster, a duck, and a sheep were hefted by hot air on September 19 of that year. On October 15, the brothers lifted Pilatre de Rozier, an apothecary of Metz, in a tethered hot air balloon to a height of 50 ft. On November 23, de Rozier and Francois Laurent Marquis d’Arlandes were free floated across Paris in a hot air balloon. American ambassador to France, Benjamin Franklin, observed that these developments in ballooning foretold a promising future.
Professor Jacques Alexandre Cesar Charles (1746-1823), along with Joseph Louis Gay-Lussac (1778-1850), articulated what is now known as Charles’ Law that states “At a constant pressure, a given amount of gas will expand its volume in direct proportion to the absolute temperature.” Charles invented the hydrogen balloon in 1783 and made a flight on December 1 with a companion (the balloon’s maker). After the companion left the balloon after a 1-hour 45-minute flight, the lightened balloon immediately rose to an altitude of 3,048 m (10,000 ft). Charles reported right ear and maxillary pain with increasing altitude, and this report is usually considered the first case of aerotitis. Early in the next century, Gay-Lussac made a balloon flight, on September 16, 1804, to an altitude of over 7,016 m (23,000 ft), a record that stood for approximately a half century.
Trained in Scotland and loyal to King George III, Boston physician John Jeffries moved to London at the beginning of the Revolutionary War. He, along with crowds estimated at 150,000 to 250,000, gathered to observe balloon ascents by John Pierre Blanchard and the Italian, Vincent Lunardi. Jeffries paid Blanchard 100 guineas to fly from London to Kent in a hydrogen balloon. On the flight, Jeffries carried a thermometer, barometer, pocket electrometer, hydrometer, precision timepiece, compass, small telescope, and seven sealed vials to collect air samples at different altitudes for Henry Cavendish, the discoverer of hydrogen. The results were reported to the Royal Society.
Blanchard had announced his intention to fly across the English Channel before agreeing to take Jeffries along. Again, Jeffries agreed to pay the expenses of the flight, and, if necessary to save Blanchard, he would jump into the channel.
Blanchard, in a bit of deviousness, ordered a vest lined with lead to keep the balloon from lifting, forcing Jeffries out. The tailor mistakenly sent the vest to Dr. Jeffries at a hotel in Dover, and the ruse was uncovered. On January 7, 1785, the two were the first to cross the English Channel, and Jeffries became the first paying aerial passenger on an international flight.
They carried the first over-water survival gear, cork vests, and equipment required during the over-water flight. Jeffries reported visual illusions: “we were fixed and objects appeared to pass to or from us or revolve around us.” He also reported that “we were enveloped by a certain stillness that could be felt” (possibly sensory deprivation). At one point it was almost necessary for Jeffries to jump into the water. Later, close to a hard landing, most of their clothing, the celebration bottle of brandy, the life vests, and all equipment except the barometer, were jettisoned.
To soften the landing in France, Jeffries thought to eliminate “five to six pounds of urine.” A letter from Benjamin Franklin’s son in London, to his son who was with his grandfather in Paris was delivered, the first airmailed letter.
Jeffries’ accounts have been reprinted in Aviation, Space, and Environmental Medicine (2,3).
Jeffries’ accounts have been reprinted in Aviation, Space, and Environmental Medicine (2,3).
In 1789, Dr. Jeffries returned to Boston and practiced medicine until his death in 1819. He was active in teaching, and gave the first public lecture on anatomy. He was a founder of the Boston Medical Library.
Jeffries helped Blanchard to make the first hydrogen balloon free flight in America on January 9, 1793. This event occurred in Philadelphia with the departure from the yard of the Walnut Street prison. A large crowd observed the departing flight, including President George Washington and the French Ambassador. Washington gave Blanchard a letter of introduction (Blanchard’s English was not very good, hence the letter for those he may meet on landing—some consider this the first U.S. passport). Blanchard’s pulse rate data collected for Dr. Benjamin Rush was 84 beats/minute on the ground and 92 at 1,772 m (5,812 ft). Six air samples were collected for Dr. Casper Wistar.
