Highlights
- •
Testosterone recovery after androgen deprivation therapy is highly variable.
- •
Younger age and GnRH antagonist use are associated with testosterone recovery.
- •
Many men prescribed GnRH agonists may never recover their testosterone.
- •
Strategies to limit treatment duration of androgen ablation should be considered.
Abstract
Purpose
Finite courses of androgen deprivation therapy (ADT) are often utilized in men undergoing treatment for prostate cancer. Previous evidence suggests that timing of testosterone (T) recovery can be variable after ADT. Recently, an oral gonadotropin releasing-hormone (GnRH) antagonist, relugolix, has demonstrated more rapid T recovery than injectable GnRH agonists such as leuprolide. In this study, we sought to evaluate patient characteristics associated with T recovery in patients undergoing ADT of defined duration.
Materials and Methods
The Northwestern Enterprise Data Warehouse was queried for men with prostate cancer who completed a course of ADT and subsequently had a testosterone lab performed. Testosterone recovery was evaluated for levels that reached above castrate (T > 50 ng/dl), partial recovery (T > 150 ng/dl), and full recovery (T ≥ 300 ng/dl).
Results
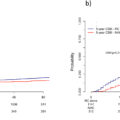
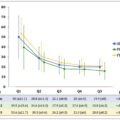
388 men who received finite courses of ADT were identified (348 receiving leuprolide, 36 receiving relugolix, and 4 receiving degarelix). In multivariable Cox regression analysis, men who were prescribed GnRH antagonists (HR = 3.74, CI = 2.53–5.53, P ≤ 0.001) and who were younger (HR for 1 year increase in age = 0.96, CI = 0.95–0.98, P < 0.001) were more likely to achieve partial recovery. In a subgroup analysis, men who received extended ADT courses (>12 months) with a GnRH agonist had lower rates of partial T recovery (HR = 0.58, CI = 0.41–0.81, P = 0.001).
Conclusion
T recovery after ADT is variable with roughly one sixth of men remaining castrate. GnRH antagonist use and younger age are associated with higher rates of T recovery after ADT. Longer ADT courses were associated with worse T recovery rates.
1
Introduction
Prostate cancer is a significant health burden for men across the world. It remains the most frequently diagnosed noncutaneous cancer for American men; in 2024 alone, the American Cancer Society estimates that 299,010 American men will receive a new diagnosis of prostate cancer [ ]. Current estimates suggest that up to 40% of men diagnosed with prostate cancer will eventually receive some form of androgen deprivation therapy (ADT) which can be associated with serious quality of life implications [ ].
The complications arising from ADT may range from low energy levels and decreased libido to having an increased risk of developing major adverse cardiovascular events and diabetes [ ]. While men with metastatic disease are often exposed to lifelong ADT, many men receive defined courses, typically alongside radiation therapy, for clinically localized or biochemically recurrent disease [ ]. For these men, patterns of testosterone (T) recovery vary and can be protracted, with some men remaining castrate for years after cessation of therapy, and some not recovering testosterone production at all [ ]. Relugolix is an oral gonadotropin releasing hormone (GnRH) antagonist that provides an alternative means of ADT to depot injections of GnRH agonists [ ]. Importantly, in the HERO trial, patients treated with relugolix experienced more rapid T recovery after cessation of therapy compared to their counterparts who received leuprolide [ ]. Real-world data describing T recovery during treatment with different forms of ADT has been limited.
In this study we sought to evaluate T recovery for patients prescribed a defined course of ADT at our multicentered academic institution.
2
Materials and Methods
2.1
Study Population
The Northwestern Enterprise Data Warehouse [ ] was queried for men with an established diagnosis of prostate cancer for whom ADT (leuprolide, relugolix, or degarelix) were prescribed from 2005 to 2023 and who had a recorded testosterone lab draw after completing ADT. Baseline demographics, clinicopathologic characteristics of disease, treatment history of prostate cancer, testosterone lab results, and Charlson comorbidity index (CCI) were collected.
