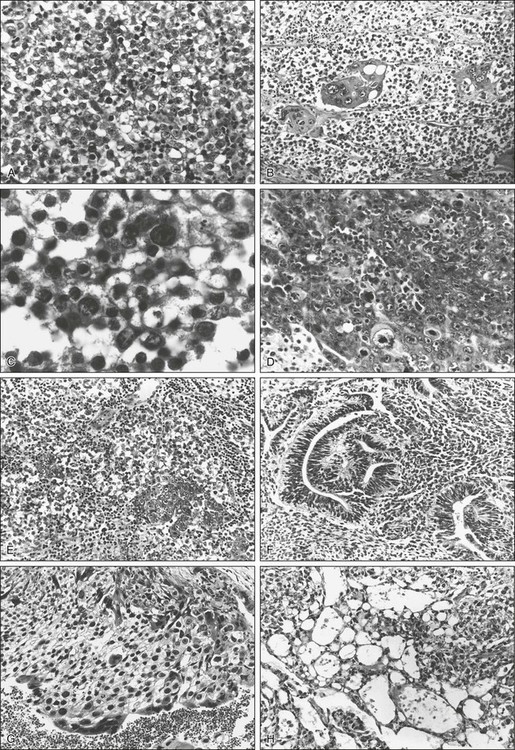
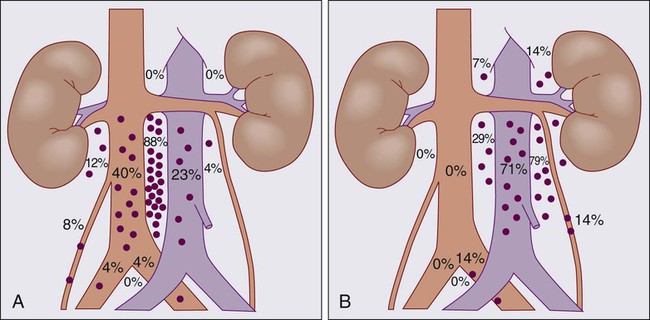
86 Terence W. Friedlander, Charles J. Ryan, Eric J. Small and Frank Torti • One percent of all male malignancies, accounting for 6000 to 8000 new cases a year in the United States • Most common malignancy among men aged 15 to 35 • Germ cell tumors: 95% of all testicular cancers • Pure seminoma: 40% of all germ cell tumors • Nonseminoma: 60% of all germ cell tumors, with embryonal elements most frequent • Testicular torsion, hydrocele, varicocele, spermatocele, epididymitis (can coexist with germ cell tumors) • Other malignancies: lymphoma, metastases from prostate cancer, lung cancer, or melanoma (generally in older age group) Diagnosis and Staging Evaluation • Complete history and physical examination • Bilateral testicular ultrasonography • Tumor serum markers (lactate dehydrogenase [LDH], β-human chorionic gonadotropin [β-hCG], and α-fetoprotein [AFP]) • Complete blood count, chemistry studies including renal function • Computed tomography (CT) of chest, abdomen, and pelvis • Additional imaging studies as appropriate (e.g., imaging of brain in patient with pure choriocarcinoma) • Radical (inguinal) orchiectomy (transscrotal biopsy or orchiectomy should be avoided) • Localized disease is curable with orchiectomy alone. Both adjuvant chemotherapy and adjuvant low-dose radiotherapy to lymph nodes can reduce the risk of relapse. • Locally advanced disease (stage IIA/IIB) is curable in more than 90% of patients with orchiectomy plus radiotherapy to involved nodal areas or with combination chemotherapy. • Metastatic disease (stage III) or bulky locally advanced disease (stage IIB/IIC) is curable in 90% with combination chemotherapy • Postchemotherapy retroperitoneal lymphadenectomy can prevent subsequent relapse in select patients • Clinically localized disease is curable with orchiectomy alone in 60% to 87% of patients • Risk of relapse is decreased with both retroperitoneal lymphadenectomy as well as with adjuvant combination chemotherapy, although in selected patients, surveillance without surgery is a possible option • Adjuvant combination chemotherapy after lymphadenectomy may further decrease risk of relapse, but does not impact survival • No bulky locally advanced (stage IIA) disease is cured with retroperitoneal lymphadenectomy alone in up to 65%. Adjuvant chemotherapy after surgery can reduce the risk of relapse for these patients. • Moderate to bulky nodal disease (stage IIB/C) requires combination chemotherapy • Metastatic disease (stage III), or bulky locally advanced disease is curable in 80% of patients with combination chemotherapy • Postchemotherapy retroperitoneal lymphadenectomy can prevent subsequent relapse in selected patients Effective Second- and Third-Line Therapies • Chemotherapy salvages about 80% of patients who have failed surgical or radiation therapeutic treatments • Second-line chemotherapy for patients who have failed prior chemotherapy curative in 20% of patients • Subsequent high-dose therapy with autologous bone marrow transplant (ABMT)/peripheral stem cell transplant (PSCT) possibly curative in 15% to 20% of those who have failed second-line therapy GCTs account for 1% of all male malignancies, and it is estimated that 8590 new cases were diagnosed in the United States in the year 2011.1 Despite its overall curability, approximately 360 men in the United States died in the year 2011 as a consequence of germ cell tumors. Although GCT is an uncommon malignancy, it is the most common malignancy among men aged 15 to 35. Seminoma accounts for half of all germ cell tumors, whereas nonseminoma germ cell tumors (NSGCTs) account for the remaining half. Although occasionally GCT occurs in children (generally yolk sac tumors), and in men over 70 (generally spermatocytic seminoma), by and large it is a malignancy of early adulthood, with the incidence of seminoma peaking in the 25- to 45-year-old group; the highest incidence of nonseminoma occurs in a slightly younger group of men (15- to 30-year-old group).2 Although the incidence of germ cell neoplasms in African American men is one fourth that of white men, African Americans have a higher disease stage at diagnosis than white men.3 Bilateral tumors occur in 2% to 4% of patients.4 Although risk factors for the development of this disease are largely unknown, a history of