The balloon landed in Gloucester County, New Jersey. Blanchard returned to Europe and made a number of flights in various countries. While flying over The Hague, Netherlands, he is reported to have had an in-flight heart attack, falling more than 50 ft. He died on March 7, 1809, the first pilot in command to have an in-flight incapacitating cardiac event.
On June 15, 1785, Pilatre de Rozier, the first person lifted by the Montgolfiers, accompanied by a companion, Pierre Romain, attempted to cross the channel from France to Britain in a combination hydrogen-hot air balloon. The hydrogen caught fire half an hour after take-off and both died in the accident, the first aeronautic fatalities. De Rozier’s fiancée, Susan Dyer, witnessed the explosion, collapsed, and died.
THE NINETEENTH CENTURY
A Belgian physicist, Etienne Robertson, ascended to approximately 7,000 m (22,966 ft) with a music teacher named Lhoest, at Hamburg, Germany, on July 18, 1803. He described a hurried pulse, mental and physical apathy, and an indifference instead of his usual glory and passion for discoveries. He reported that his lips had swelled from blood rushing there and his hat seemed too small. He was able to place his hand in boiling water without feeling pain. He flew with Russia’s first aeronaut, Sacharoff, on June 30, 1804.
Robertson’s son, Eugene, ascended to 6,000 m (21,000 ft) at Castle Garden, New York, on October 16, 1826.
Dr. Claude Bernard (1813-1878) of France is considered the founder of experimental medicine. He studied the effects of illness, carbon dioxide, cold, and superoxygenated air on hypoxia tolerance. He studied carbon monoxide combination with hemoglobin as a cause of oxygen starvation. While studying the liver, he discovered that liver glycogen (he gave the substance its name) broke down to glucose, elucidating the glucose-glycogen relationship.
Paul Bert (1833-1886), considered by some to be the father of aviation medicine, was born in Auxerre, Yonne, France. He was trained in engineering, law, physiology, and medicine. He succeeded his mentor, Claude Bernard, to the chair of physiology, Faculte’ des Sciences, Paris. He conducted extensive work in the early 1870s, the latter culminating in his classic book, La Pression Barométrique, Recherches de Physiologie Expérimentale in 1878. Mary Alice and Fred Hitchcock translated the volume into English during World War II.
Bert undertook studies to explain the symptoms reported by aeronauts during their balloon ascensions. He conducted 670 experiments in bell jars and an altitude chamber of his construction. He used plants, sparrows, rabbits, guinea pigs, cats, dogs, and humans, and reported the findings in his book. He established that death occurred at a partial pressure of oxygen of 35 mm Hg, irrespective of atmospheric pressure. He found that the intermittent inhalation of air rich in oxygen relieved symptoms of hypoxia. He also recognized that excess carbonic acid in the blood and tissues created adverse effects. The hazard of loss of too much carbon dioxide through hyperventilation was apparently not recognized. Bert died as Resident General, Tonkin province, French Indochina, at age 53, on November 11, 1886, during an attack of dysentery.
James Glaisher (1809-1903) and his balloon engineer, Henry Coxwell (1819-1900), made several ascents to high altitudes over England to relatively high altitudes without supplemental oxygen. On September 5, 1862, reaching 8,839 m (29,000 ft), Glaisher was unconscious for an estimated 7 minutes. It is reported that the two balloonists experienced some acclimatization to high altitudes without turning blue or having difficulty breathing.
Henri Sivel, a naval officer, and Joseph Croce-Spinelli, a journalist, ascended on March 22, 1874, in the balloon, Polar Star, to a height of 7,300 m (23, 950 ft). They carried bags provided by Bert containing 40% and 70% oxygen, the former to be breathed on reachi ng 3,600 m (11,811 ft) and the latter on reaching 6,000 m (19,685 ft). It was observed that the oxygen improved strength, alertness, memory, visual acuity, and appetite.
