Tumors of the biliary tract and hepatocellular carcinoma (HCC) are complex tumors with heterogeneous carcinogenic mechanisms. Patients with hepatobiliary cancer have advances disease and need systematic therapy to palliate symptoms and extend survival. Development of effective systematic therapy is a significant unmet medical need. It is hoped that current and future clinical trials will identify additional effective systemic agents, combination systemic therapies, and combined modality options. The HCC community needs validated biomarkers to help identify the patients who will benefit most from emerging treatment options.
Key points
- •
There are limited effective chemotherapy options that have shown clinical benefit for patients with metastatic bile duct and hepatocellular carcinoma.
- •
Cancers of the biliary tract and primary tumors of the liver are challenging malignancies to treat in the advanced disease setting. These tumors are known as being chemotherapy resistant, as is well documented in the numerous negative clinical trials that have been conducted using conventional cytotoxic chemotherapy agents.
- •
There is emerging understanding of the unique biology of hepatobiliary cancers that will lead to development of targeted anticancer therapies for hepatobiliary cancers.
Introduction
Most patients with cancer of the bile ducts and liver eventually develop advanced disease that is not treatable with surgery, radiation therapy, or other liver-directed treatment options. These patients seek systemic therapy hoping for prolonged survival and palliation of tumor-related symptoms such as pain, anorexia, ascites, and fatigue. A large number of clinical trials have been conducted over several decades to evaluate a variety of chemotherapy agents in both tumor types. However, few chemotherapy regimens have produced level-1 evidence of clinical benefit to patients.
Introduction
Most patients with cancer of the bile ducts and liver eventually develop advanced disease that is not treatable with surgery, radiation therapy, or other liver-directed treatment options. These patients seek systemic therapy hoping for prolonged survival and palliation of tumor-related symptoms such as pain, anorexia, ascites, and fatigue. A large number of clinical trials have been conducted over several decades to evaluate a variety of chemotherapy agents in both tumor types. However, few chemotherapy regimens have produced level-1 evidence of clinical benefit to patients.
The challenges of developing an effective systemic therapy for advanced biliary tract and liver cancers
When evaluating systemic therapy for solid tumors, there are several factors that affect the design of clinical trials, selection of study end points, and the agents to be studied. The factors relevant to biliary tract cancer are summarized in this article.
Clinical Behavior
As is the case in many solid tumors, but particularly in cholangiocarcinoma, a wide range of tumor behavior is observed. Many of these tumors display indolent clinical behavior, may remain stable for many months, and seem to grow slowly and progress over years rather than months. These indolent intrahepatic cholangiocarcinomas (ICCs) often do not cause tumor-related symptoms until the tumor burden is extensive. Other cholangiocarcinomas have a more aggressive phenotype, progress rapidly, and result in more tumor-related morbidity.
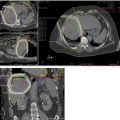
Imaging Characteristics
Tumors of the bile ducts appear radiographically in 2 general forms: the mass-forming ICCs appear as low-attenuation masses with irregular peripheral enhancement, and may be accompanied by liver capsule retraction, satellite nodules, and peripheral intrahepatic ductal dilatation. The periductal infiltrating cholangiocarcinomas are characterized by growth along dilated or narrowed bile ducts without mass formation. Both ICC and extrahepatic cholangiocarcinoma (EHCC) are highly desmoplastic tumors and tend to spread along bile duct walls and periductal tissue, which makes them challenging to image adequately with conventional imaging techniques in order to establish a baseline and assess radiographic tumor response.
Tumor Biology
The putative cell of origin in ICC and EHCC, the cholangiocytes, are multifunctional proproliferative cells. Cholangiocytes produce stimulatory cytokines (including transforming growth factor, interleukin-6, platelet-derived growth factor, tumor necrosis factor) as part of both autocrine and paracrine modulatory pathways. They mediate inflammation in the liver, which is known to play a key role in the initiation and maintenance of carcinogenesis. The liver-cholangiocyte microenvironment is thought to be procarcinogenic. Cholangiocytes are also able to detoxify foreign substances as a normal cellular function, and thus are inherently chemotherapy resistant.