cryptorchidism appears to be related to the development of GCT. The risk of developing GCT is 10- to 40-fold higher in cryptorchid testes, and it is anticipated that 12% of all GCTs arise in cryptorchid testes. Conversely, from 1% to 5% of boys with a history of an undescended testicle will go on to develop GCT. The risk is highest (at approximately 5%) when a cryptorchid testis is retained intraabdominally, falls to 1% if retained in the inguinal canal, and appears to fall further if the undescended testis is surgically placed in the scrotum (orchiopexy) before 6 years of age. Despite reducing risk, orchiopexy does not completely eliminate the elevated risk of testis cancer in this population, as evidenced by the fact that one-fourth of GCTs arising in patients with a history of cryptorchidism occur in the normal, descended testicle, suggesting that systemic sequelae of cryptorchidism (i.e., testicular atrophy) is of greater etiologic importance than local or anatomic abnormalities.5,6 Further, males exposed to tobacco smoke in utero have a higher incidence of cryptorchidism,7 although a direct link between tobacco smoke and testis cancer has not been observed. In patients with testicular feminization syndrome and intraabdominally retained gonads, a 40-fold increase of GCT is seen. In phenotypically female but genotypically male patients, this syndrome may be mistaken for ovarian cancer.8 Approximately 1% to 3% of men with GCT have a family history, pointing to a possible genetic contribution. Brothers or sons of affected patients have between a 6- to 10-fold increased risk of developing the disease in their lifetime.9 Although the association between cryptorchidism and the development of GCT is indisputable, nearly 90% of men with GCT have no history of cryptorchidism. The contribution of orchitis, testicular trauma, or irradiation to the genesis of GCT is unknown, but it has been postulated that the final pathway common to all of these associations is testicular atrophy with increased follicle-stimulating hormone (FSH) drive. There is also growing support for the concept of transplacental damage to the fetal gonad by maternal estrogen levels as a contributing causative agent of germ cell cancer.10 Extragonadal GCTs appear to arise as a consequence of the malignant transformation of residual midline germinal elements, usually in the mediastinum or retroperitoneum, but occasionally in other locations such as the sacrococcygeal region and the pineal gland.11 Whether these residual germinal elements are a consequence of abnormal germ cell migration is not known, and other factors that may contribute to the development of extragonadal GCT have not been identified. The cytogenetic and molecular biology of GCT has only recently begun to be understood. Most interest has focused on changes involving chromosome 12. The isochromosome of the short arm of chromosome 12, i(12p), has been reported in up to 90% of GCT patients,12,13 and cases in which the isochromosome is not seen, excess genetic material is typically found on the p arm of chromosome 12.14 Although it is occasionally found in gastric cancer, i(12p) is nearly a pathognomic feature of GCT of all histologic types, whether of gonadal or extragonadal origin. This cytogenetic abnormality has been reported in carcinoma in situ tissue, suggesting it is an early marker, if not a cause, of germ cell tumorigenesis.15 In patients with mediastinal GCT, in whom there is an increased incidence of hematologic malignancies, often acute myeloid leukemia i(12p) can be found in both the mediastinal GCT tissue and in the leukemic cells,16 suggesting a common clonal origin for both. Similarly, i(12p) is found in malignant tissue of diverse histologies that has developed from the malignant transformation of teratoma, which is a component of nonseminomatous germ cell cancers. The presence of i(12p) has been utilized diagnostically in patients with midline carcinomas of unknown origin,17 allowing, in one series, a definitive diagnosis of GCT in 28% of patients and also serving as a marker of chemotherapy sensitivity (within the group of patients with midline malignancies of uncertain histogenesis).18 The presence of three or more copies of i(12p) has been correlated with poor prognosis GCT.19 Other changes in chromosome 12 are seen in GCT. Deletions of the terminal portion of 12q have been observed in up to 