On April 15, 1875, they, along with a third aeronaut, Gaston Tissandier, launched in the balloon, Zenith, with goldbeater’s bags (made from the cecum of an ox) of 65% and 70% oxygen. They sought to reach an altitude well above 8,000 m (26,246 ft), exceeding Glaisher’s and Coxwell’s September 5, 1862 record. Bert sent a message that the French balloonists did not have sufficient oxygen, but they had lifted off before the arrival of the message. At 7,450 m (24, 442 ft) they cut three bags of ballast, probably in a state of hypoxic euphoria, and climbed to an estimated 8,600 m (28, 215 ft). All three lost consciousness and Sivel and Croce-Spinelli died in-flight. Tissandier passed out, coming to some time later as the balloon had spontaneously descended to a lower altitude and struck the ground.
In the third edition of his Principles and Practice of Aviation Medicine (4), Armstrong wrote, “the first use of air transportation in support of medical activities occurred during the Siege of Paris in 1870 when a total of 160 patients were removed from the city by means of an observation
balloon.” Lam has examined the records and found that no passengers were patients (5). The records contain the names of the balloonists, the weights of the mail, and the landing sites. The flights occurred between September 23, 1870 and January 21, 1871, during the Paris siege as the Franco-Prussian war continued. Tissandier was one of the balloonists but most were sailors.
balloon.” Lam has examined the records and found that no passengers were patients (5). The records contain the names of the balloonists, the weights of the mail, and the landing sites. The flights occurred between September 23, 1870 and January 21, 1871, during the Paris siege as the Franco-Prussian war continued. Tissandier was one of the balloonists but most were sailors.
TWENTIETH CENTURY: EXPONENTIAL GROWTH OF AEROSPACE MEDICINE
The invention of the practical heavier-than-air powered and controlled flight by Wilbur and Orville Wright of Dayton, Ohio, initially proved by them on December 17, 1903 at Kitty Hawk, North Carolina, was followed in the years before World War I by flight schools and derivative aircraft in all parts of the world. Large dirigibles also evolved, and the German Naval Airship Division conducted air raids over London, flying at 5,000 to 6,000 m (16,400-20,000 ft) whenever possible to avoid airplane attacks. Eight hours of cold, hypoxia, and engine noise caused documented dizziness, tinnitus, headache, increased heart and respiration rates, and fatigue. The supplied compressed oxygen had an unpleasant oily taste. Crewmembers and commanders were reluctant to use oxygen, despite symptoms, because to do so was considered as a sign of weakness. Liquid oxygen was later used because more could be carried, weight for weight, than as a gas (4).
On February 7, 1912, the U.S. War Department published instructions concerning the physical examination for candidates with respect to aviation duties. These instructions were preceded by the 1910 minimum medical standards for military pilots that were developed in Germany, the first country to establish such standards. Soon afterward, the Italian Air Medical Service followed suit. The French and British established military pilot medical standards in 1912. The U.S. military established detailed physical standards for aviators under the guidance of Theodore C. Lyster in 1916. These were published in 1919 as the Air Service Medical (6).
With respect to the early standards, the British emphasized cardiovascular performance and hypoxia tolerance with a rebreather bag that progressively decreased the oxygen to simulate the decrease in oxygen pressure at higher altitudes. The French added vestibular function and neurovascular steadiness in the presence of an unexpected gunshot. The Italians emphasized reaction time. When the United States acquired its first airplane in 1908, the general army duty medical standards applied. These emphasized the dental characteristics, a holdover from the Civil War era when enlisted men needed to be able to pull a cork by the teeth from a powder flask. The 1912 draft aviation medical standards emphasized normal vision, normal hearing and eardrums, and the visual ability to determine distances. Disqualification included colorblindness, acute or chronic disease of the middle or inner ear, or auditory nerve, or any disease of the respiratory, circulatory, or nervous system. Equilibrium was tested by standing with the eyes closed, and then hopping with the eyes open and then closed. In 1914 new arbitrary, more rigorous standards, were ordered by the Surgeon General, but failure rates were so high for new young applicant officers that the standards were relaxed. One screening test involved the candidate holding a needle between the thumb and forefinger. A blank pistolwas fired behind the candidate’s head. If the startle reaction produced blood, the candidate was disqualified.
During the first year of flying in World War I, when there was little combat, the English and French found that 2% of aircraft accidents were due to combat, 8% were due to mechanical problems, and 90% were due to human failure; two thirds of these 90% were reported to be due to physical defects (6).