2.2
Definitions
The primary outcome of interest was the patient’s highest recorded T after completion of ADT. T recovery was categorized in 1 of 4 ways: full recovery, maximum T level at least 300 ng/dl; partial recovery, maximum T level > 150 ng/ml, return to noncastrate levels, maximum T level > 50 ng/ml; and castrate, maximum T ≤ 50 ng/ml. 300 ng/dl was chosen as the cutoff for full recovery as current clinical guidelines state that T levels below 300 ng/dl should be considered hypogonadal [ ] 150 ng/dl was chosen as the cutoff for partial recovery as guidelines suggest this threshold as representing very low or exceedingly low testosterone [ ].
Studied GnRH agonists included leuprolide only as goserelin was not utilized in our medical system. GnRH antagonists included relugolix and degarelix. Duration of ADT therapy was utilized as a continuous and categorical variable. When evaluating the entire cohort, ADT duration was dichotomized as a categorical variable where short-term ADT was defined as usage ≤ 6 months of therapy and long-term ADT was defined as usage > 6 months of therapy. Very few men received longer than 12 months of GnRH antagonist therapy. Because of this, extended durations of ADT were studied in men receiving GnRH agonists only. In this sensitivity analysis, ADT duration was defined as short-term (≤ 6 months), medium-term (6–12 months), and extended-term (> 12 months). History of diabetes, obstructive sleep apnea, high BMI, HIV/AIDS, pituitary dysfunction, and osteoporosis were defined by ICD10 codes. These clinical variables were analyzed as they are associated with low T and thus may be correlated with T recovery [ ].
2.3
Statistical Analysis
Descriptive statistics and Cox proportional hazard regression models are described in the eMethods. Three subgroup analyses were performed which, briefly, consisted of patients with a recorded baseline T level, patients treated only with GnRH agonists, and patients who received ADT for less than 12 months. Additional details are provided in the eMethods. Statistical significance was defined as P ≤ 0.05. Statistical analyses were performed using R v4.2.2 statistical software [ ].
Results:
2.4
Patient Population
We identified 388 men who received finite courses of ADT (348 receiving leuprolide, 36 receiving relugolix, and 4 receiving degarelix; consort diagram shown in Fig. 3 ). Descriptive statistics are shown in Table 1 . The median age of our cohort was 74 (IQR = 67–78). Most men receiving a defined course of ADT had a history of prostate radiation (83.51%). The median time on ADT was 11.75 months (IQR = 6.00–23.63). The median follow-up time from discontinuation of ADT to last T evaluation was 443 days (IQR = 212–778).
| Overall Cohort | Recovery of Testosterone | |||
|---|---|---|---|---|
| Characteristic | n = 388 a | Achieved Partial or Full Recovery , n = 261 a | No Partial or Full Recovery , n = 127 a | P -value b |
| Baseline Characteristics | ||||
| Age | 74.00 (67.00, 78.25) | 72.00 (66.00, 77.00) | 76.00 (72.00, 81.00) | < 0.001 |
| Race | 0.7 | |||
| Asian | 5 (1.29%) | 2 (0.77%) | 3 (2.36%) | |
| Black | 45 (11.60%) | 33 (12.64%) | 12 (9.45%) | |
| White | 258 (66.49%) | 174 (66.67%) | 84 (66.14%) | |
| Other | 21 (5.41%) | 14 (5.36%) | 7 (5.51%) | |
| Patient declined to respond | 59 (15.21%) | 38 (14.56%) | 21 (16.54%) | |
| Insurance | < 0.001 | |||