44% of patients with GCT, as well as in several GCT cell lines, suggesting the possibility of a tumor suppressor gene in this area.20 The gene or genes on i(12p) that may be involved in carcinogenesis have not been identified, although the oncogene KRAS, which is located on i(12p), has been implicated in GCT cell lines.21 Cyclin D2, encoded by the gene CCND2, has received much attention in normal testicular development as well as in the pathogenesis of GCT. It has an important role in cellular proliferation and its expression is tightly regulated throughout the cell cycle. It facilitates passage of cells though the G1 cell-cycle checkpoint. The gene is located on the short arm of chromosome 12 and it is overexpressed in nearly all GCTs. CCND2 is therefore a candidate GCT oncogene.20 Activated mutations in the protooncogene KIT have also been isolated from seminoma specimens.22 KIT encodes a transmembrane receptor tyrosine kinase that appears to have a role in normal spermatogenesis, and it is expressed in early fetal germ cells up to 12 weeks of gestation, but not beyond. In addition, it has also been detected in carcinoma in situ and seminoma cells reflecting a possible role in GCT oncogenesis.22,23 Epidermal growth factor receptor (EGFR) has also been found to be overexpressed in approximately 25% of the β-human chorionic gonadotropin (β-hCG)–expressing component of mixed GCTs.24 EGFR is a membrane protein that after binding to its ligand activates protein tyrosine kinase activity. This leads to activation of a cascade of biochemical and physiological responses that are involved in the mitogenic signal transduction of normal as well as malignant cells. A commonly used histologic classification of testicular neoplasms is derived from the Armed Forces Institute of Pathology classification schema of Dixon and Moore,25 which recognizes pure seminoma, as well as four other categories, each of which may occur with or without seminoma elements: (1) embryonal carcinoma, (2) teratoma, (3) teratoma with foci of embryonal carcinoma and choriocarcinoma (also termed teratocarcinoma), and (4) choriocarcinoma with and without embryonal elements. The World Health Organization (WHO) international classification divides tumors into those of single histologic type (seminoma, spermatocytic seminoma, embryonal carcinoma, choriocarcinoma, teratoma, and yolk sac tumors) and those of more than one type, in which the listing and estimation of relative proportion of each type is required.26 The major important differences between these two schemas are the recognition by the WHO schema of yolk sac tumors (endodermal sinus tumors) and spermatocytic seminoma as distinct categories (Table 86-1). Representative photomicrographs of various germ cell tumors can be seen in Figure 86-1. Table 86-1 Histologic Classification of Testicular Tumors* WHO, World Health Organization. *Data from Mostofi FK, Sesterhenn IA. Revised international classification of testicular tumors. In Jones WG, Harnden P, Appleyard I, editors. Germ Cell Tumors III. Oxford: Pergamon; 1994. p. 153. †Pugh RCB: Pathology of the Testis. Oxford: Blackwell; 1976. From Bosl GJ, Bajorin DF, Sheinfeld J, et al. Cancer of the testes. In Devita VT, editor. Principles and Practice of Oncology. 7th ed. Philadelphia: Lippincott Williams & Wilkins; 2005. Testicular cancers that are of nongerminal origin include specialized gonadal stromal neoplasms as well as sarcomas. These, in addition to adenocarcinoma (of the rete testis) and secondary (nonprimary) malignancies such as acute leukemia, lymphoma, carcinoma, and melanoma, comprise less than 5% of testicular neoplasms. The frequency and natural history of specific histologic subtypes are discussed below and summarized in Table 86-2. Table 86-2 Frequency and Age Distribution of Germ Cell Tumors The distribution of retroperitoneal lymph node metastases in nonseminomatous GCT has been described by Ray et al.27 and Donohue et al.,28 and they provide the basis for the specific surgical and therapeutic approaches described below. Figure 86-2 diagrams the anatomy and distribution of retroperitoneal lymph node involvement in GCT. A right-sided testicular primary is most frequently found to have interaortocaval nodal metastases, followed (in order of decreasing frequency) by the precaval and preaortic nodes. Contralateral nodal involvement occurs in 15% of patients, but