The U.S. medical personnel thought that a considerable proportion of the physical defects leading to accidents “are the immediate or late effects of strain on the circulation under the influence of low oxygen tension in the air” (6). Some soldiers disqualified for further combat because of battle fatigue, shell shock, and neurocirculatory asthenia became pilots. The Royal Air Force (RAF) of the United Kingdom started a Care of Flyer Service. This activity reduced pilot deficiency accidents over 2 years from 60% to 12%. Improved physical standards, examinations, flight training, and attention to physical and emotional problems undoubtedly contributed to this decline.
Even so, many aces had physical defects that would be disqualifying by current standards. Roy Brown, who shot down top ace Baron Manfred von Richthofen (80 victories) in 1918, had chronic stomach distress, requiring the regular consumption of soda, milk, and brandy. American pilot Elliott Springs (5 victories) consumed milk of magnesia and gin, alternately, to relieve chronic stomach symptoms. “Eddie” Rickenbacker (26 victories) required a mastoidectomy during the war. French “ace of aces,” Georges Guynemer (53 victories) disappeared during a flight that was preceded by emotional strain and a crash-induced concussion and knee injury.
A little-known pilot with the name of Veil, when asked why he stayed with the Lafayette Flying Corps when the United States came into the war, stated that he would not qualify in the U.S. air arm because he had “a game leg, a stiff neck, a hole in my groin, and a blood disease among other things.”
Britain’s top ace, 34-year-old Mike Mannock (73 victories) was nearly blind in the left eye from a congenital condition. American William Thaw (5 victories), Lafayette Escadrille and later U.S. 103rd Aero Squadron, had normal vision in only one eye. Lt. Frank Alberry of Australia lost his right leg in ground combat in 1916. He was determined to fly as he could not be a ground troop with an artificial leg. He sought an audience with the King, and obtained a letter of acceptance. He took this to the Air Board, went through pilot training, and shot down seven enemy aircraft. In 1921, the New Australian Air Force would not accept him for flight service.
German ace Oswald Boelcke (40 victories), had severe asthmatic attacks and Georg Zeumer, skilled pilot and 1915 combat instructor of Baron von Richthofen, was a “lunger” with advanced tuberculosis, chronic coughing, and a very unhealthy appearance. Flying was considered a seated sedentary activity, a factor in the decisions to allow certain soldiers too impaired to be in the trenches to take to the air.
The U.S. Army had issued orders forbidding hard landings and the wearing of spurs in the cockpit. In May 1917, the Army established new medical standards for flight crew, including normal eye muscle balance, fusion, intraocular tension, visual field, near-vision accommodation, and the ability to clear the ears on descent. A turning chair test took the place of the stand, walk, and hop test. Specially trained physicians at 35 centers in the United States conducted the examinations.
Theodore C. Lyster, MD, Chief Surgeon of the U.S. Army Aviation Section, selected in May 1917 Isaac H. Jones, MD, a Philadelphia otologist, to open the first of the 35 medical examination centers at the University of Pennsylvania Hospital. In December, Dr. Lyster and Dr. Jones spent 3 months in Europe, assessing the medical problems facing aviators. On return, they established the Air Service Medical Research Laboratory at Hazelhurst Field, Mineola, Long Island, New York. William H. Wilmer, MD was put in charge. This new facility contained a low-pressure chamber, allowing the program to conduct pioneering studies in aviation physiology aspects and aircrew protection from hypoxia.
The above-mentioned principals established a medical research board on October 18, 1917 to investigate conditions that affect the efficiency of pilots, to carry out tests on pilot abilities to fly at high altitudes, to carry out tests on suitable equipment to supply oxygen to pilots, and to act as a standing medical board on matters relating to the physical fitness of pilots. Examination procedures and research at the laboratory are provided in Air Service Medical (6).
A program at the new laboratory instituted selection and training measures for new aeromedical examiners. Isaac Jones, MD, and fellow otologist, Eugene R. Lewis, MD, recommended that the examiners fly regularly. Lewis introduced the new term for these physicians, flight surgeons. Pilots and commanding officers were to be counseled with respect to an airman’s condition that warranted temporary or permanent “grounding.”
