Surgical site infections (SSIs) are a leading cause of healthcare-associated infections (HAIs). These infections can range in severity from nuisance to life-threatening; overall, they contribute to substantial patient suffering. A large portion of SSIs is considered preventable, and SSI prevention is a key patient safety issue that requires close collaboration between multiple healthcare personnel (HCP), including surgeons, nurses, anesthetists, and infection prevention personnel. This chapter provides updates to the diagnosis and epidemiology of SSIs with particular emphasis on risk factors, evidence-based strategies for prevention, and surveillance.
DIAGNOSIS
Clinically, a surgical wound is considered infected when purulent drainage is present at the incision site or there is evidence of abscess involving the surgical bed. However, other presentations of surgical wound infections also occur, including wound dehiscence, nonpurulent drainage, local erythema, induration, pain, or systemic signs of infection. Because of the varied presentation of SSIs, many of which overlap with noninfectious etiologies, no single clinical definition of SSI exists. Instead, the diagnosis of SSI is typically made based on a constellation of clinical and examination features, laboratory and microbiologic data, and radiography results.
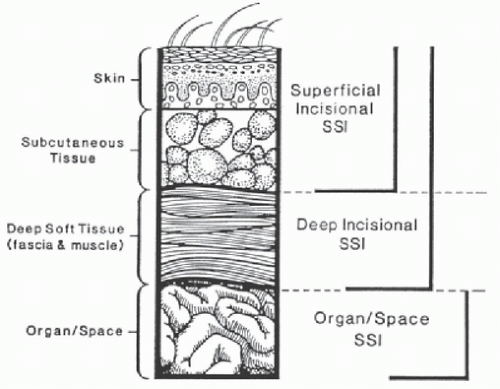
Despite the variability in clinical presentations of SSIs, specific definitions of SSI are used for epidemiologic and surveillance purposes. The U.S. Centers for Disease Control and Prevention’s (CDC) National Healthcare Safety Network (NHSN) provides the most commonly used SSI definitions. These definitions were designed to be objective and easy to apply, but also flexible enough to identify clinically relevant SSIs with varied presentations.1 NHSN categorizes SSIs into three groups: superficial incisional (involving the skin or subcutaneous tissue layers of the incision), deep incisional (involving muscle or connective tissue layers of the incision), and organ/space (involving structures, organs, or spaces deep to the incision) (Fig. 15-1, Table 15-1). Examples of organ/space infection include intra-abdominal abscess following colon surgery, periprosthetic joint infection following joint arthroplasty, and mediastinitis following cardiac surgery. Per NHSN definitions, surveillance for superficial incisional infections is conducted for 30 days, whereas surveillance for deep incisional and organ/space infections is conducted for 30 or 90 days, depending on the index surgical procedure.
It is important to note that surveillance definitions have changed over time and that various epidemiologic surveys and studies of SSI prevention have used variable casefinding methods (eg, active versus passive surveillance), criteria for inclusion (eg, index procedure versus all procedures), depth of infection (eg, superficial incisional, deep incisional, or organ/space infection), and surveillance periods (eg, 30 vs 90 days). For example, 10% fewer SSIs were identified when updated 2013 NHSN definitions that shortened surveillance periods were applied retrospectively to SSI surveillance data from a network of 35 hospitals and 2 ambulatory surgery centers.3 Therefore, it is important to understand the surveillance criteria used when interpreting SSI data from different surveys or time periods.
EPIDEMIOLOGY
Incidence
SSIs are the most common and most costly HAI in the United States, accounting for almost a quarter of all HAIs.4,5,6 While the risk of SSI is generally low, SSIs are common due to the volume of surgical procedures performed across the United States. In the United States, in 2010, over 51 million surgical procedures were performed in nonfederal U.S. hospitals, and over 53 million surgical and nonsurgical procedures were performed in United States ambulatory surgical centers.7 SSIs occur in 2%-5% of patients undergoing inpatient surgery.8,9 Rates are generally lower among procedures performed in outpatient settings. Overall, ˜300 000 SSIs occur each year, though this estimate likely underrepresents the true burden of SSI due to limitations in surveillance and diagnosis.10,11 SSIs are even more common in low- and middle-income countries, occurring in 1-24% of procedures performed.12
Overall, rates of SSI are decreasing in the United States. Among 148 hospitals participating in serial point prevalence surveys performed by the CDC, the rate of SSI decreased from 0.97 per 100 procedures in 2011 (n = 11 282 patients reviewed) to 0.56 per 100 procedures in 2015 (n = 12 299 patients reviewed; P = .001).13 Similarly, the publicly reported rates of SSI following abdominal hysterectomy and colon surgery decreased ˜10% in 2017 compared to the national baseline reported in 2016, though the decreases were not statistically significant.14 However, decreases in SSI have been modest compared to decreases observed in several other HAIs, including central line-associated bloodstream infection (CLABSI), catheter-associated urinary tract infection (CAUTI), methicillin-resistant Staphylococcus aureus (MRSA) bacteremia, and Clostridioides difficile infection.