in virtually every case with contralateral involvement, ipsilateral nodes were also involved. Left testis tumors most frequently have nodal spread to the left paraaortic, preaortic, and interaortocaval nodes, in that order. Suprahilar nodal involvement does not occur in patients with microscopic or low burden infrahilar disease (stage B1; see below), whereas 25% of patients with gross infrahilar disease have been found to have positive suprahilar nodes.27 Other nodal metastases are rare, but can occur in the external iliac and obturator nodes if the primary tumor invades the epididymis or extends up the spermatic cord, or in inguinal lymph nodes if the tumor extends through the tunica vaginalis to involve the scrotum, or if transscrotal exploration has been used.29 Seminomas account for 40% of all GCTs. The three distinct histologic patterns that have historically been described are classic seminoma, anaplastic seminoma, and spermatocytic seminoma. However, a clinical distinction can only be made between classic seminoma and spermatocytic seminoma, and the histologic definition of anaplastic seminoma (more than five mitotic figures per high-power field, cellular anaplasia, and tissue disruption) is of historic interest only, as neither response to therapy nor survival are adversely affected by the presence of anaplastic features.30 Classic seminoma usually manifests in the fourth or fifth decade. It is localized to the testes (stage I) in approximately 70% of patients and is metastatic to lymph nodes (generally stage II) in 25%.31 Metastases to lymph nodes occur in an orderly sequential fashion along draining lymph node chains. Visceral metastases are present at presentation in less than 5% of patients, and in general occur late in the course of the disease. Seminomas tend to appear homogeneous, with little necrosis or hemorrhage on gross inspection. Microscopically, they consist of sheets of uniform cells with large central hyperchromatic nuclei and clear or granular cytoplasm, which are divided by thin fibrous septations. Although lymphocytic infiltration and occasional giant cells may be seen, neoplasms in which any teratomatous or embryonal elements are seen are by definition not considered to be pure seminomas.25 Spermatocytic seminoma represents approximately 5% of all seminomas, and warrants special consideration. It generally occurs in the sixth decade. Although it is more likely to be bilateral than typical seminoma (6% vs. 2%), it is nonetheless a fairly indolent malignancy in which metastatic events are distinctly uncommon.32 Spermatocytic seminoma can be histologically distinguished from classic seminoma by the relative lack of compartmentalization of sheets of cells by fibrous septae, by the marked variation in cell size, and by the absence of lymphocytic infiltration. Pure embryonal carcinomas account for more than 60% of NSGCTs, although foci of embryonal elements may be found in a large majority of NSGCTs. Embryonal carcinoma occurs in 20- to 30-year-olds and is a highly malignant tumor characterized by rapid and bulky growth. In addition to lymphatic spread, these tumors are characterized by hematogenous spread of cancer cells, particularly to lung and liver. More than 60% of patients with embryonal carcinoma have metastases at presentation and the likelihood of occult nodal metastases in clinical stage I (confined to testis) tumors is a function of the proportion of the tumor that is composed of embryonal carcinoma.33 Furthermore, embryonal carcinoma has been reported to have the highest rate of venous invasion, lymphatic invasion, and tunica (capsular) invasion in both stage I and II tumors.30 Embryonal carcinomas exhibit focal necrosis and hemorrhage and microscopically are quite variable. Cellular features of embryonal carcinoma correlate with its more aggressive behavior and include anaplastic cells with embryoid features. Large pleomorphic nuclei, mitotic figures, and multinucleation are common as well. Stroma varies from loose to thick and fibrous.25 Mature teratoma has elements of one or more of the three germinal layers that are fully differentiated. Pure teratoma is uncommon and comprises less than 5% of GCT in adults. More than 75% of nonseminomas have been reported to have variable amounts of teratomatous elements, so that “pure” teratomas must be sampled carefully to exclude undifferentiated foci. The