The first flight surgeon to report for active duty at a U.S. base was Capt. Robert J. Hunter. From Park Field, Tennessee, Dr. Hunter submitted a report dated May 13, 1918 to Dr. Lyster documenting early efforts to reduce accidents. The report stated that 63 candidates were interviewed, a sick call was held on May 27, a rest period was established between 11:00 AM and 3:00 PM, and athletic and recreation exercises were to be held twice/week. Sanitary cups in the field and shady areas for cadets were instituted. Three nonfatal accidents were investigated, one due to inexperience, one possibly due to hitting the head on the cowl during a loop, and one due to chasing a crow. Discussions with the mess officer were undertaken. Hunter acted as a member of a special board in several cases to consider whether further instruction of certain cadets should be continued.
Dr. Isaac Jones believed that the doctor who flies best understands the pilot. He taught that keeping pilots mentally and physically fit to continue flying was the main purpose of flight surgeons. He reportedly said that it might take 100 years to convince pilots not to feel that the main purpose of flight surgeons is to find a way to not let pilots fly. Jones and Lewis probably coauthored Air Service Medical and Jones also wrote Equilibrium and Vertigo, 1918. Raymond E. Longacre, MD, a 1921 graduate of the new flight surgeon school, developed for the first time a set of personality criteria for selecting candidates for flight training. Following World War I, Hazelhurst Field was converted to a private airport (Roosevelt Field), and the medical research facility was moved in 1919 to nearby Mitchel Field. In 1926 the facility again moved, this time to Brooks Field, San Antonio. Later it moved to Randolph Field and subsequently back to Brooks.
In 1924, the National Geographic Magazine stated, “Perhaps the most heroic test of an aviator’s grit and stamina is an altitude climb” (7). Rudolph W. “Shorty” Schroeder of McCook Field, Dayton, Ohio, began to set altitude records in 1918, reaching 10,093 m (33,114 ft) on February 27, 1920, his third record. He used a LePere LUSAC-11 (LePere U.S. Army Combat) open cockpit American-produced two-seat biplane that resembled the British Bristol fighter. It had a GE Moss supercharger powered by exhaust gases to boost air to its 400 hp Liberty engine. Schroeder’s oxygen gave out at the peak altitude and he lost consciousness. He recovered at 914.4 m (3,000 ft) after losing 9,144 m (30,000 ft) in 2 minutes and landed at the edge of the river near McCook Field. There were other problems, including ice in the oxygen tubes and carbon monoxide. The flight was a major demonstration of capabilities and deficiencies in pursuing high-altitude flights.
John A. Macready followed the Schroeder flights in the same aircraft and reached 11,521 m (37,800 ft) on September 28, 1921. He wore suits of woolen underwear, his regulation uniform, a knitted wool garment, a leather suit padded with down and feathers, fur-lined gloves, fleece-lined moccasins over the boots, and goggles treated with an antifreeze gelatin (Figure 1-1). An oxygen tube was attached to a pipe-stem mouthpiece. A mask protected the face from freezing at the −67°F range of air temperature.
Macready and Oakley Kelly made the first nonstop transcontinental airplane flight in a Fokker T-2 monoplane across the United States, departing Roosevelt Field, Long Island, New York, at 12:36 PM (EST) on May 2, 1923, and landing at Rockwell Field, San Diego, California, at 3:26 PM (EST) on May 3, a flight of 26 hours and 50 minutes covering 2,516 mi. The pilots had made two prior “endurance” cross-country flights in the Fokker to test their physical capabilities on such long flights as well as the aircraft and its equipment. The pilot in the open cockpit just behind the engine could check the maps en route while the other pilot in the fuselage with side windows kept the wings level with a set of controls, a “human autopilot.” Kelly made
the take-off from Roosevelt Field and Macready made the landing at Rockwell Field. The pilot seat back was modified so that the two could change places periodically during the long flight.
the take-off from Roosevelt Field and Macready made the landing at Rockwell Field. The pilot seat back was modified so that the two could change places periodically during the long flight.