| Medicaid | 7 (1.81%) | 2 (0.76%) | 5 (3.94%) | |
| Medicare | 279 (71.91%) | 175 (67.05%) | 104 (81.89%) | |
| Private | 102 (26.29%) | 84 (32.18%) | 18 (14.17%) | |
| BMI | 28.02 (25.15, 31.40) | 27.89 (25.10, 31.22) | 28.46 (25.61, 32.06) | 0.2 |
| Charlson Comorbidity Index | 6.00 (5.00, 8.00) | 6.00 (5.00, 8.00) | 7.00 (6.00, 9.00) | < 0.001 |
| History of Obstructive Sleep Apnea | 58 (14.95%) | 40 (15.33%) | 18 (14.17%) | 0.8 |
| History of Osteoporosis | 11 (2.84%) | 7 (2.68%) | 4 (3.15%) | 0.8 |
| History of Type 2 Diabetes | 65 (16.75%) | 35 (13.41%) | 30 (23.62%) | 0.011 |
| History of Pituitary Dysfunction | 2 (0.52%) | 2 (0.77%) | 0 (0.00%) | > 0.9 |
| History of HIV/AIDS | 2 (0.52%) | 2 (0.77%) | 0 (0.00%) | > 0.9 |
| Prostate Cancer Treatment | ||||
| Received Prostate Radiation | 324 (83.51%) | 229 (87.74%) | 95 (74.80%) | 0.001 |
| Received Radical Prostatectomy | 137 (35.31%) | 100 (38.31%) | 37 (29.13%) | 0.076 |
| Median ADT Duration (Months) | 11.75 (6.00, 23.63) | 8.20 (6.00, 20.90) | 18.00 (6.40, 24.45) | < 0.001 |
| Maximum Follow-Up | 443.00 (211.75, 777.50) | 467.00 (266.00, 782.00) | 312.00 (96.00, 753.50) | < 0.001 |
| ADT Type | 0.001 | |||
| Leuprolide | 348 (89.69%) | 225 (86.21%) | 123 (96.85%) | |
| Relugolix/Degarelix | 40 (10.31%) | 36 (13.79%) | 4 (3.15%) | |
| ADT Duration Dichotomized | 0.5 | |||
| Short-Term (≤ 6 months) | 101 (26.03%) | 71 (27.20%) | 30 (23.62%) | |
| Long-Term (> 6 months) | 287 (73.97%) | 190 (72.80%) | 97 (76.38%) | |
| Gleason Grade Group | 0.046 | |||
| 0 | 4 (1.63%) | 3 (1.80%) | 1 (1.28%) | |
| 1 | 18 (7.35%) | 15 (8.98%) | 3 (3.85%) | |
| 2 | 55 (22.45%) | 41 (24.55%) | 14 (17.95%) | |
| 3 | 77 (31.43%) | 57 (34.13%) | 20 (25.64%) | |
| 4 | 43 (17.55%) | 22 (13.17%) | 21 (26.92%) | |
| 5 | 48 (19.59%) | 29 (17.37%) | 19 (24.36%) | |
| Unknown | 143 | 94 | 49 | |
| Baseline T | 316.00 (228.50, 390.00) | 339.50 (255.25, 404.25) | 262.00 (142.25, 335.75) | 0.001 |
| Unknown | 250 | 165 | 85 | |
Related posts:
 A systematic review of family history, race/ethnicity, and genetic risk on prostate cancer detection and outcomes: Considerations in PSA-based screening
A systematic review of family history, race/ethnicity, and genetic risk on prostate cancer detection and outcomes: Considerations in PSA-based screening
 Neoadjuvant chemotherapy before radical cystectomy in patients with organ-confined and non-organ-confined urothelial carcinoma
Neoadjuvant chemotherapy before radical cystectomy in patients with organ-confined and non-organ-confined urothelial carcinoma
 Comparison of outcomes between single-port and multiport retroperitoneal robotic partial nephrectomy
Comparison of outcomes between single-port and multiport retroperitoneal robotic partial nephrectomy
 The learning curve for transperineal MRI/TRUS fusion prostate biopsy: A prospective evaluation of a stepwise approach
The learning curve for transperineal MRI/TRUS fusion prostate biopsy: A prospective evaluation of a stepwise approach
 Impact of heavy metals, oxidative stress, expression of VHL, and antioxidant genes in the pathogenesis of renal cell carcinoma
Impact of heavy metals, oxidative stress, expression of VHL, and antioxidant genes in the pathogenesis of renal cell carcinoma
 Testicular cancer malpractice trends
Testicular cancer malpractice trends
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