term teratocarcinoma refers to teratomas in combination with other elements, although some pathologists reserve the term for the combination of teratoma and embryonal carcinoma. When a teratoma has cellular and active stroma with mitotic figures, it is referred to as immature teratoma. Teratomas and teratocarcinomas are composed of solid and cystic spaces on cut surface, with areas of hemorrhage and necrosis. A histologic mix of fully differentiated cartilage, muscle, or epithelial tissue and malignant embryonal elements is seen. Predominant teratomatous features account for one-third of teratocarcinomas, whereas approximately two-thirds are mostly composed of nonteratomatous elements.25 Mature teratoma is the least aggressive of the nonseminoma GCTs, although up to 30% of adult patients with clinical stage I teratoma treated with orchiectomy alone will subsequently relapse, suggesting that pure teratomas should not be exempted from the usual clinical and pathological staging of GCT or from the usual subsequent therapeutic interventions.34 The natural history of teratocarcinomas lies somewhere between that of mature teratoma and embryonal carcinoma, but for practical (diagnostic and therapeutic) purposes, teratocarcinomas can be grouped with embryonal cell carcinomas. The likelihood that residual or recurrent masses after treatment are composed of mature teratoma is increased in patients with more extensive teratomatous elements at presentation and is discussed below. Choriocarcinoma is the most aggressive of the nonseminoma GCTs, with early hematogenous dissemination to lungs, liver, brain, and other visceral sites. Pure choriocarcinoma is exceedingly rare, accounting for less than 0.5% of all testicular malignancies, but focal areas of choriocarcinoma are seen in approximately 12% of embryonal and teratocarcinomas.35 Because advanced-stage disease at diagnosis is common, pure choriocarcinoma has a particularly poor prognosis. If pure choriocarcinomas are excluded, the specific histologic subtype of NSGCT does not have an influence on survival. The microscopic diagnosis of choriocarcinoma requires the presence of two cell types, syncytiotrophoblastic cells (giant cells with multiple hyperchromatic nuclei and abundant eosinophilic cytoplasm) and cytotrophoblasts (sheets of cells with single nuclei, abundant clear cytoplasm, and well-defined borders) arranged in papillary or pseudovillous patterns.25 Serum hCG is usually elevated in patients with choriocarcinoma; however, choriocarcinoma does not produce alpha-fetoprotein. Also known as endodermal sinus tumors, pure yolk sac tumors occur rarely, accounting for 1% of GCTs in adults. More commonly, yolk sac tumors in adults are found in combination with other tumor types, occurring in up to 70% of GCTs. In one series of 459 patients with stage I and II testicular cancer, the most common histology observed was a mixed one consisting of embryonal carcinoma plus yolk sac tumor and teratoma. Furthermore, the presence of teratoma and yolk sac tumor appeared to be associated with a large primary tumor size.35 Although pure yolk sac tumors are conventionally considered to be more aggressive with early hematogenous distribution,30 recent histologic reviews have suggested that patients in whom yolk sac tumor elements are present are at lower risk of relapse than patients in whom they are absent. However, the relatively high frequency with which yolk sac tumors and embryonal carcinoma are found together (50% of all tumors in some series) and the extremely rare occurrence of pure yolk sac tumors (1%) make this a difficult conclusion to substantiate.36 Yolk sac tumors occur more commonly in children, in whom they appear to be a less aggressive histologic subtype.37 The histology of yolk sac tumors, though characteristic, may be observed in several common patterns. These include a papillary pattern in which Schiller-Duval bodies (a fibrovascular core with a circle of cells around it, vaguely reminiscent of a glomerulus) can be seen, as well as microcystic, glanduloalveolar, and solid patterns. Nearly all patients with yolk sac tumors have elevations in serum AFP. In contrast to choriocarcinoma, yolk sac tumors do not produce AFP. Derived from the stromal and supporting cells surrounding germ cells, stromal cell tumors consist of Leydig cell tumors, Sertoli cell tumors, and granulosa cell