FIGURE 15-1 NHSN categorization of surgical site infections. (From Horan TC, Gaynes RP, Martone WJ, Jarvis WR, Emori TG. CDC definitions of nosocomial surgical site infections, 1992: a modification of CDC definitions of surgical wound infections. Infect Control Hosp Epidemiol. 1992;13(10):606-608, Ref.2)
Rates of SSI vary by type of procedure and by setting. NHSN no longer routinely reports national rates of SSI following commonly performed procedures; therefore, most nationwide estimates currently used are from data reported almost 10 years ago. Clean-contaminated and dirty procedures, including procedures that enter a nonsterile viscera, have higher rates of SSI than clean procedures. For example, rates of SSI following colon, rectal, or other GI procedures range from 4% to 25%, while the rate of SSI following coronary artery bypass grafting is ˜3% and following hip or knee arthroplasty is 1% or lower.15,16 In most cases, rates of SSI at surgical centers are inversely associated with surgical volume. That is, the more procedures performed, the lower the rate of SSI.17,18,19 While referral centers typically care for more complex patients and perform higher risk procedures, these risks are often offset by high surgical volume and experience. Small community hospitals with low volume have higher rates of SSI than higher-volume community hospitals.20
TABLE 15-1 Summary of NHSN Surveillance Criteria for Surgical Site Infection Based on 2019 Definitions
Purulent drainage from a drain that is placed into the organ/space
Organism identified from aseptically obtained specimen or superficial incision deliberately opened by surgeon, attending physician, or designee and culture not obtained
A deep incision that spontaneously dehisces or is deliberately opened or aspirated by a surgeon, attending physician, or designee and organism identified from deep soft tissues of the incision and one or more of the following symptoms: fever >38°C, localized pain or tenderness
Organism identified from fluid or tissue in the organ/space
Diagnosis of superficial incisional SSI by surgeon, attending physician, or other designee
Abscess or other evidence of infection involving the deep incision that is detected on gross anatomical or histopathologic examination, or imaging test
Abscess or other evidence of infection involving the organ/space that is detected on gross anatomical or histopathologic examination, or imaging test evidence suggestive of infection
aInvolves part of the incision deeper than the fascial layer.
bInvolves any part of the body that is deeper than the muscle/fascial layers and was manipulated or entered during the operative procedure. Centers for Disease Control and Prevention. Surgical Site Infection (SSI) Event. 2019. https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf. Accessed October 16, 2019.
Patient Impact
SSIs lead to significant patient morbidity and mortality. Each SSI is associated with ˜7-11 additional postoperative hospital days.6,8,21,22 In total, patients with SSIs have 3.7 million excess hospital days each year.23 Surgical patients who develop an SSI have a risk of death that is between 2- and 11-fold higher than patients without an SSI;24,25,26 77% of deaths in patients with SSI are directly attributable to SSI.27 Investigators from the Agency for Healthcare Research and Quality (AHRQ) estimated excess mortality related to SSI was 0.026 (95% CI 0.009-0.059, meaning an additional 26 deaths occur for every 1000 SSIs).28 SSIs lead to ˜$25 000 of additional costs, though attributable costs of SSI vary depending on the type of operative procedure and the type of infecting pathogen.22,24,28,29,30,31,32,33,34,35,36 Overall, SSIs account for $3.5 billion to $10 billion annually in healthcare expenditures using the CPI (consumer price index for inpatient hospital services with all cost estimates adjusted for 2007 dollars).11
MICROBIOLOGY
SSIs are typically caused by pathogens inoculated at the time of surgery. The majority of SSIs are caused by the patient’s own flora. However, exogenous sources of wound contamination are possible.27,37 Most SSIs are caused by skin pathogens, though enteric pathogens are frequently seen in SSIs following GI procedures (Table 15-2). Overall, S aureus is the most common cause of SSI. While MRSA was previously a more frequent cause of SSI than methicillinsensitive S aureus (MSSA), rates of MRSA SSI have declined; MSSA is now a more common cause of SSI than MRSA.16,38 This trend is important because SSIs caused by resistant pathogens such as MRSA lead to even worse clinical outcomes than SSIs caused by susceptible pathogens.22,26 Outbreaks involving atypical organisms such as Mycoplasma, Ureaplasma, Candida and other fungi, Nocardia, Rhodococcus, and nontuberculous mycobacteria (including rapidly growing mycobacteria) are uncommon, but have been previously described.39,40,41,42,43,44
TABLE 15-2 Common Causes of Surgical Site Infections
Organism
Clean cardiac bypass and joint arthoplastiesa N = 6263 n (%); rank
a6262 complex surgical site infections (SSIs) identified after 680 489 procedures performed in 880 hospitals over a 4-year period.