Patient Comorbid Conditions
Patients with malignancies of the bile ducts or hepatocytes commonly have underlying liver disease that contributes in varying degrees to the initiation and progression of these cancers, as well as to whether the patient is a reasonable candidate for palliative systemic therapy. Comorbid liver-related conditions include fibrosis, cirrhosis, portal hypertension, altered drug metabolism, coagulopathy, hypoalbuminemia, thrombocytopenia, and ascites.
Cirrhosis can have a profound impact on tolerance and efficacy of anticancer drug therapy. The liver is central to the metabolism of most foreign and endogenous substances in the body. Hepatic metabolism involves oxidative pathways, primarily via the cytochrome P (CYP) 450 enzyme system, and additional metabolic steps, which include conjugation to a glucuronide, a sulfate, or glutathione. In cirrhosis, the total liver cell mass is reduced and distortion of the microcirculation of the liver and collagen deposition lead to impaired sinusoidal transport and reduced extraction of protein-bound substances. Hepatic cirrhosis not only decreases drug metabolizing enzyme activity but also alters the absorption, plasma protein binding, distribution, and renal excretion of drugs. Intrahepatic vascular shunts that develop as a consequence of cirrhosis allow drugs to be routed around hepatocytes, thus decreasing their first-pass extraction. However, all routes of hepatic metabolism are not equally impaired. As hepatic dysfunction progresses in cirrhotic patients, reduced synthesis of albumin occurs and leads to a decrease in the plasma protein binding of drugs. In the setting of hypoalbuminemia, for drugs that are more than 90% protein bound, the increase in the free drug fraction may have substantial clinical consequences. The CYP3A4 subfamily, the most common hepatic enzyme in adult humans, oxidizes more than 50% of currently used drugs. Several studies have shown significant decreases in the CYP3A protein levels in patients with cirrhosis, although contradictory data do exist. Therefore, it is difficult to predict the disposition of a drug in liver disease, and each agent must be studied individually to provide a rationale for adjusting doses.
Systemic therapy for biliary tract cancers: state of the clinical science
A large number of clinical trials of chemotherapy using single agents, doublets, and multidrug combinations have been published in recent years. Most trials were conducted to ascertain whether chemotherapy can provide clinical benefit to patients with advanced cancer of the biliary tract, in terms of palliation of tumor-related symptoms or increased survival. Most trials have been small, single-arm studies that commonly evaluate tumor response rate at the primary end point. For trials that follow the RECIST (Response Evaluation Criteria in Solid Tumors) 1.1 guidelines, tumor response is defined as complete response (disappearance of all target lesions) or partial response (at least a 30% decrease in the sum of diameters of target lesions, taking as reference the baseline sum diameters). Tumor response is an indication of antitumor activity, but may not correlate with clinical benefit to patients with advanced disease. A few prospective chemotherapy clinical trials have included subgroup analyses to ascertain whether there are differences in clinical outcome based on ICC, EHCC, or gallbladder cancer. However, because of the many challenges in conducting prospective clinical trials in these patients, there have not yet been separate trials in ICC and EHCC, or trials that are stratified by tumor location that are adequately powered to identify differences in chemotherapy benefit. Selected studies are summarized in Table 1 .