tumors. As a group, they account for 3% to 4% of primary testicular tumors but constitute nearly 20% of childhood testicular tumors. Although by and large they are benign, up to 10% may metastasize.38 Histologic features appear to be useful in predicting the risk of disseminated disease, and management generally consists of orchiectomy and clinical staging with computed tomographic (CT) scan, without use of RPLND. These tumors may be estradiol secreting; gynecomastia occurs in 30% of Sertoli cell tumors and 15% of Leydig cell tumors. Although the large majority of testicular neoplasms in young men are germ cell tumors, in men more than 60 years of age, only 25% of malignancies will be of germinal origin. Testicular malignancies in this age group are predominantly composed of lymphomas,39 although metastases to the testicles, primarily from prostatic adenocarcinoma, lung carcinoma, and melanoma primary tumors must also be considered. Chemotherapeutics may not penetrate the blood–testis barrier efficiently; thus special consideration must be given to the treatment and subsequent surveillance of metastatic tumors (usually lymphomas) in the testis. The most common presentation of testicular cancer is testicular swelling (73% in one series of 450 patients).35 A commonly held misconception is that testicular cancers are by and large painless and that painful testicular masses need not be evaluated for malignancy. In fact, testicular pain is a manifesting feature of 18% to 46% of patients with GCT.35 Acute pain may be associated with torsion of the neoplasm, infarction or bleeding in the tumor, as well as with epididymitis. Signs and symptoms indistinguishable from acute epididymitis have been observed in up to one-fourth of patients with testicular neoplasms. Less commonly presenting symptoms will include gynecomastia in hCG-producing tumors such as choriocarcinoma (10%), back or flank pain from metastatic disease (10%), and infertility in less than 5% of tumors. Approximately 25% of patients with advanced disease have symptoms referable to their metastases, such as back pain.40 This is frequently the manifesting symptom in patients with primary retroperitoneal GCT. Pulmonary symptoms including shortness of breath, chest pain, and hemoptysis are rare but can occur in patients with advanced pulmonary disease or primary mediastinal GCT. The constellation of elicited symptoms and physical examination findings can offer a clue to the histology of a testicular mass. For example, it has been reported that pain more commonly occurred in patients who had embryonal carcinoma elements in their tumors than in those without that histologic feature (56% vs. 37%; P < 0.02). The same study reported a significantly higher incidence of testicular swelling when the primary tumors contained teratoma or yolk sac tumor elements.35 Primary tumors from patients with seminoma tend to be larger and more homogeneous, with diffuse involvement of the testicle, whereas embryonal and teratomatous elements tend to from smaller, discrete masses. Rapidly growing tumors, particularly those with extranodal dissemination, should raise the possibility of choriocarcinoma. These observations are of course no substitute for the appropriate clinical staging and histopathological evaluation.
Testicular Cancer
Epidemiology
Incidence
Etiology
Molecular Biology
Histology and Natural History
Overview of Histology
WHO*
British Tumor Board†
Seminoma
Seminoma
Typical (classic)
Anaplastic
Embryonal carcinoma
Malignant teratoma, undifferentiated
Teratoma
Malignant teratoma, differentiated
Mature
Immature
With malignant differentiation
Choriocarcinoma
Malignant teratoma, trophoblastic
Yolk sac tumor
Yolk sac tumor
Mixed germ cell tumors (specify components)
Malignant teratoma, intermediate
All GCTs (%)
Peak Age
HISTOLOGIC SUBTYPE
Seminoma
40
25–45
Classic and anaplastic
35
25–45
Spermatocytic
5
Average 65
Nonseminoma
60
15–35
Embryonal ± seminoma
24
20–30
Teratoma ± seminoma
5
Teratoma + embryonal, choriocarcinoma, or both
25
Choriocarcinoma (pure)
<1
Yolk sac tumor (pure)
<1
SITE OF ORIGIN
Gonadal
95–99
As above
Extragonadal
1–5
20–35
Overview of Natural History
Seminoma
Embryonal Carcinoma
Teratoma and Teratocarcinoma
Choriocarcinoma
Yolk Sac Tumors
Stromal Cell Tumors
Secondary (Metastatic) Neoplasms
Clinical Manifestations
Oncohema Key
Fastest Oncology & Hematology Insight Engine