b3988 complex SSIs identified after 532 694 procedures performed in 29 community hospitals over a 5-year period.
RISK FACTORS
SSI acquisition depends on exposure to bacteria and the host’s ability to control the inevitable bacterial contamination of a surgical wound. The likelihood of developing an SSI is a complex interaction among several variables including overall host characteristics (ie, age, immunosuppression, obesity, diabetes), effectiveness of antimicrobial prophylaxis, surgical site tissue condition and presence of foreign material, and degree of wound contamination.
Table 15-3 provides a summary of known SSI risk factors, which are also discussed in detail below. Some risk factors that increase risk of SSI are nonmodifiable, such as gender and age. However, other risk factors are modifiable, and their optimization can decrease the likelihood of developing an SSI.
Patient-Related, Nonmodifiable
Age Several studies identify the extremes of age as a risk factor for SSI. The risk of SSI is higher in infants compared to older children92 and higher among older adults compared to younger cohorts.45,46 With increasing age, the skin’s dermis and basement membrane thins. In addition, the skin loses its supply of cutaneous nerves and blood vessels. These physiologic changes contribute to slow or impaired wound healing.93,94
However, the risk of SSI may only increase up until a certain age. Kaye et al. found that after age 65, the risk of SSI decreased by 1.2% for each additional year of life.95 Therefore, the risk of SSI may be due to comorbidities and immunosuppression not directly due to increasing age. Furthermore, this result may indicate a selection bias of “healthier” older patients for surgery.
History of Radiation History of prior radiation therapy at the site of surgery increases SSI risk because of the risk of underlying tissue damage.47,96 Irradiated skin is hypovascular and easily injured with slight trauma. Given the damaged tissue and lack of perfusion, surgical incisions in locations with prior radiation treatment are more likely to develop a wound complication.
History of Prior Skin and Soft Tissue Infection History of a prior skin and soft tissue infection (SSTI) is another risk factor for SSI development.49 While not fully understood, the increased SSI risk among these patients may reflect differences in inherent immunity and susceptibility to infection.
Patient-Related, Modifiable
Diabetes Mellitus Patients with diabetes mellitus are more likely to develop SSIs. In a meta-analysis including 14 prospective studies, patients diagnosed with diabetes were twice as likely to develop an SSI compared to patients without a diagnosis of diabetes.50 The increased risk of SSI among patients with diabetes is consistent across multiple surgical procedures and is likely multifactorial.97 Patients with diabetes have a high incidence of small vessel disease, leading to impaired oxygen and nutrition delivery to peripheral tissues. Hypoxemia and lack of nutritional support reduce the systemic ability to prevent infection.98 Dronge et al. found that patients with a hemoglobin A1c level above 7% were significantly more likely to develop infectious complications compared to patients with a hemoglobin A1c level below 7%.99
Malnutrition Malnutrition is prevalent among surgical patients. One of the most commonly used markers of malnutrition is albumin, and hypoalbuminemia increases the risk of SSI.52,100 Hypoalbuminemia may lead to increased risk of SSI through several mechanisms. First, hypoalbuminemia can lead to poor tissue healing, decreased collagen synthesis, and granuloma formation in surgical wounds.101,102,103 These factors can impair wound healing and predispose the tissue to infection. Second, low albumin impairs macrophage activation and induces macrophage apoptosis, which decreases innate immunity response.103,104 Lastly, hypoalbuminemia can lead to tissue edema and leakage of interstitial fluid into the surgical wound.105 This fluid can serve as a medium for bacteria to proliferate and ultimately lead to infection.