| Regimen | Study Phase | Sample Size | Response Rate (%) | PFS TTP (mo) | Overall Survival (mo) |
|---|---|---|---|---|---|
| Gemcitabine plus cisplatin vs gemcitabine | III | 410 | 81 a | 8.0 | 11.7 |
| 71 | 5.0 | 8.1 | |||
| Gemcitabine | II | 24 | 13 | — | 7.2 |
| Gemcitabine plus 5-fluorouracil | II | 42 | 1 | — | 9.7 |
| Gemcitabine plus S-1 | II | 35 | 34.3 | TTP 5.9 | 11.6 |
| Gemcitabine plus cisplatin | II | 43 | 28 | — | 8.4 |
| Gemcitabine plus capecitabine | II | 45 | 31 | — | 14 |
| GEMOX | II | 53 | 18.9 | PFS 4.8 | 8.3 |
| GEMOX plus cetuximab | II | 30 | 63 | — | 11.6 |
| CAPEOX | II | 65 | 37 (GB, ECC) | — | 12.8 |
| 0 (ICC) | 16.8 | ||||
| Capecitabine | II | 26 | 19 | — | 8.1 |
| FOLFIRI | II | 30 17 ICC 13 GB | 10 | PFS: 3 5.9 | OS: 5.9 9.75 |
a Tumor control rate = stable disease + partial response + complete response.
In April 2010, the Advanced Biliary Cancer (ABC)-02 trial was published, and this was the first phase III, randomized controlled trial in subjects with advanced biliary tract cancer. The ABC-02 trial compared doublet therapy consisting of gemcitabine and cisplatin with single-agent gemcitabine in 410 patients with locally advanced or metastatic biliary tract cancer. The combination of gemcitabine plus cisplatin showed improved progression-free survival (PFS) and overall survival (OS) compared with gemcitabine alone. In this trial, 59% (241 patients) had bile duct tumors, but the site of disease within the bile duct was not specified. After a median follow-up of 8.2 months, the combination group had significantly improved OS (11.7 vs 8.1 months). This regimen is currently considered the standard-of-care, first-line therapy for patients with advanced cancer of the bile ducts and gallbladder. The results of the ABC-02 trial have prompted many investigators to conduct trials in the second-line setting, as well as of novel targeted anticancer agents based on existing understanding of the molecular carcinogenesis of biliary tract cancers.
Advancing treatment of biliary tract cancer by incorporating targeted therapies into clinical trials
There remains a significant unmet medical need to develop effective and safe systemic therapy regimens for patients with advanced cholangiocarcinoma. The 2 main areas of unmet clinical need are to extend the benefit of gemcitabine and cisplatin, potentially by adding one or more targeted agents to the combination, and to develop effective regimens for patients who have failed first-line chemotherapy. However, the numerous single-arm clinical trials in advanced biliary tract cancer conducted over the previous 2 decades have made little progress. Some trials of single-agent targeted therapies, and combinations with cytotoxic agents, have been reported, as listed in Table 2 .
| Regimen | Study Phase | Sample Size | Response Rate (%) | PFS TTP (mo) | Overall Survival (mo) |
|---|---|---|---|---|---|
| Bevacizumab plus erlotinib | II | 49 | 18.4 | TTP 4.4 | 9.9 |
| Sorafenib | II | 31 | — | 3 | 9 |
| Sorafenib | II | 46 | 0 | PFS 3 | 9 |
| Lapatinib | II | 17 | — | PFS 1.8 | 5.2 |
| Selumetinib | II | 28 | 12 | 3.7 | 9.8 |
| Erlotinib | II | 42 | 8 | — | 7.5 |
| GEMOX plus Panitumumab | II | 46 | 33 | PFS 8.3 | 10.0 |
| GEMOX vs | RIII | 133 | 29 | PFS 4.2 | 9.5 |
| GEMOX plus erlotinib | First line | 135 | 15.7 | PFS 5.8 | 9.5 |
| Sunitinib | II, 2nd line | 56 | 8.9 | 1.7 | 4.8 |
| GEMOX plus bevacizumab | II, 1st line | 35 | 40 | 7 | 12.7 |
The foremost task in biliary tract cancer research is to improve understanding of the key molecular carcinogenetic mechanisms, with a focus on identifying the oncogenic driver mechanisms or mutations. Table 3 summarizes several of the potential therapeutic targets in biliary tract cancer that have been identified and, in some cases, evaluated in preclinical models. Given the high cost, the time required to complete, and low yield of empirical clinical trials, it is essential that a better understanding of the potential efficacy of new agents and combinations be obtained in the preclinical setting. In order to identify potential relevant molecular targets(s) or combinations of targets in ICC and/or EHCC, some concepts are particularly important:
- •
The results from measuring overexpression of a potential molecular target are highly variable depending on the quality of tumor specimen analyzed.