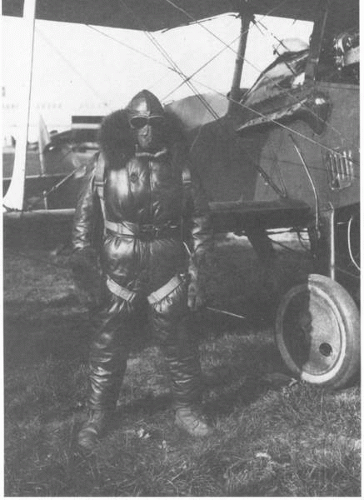 FIGURE 1-1 Lt. John A. Macready, U.S. Army Engineering Division test pilot, McCook Field, Ohio, dressed for his record ascent to 11,521 m (37,800 ft) on September 28, 1921. |
Macready made the first night parachute jump when engine failure occurred at 518 m (1,700 ft) on June 18, 1924. He landed unhurt. He also set National Aeronautic Association altitude and duration records in a bomber in 1924, and reached 11,796 m (38,700 ft) in an XCO5 aircraft with a turbosupercharger on January 29, 1926. Some scientists in 1923 reportedly told Macready that he might cross a boundary beyond the pull of gravity and become a space satellite.
Lt. Harold R. Harris, Flying Section Chief, Engineering Division, McCook Field, set ten Federation Aeronautique Internationale (FAI) World Air Records and 16 American air records during October 1, 1920 and January 30, 1925. During June 1921, Harris flew the first pressurized aircraft, an experimental D-99-A single-engine biplane. Owing to the circumstance that the pressurization system capability greatly exceeded the outflow valve capability, with no pilot control of cabin pressure, the aircraft cabin became pressurized to 914 m (3,000 ft) below sea level as the aircraft climbed out. The cabin air became hot and Harris was fortunate to get the airplane unharmed on the ground. Much was learned from this experience.
On October 20, 1922, Harris was the first pilot to save his life by parachuting from a Loening PW-2A that broke up in the air (Figure 1-2). He was made member number one of the subsequently famous “caterpillar club,” established by the Irvin Parachute Company.
Charles Lindbergh joined the Army as an aviator in training (note: he was already a low-time civilian pilot), Brooks Field, Texas. During training while diving on a target aircraft, another pilot ran into Lindbergh’s craft, the two airplanes becoming locked with one another. Both pilots were in the first class to be issued parachutes, and both parachuted to safety. Lindbergh graduated in March 1925, at the top of his class. Army aviation was underfunded, so he left and joined the Missouri National Guard.
Lt. Albert Stevens, a skilled aerial photographer, often flying with Macready, parachuted from a Martin MB2 bomber from an altitude of 7,376 m (24,000 ft) to set a world record over McCook field on June 12, 1922.
Capt. Hawthorne C. Gray set unofficial balloon altitude records in 1927. On March 9, 1927, he rose from Belleville, Illinois to an altitude of 8,230 m (27,000 ft) where he passed out due to faulty oxygen equipment and overexertion from emptying ballast bags. Fortunately, the balloon descended and he lived to try again. On May 4, 1927, he lifted off with a new oxygen system and a cord to dump ballast, reaching 12,945 m (42,470 ft). On descent, the balloon began falling at an excessive rate, so he bailed out at 383 m (8,000 ft). Therefore, he did not qualify for an official FAI record, but he was alive. He reported that during the flight he experienced a feeling of detachment, severe chest pains on exertion, and a strong desire to take a nap. On November 4, 1927, Gray went aloft again, reaching 12,192 m (40,000 ft). Unfortunately, his clock froze, he exhausted his oxygen, lost consciousness, and died. On November 5, the gondola was found in a tree near Sparta, Tennessee. Scientists concluded that high-altitude balloon flights should be equipped with sealed cabins. Gen. James H. Doolittle stated during his speech on October 20, 1962, on the occasion of the dedication of the Federal Aviation Agency’s Civil Aeromedical Research Institute new research facilities, Oklahoma City, Oklahoma, that “The price for almost every advancement in aviation has been high. Progress was frequently bought with someone’s life.”
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