- •
Consistent overexpression of a receptor or a protein does not guarantee that it is a driver mechanism in the cancer or an actionable target for drug development.
- •
Screening of potential new agents and combinations in cholangiocarcinoma cell lines, of which there are few, is one step in assessing new therapeutics. However, cell lines have lost many characteristics of the original tumor and thus have significant limitations in predicting behavior of human tumors.
- •
Development of new anticancer drugs in cholangiocarcinoma must use appropriate preclinical models. The ideal models include the role of the tumor microenvironment.
- •
Genetic and genomic profiling using powerful bioinformatics techniques holds the promise of identifying validated molecular targets in both populations and individuals that provide rationales for determining suitable targets for drugs in ICC and EHCC.
- •
Future clinical trials should stratify by tumor location, if targets differ by site, and enrich the trial patient population by the target of interest.
| Pathway/Target | Rationale | Outcome |
|---|---|---|
| EGFR plus VEGF inhibition | Both EGFR and VEGF overexpression common in cholangiocarcinoma | Vandetanib, dual VEGF2/EGFR inhibitor significantly decreased in cell lines and xenografts |
| PDGF | Myofibroblasts are abundant in cholangiocarcinoma microenvironment and display procarcinogenic crosstalk with cancer cells, mediated partly by PDGF-B | Cytotoxic agent navitoclax induced apoptosis in CAF in a cholangiocarcinoma rat model |
| EGFR | ERB1 and ERB2 overexpression are prominent in biliary tract. Activating mutations rate very low | Several preclinical studies suggest benefit of therapeutic efficacy with EGFR inhibitors |
| COX | COX plays important role in biliary cancer cell signaling | COX-2 inhibitor NS-398 showed dose-dependent growth inhibition in rat model of cholangiocarcinoma |
| VEGF expression | VEGF expression linked to poor prognostic features and decreased survival | Some suggestion of clinical benefit shown in single-arm clinical trials |
| MEK ERK | MEK is critical element of Ras/Raf/MEK/ERK signal transduction pathway | Evidence of gallbladder cancer cell line growth inhibition by MEK inhibitor UO126 |
| c-MET (hepatocyte growth factor) | Several studies show overexpression of c-MET overexpression in preclinical cholangiocarcinoma models | NK4, which acts as an HGF antagonist and angiogenesis inhibitor, when transfected cholangiocarcinoma cell line clones, showed cell growth inhibition by arresting cell cycle progression |
| Molecular subclasses including inflammatory and proliferative subclasses | This important work may provide biomarkers of therapeutic efficacy to design biomarker-driven clinical trials | — |
| BRAF-activating mutations | Present in 7% of cholangiocarcinoma specimens | — |
| Hedgehog signaling | Sonic hedgehog ligand highly expressed by human cholangiocarcinoma tissue specimens and cell lines | In vitro inhibition of sonic hedgehog signaling decreased epithelial-mesenchymal transition and cholangiocarcinoma cell viability |
Related posts:
 Endoscopic and Percutaneous Approaches to the Treatment of Biliary Tract and Primary Liver Tumors
Intrahepatic Cholangiocarcinoma
Distal Cholangiocarcinoma
Endoscopic and Percutaneous Approaches to the Treatment of Biliary Tract and Primary Liver Tumors
Intrahepatic Cholangiocarcinoma
Distal Cholangiocarcinoma
 Hilar Cholangiocarcinoma
Hilar Cholangiocarcinoma
 An Emerging Role for Radiation Therapy in the Treatment of Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma
Palliation
An Emerging Role for Radiation Therapy in the Treatment of Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma
Palliation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