TABLE 15-3 Summary of Known Surgical Site Infection Risk Factors
Risk factor
Pathophysiology
Patient-related, nonmodifiable
Age
The skin’s dermis and basement membrane thin with increasing age, and the skin loses its supply of cutaneous nerves and blood vessels, which can lead to poor wound healing.45,46
History of radiation
Radiation therapy produces underlying tissue damage and contributes to poor wound healing.47,48
History of prior SSTI
A prior history of SSTIs may be related to differences in inherent immunity and susceptibility to infection.49
Patient-related, modifiable
Diabetes
Hyperglycemia impairs innate immunity mechanism to fight bacteria. In addition, elevated glucose leads to glycosylation of proteins, which in turn slows wound healing.50,51
Malnutrition
Poor nutrition leads to poor tissue healing, decreased collagen synthesis, and granuloma formation in surgical wounds. Low albumin impairs macrophage activation and induces macrophage apoptosis, which decreases innate immunity response. Hypoalbuminemia can lead to tissue edema and leakage of interstitial fluid into the surgical wound.52
Smoking
Tobacco smoke impairs wound healing by vasoconstriction leading to relative ischemia, reduced inflammatory response, and alteration in collagen metabolism.53
Obesity
Decreased blood flow in adipose tissue leads to less oxygen and antibiotic delivery.54,55,56
Immunosuppressive medications and conditions
Immunosuppressive medications or clinical conditions blunts the inflammatory phase of wound healing.57,58,59,60,61
Decreased tissue oxygenation
Decreased tissue oxygenation leads to diminished oxidative killing by neutrophils and impaired tissue healing caused by reduced collagen formation, neovascularization, and epithelialization. Low oxygen levels may decrease the efficacy of perioperative antibiotics62,63,64,65,66
Perioperative hypothermia
Perioperative hypothermia impairs host defenses against surgical wound contamination: vasoconstriction causing reduced tissue perfusion to wounded tissue with reduced access for key immune cells, decreased motility of key immune cells, and reduced scar formation.67
Postoperative hyperglycemia
Cellular functions of leukocyte adherence, chemotaxis, phagocytosis, and bactericidal activity are improved by insulin and better glycemic control, suggesting a direct relation between cellular function deficits and elevated blood glucose.68
Anticoagulation
Anticoagulants can cause of persistent oozing of the incision, slow wound healing.69,70,71,72
Blood transfusions
Blood transfusions impact the risk of infection by modulating the immune system.73
Endogenous sources
Wound contamination from patient
Shaving creates microscopic cuts in the skin that later serve as niduses for bacteria to multiply.27
Absence of appropriate barrier devices and drapes allows bacteria from deeper skin layers and hair follicles to recolonize the surgical site during the operation.
Lack of or inappropriate administration of perioperative antibiotics will not prevent the inevitable burden of microorganisms at surgical site.74
Without appropriate surgical site preparation, soil and transient organisms will not be removed.75
Wound classification delineates the degree of contamination of a surgical wound at the time of the operation.76
Exogenous sources
Wound contamination from operating room personnel
Transition of skin flora on the hands of healthcare personnel to the patient and operating room from lack of appropriate hand-washing or gloving to surgical sites.77
Movement of microorganisms from surgical staff’s hair, mouths, body, or shoes to the operating room contaminates surgical wounds.77,78,79,80
Airborne contamination
Increasing the number of microorganisms in the operating room environment increases opportunity for SSI. Most of the airborne contamination comes from persons present in the operating room and their movements.81,82,83,84
Operation length
Longer operative duration is associated with increased wound contamination, increased damage to wound cells, and the local environment.85,86
Surgical technique
Not maintaining adequate blood supply, not gently handling tissue, inadvertent entry into hollow viscus, leaving behind devitalized tissue, inappropriate use of drains and sutures, and inappropriate postoperative wound management.27
Foreign material
Foreign material promotes inflammation at the surgical site and increases the risk of SSI.87,88
Intra-articular steroid injection
Infection may be introduced at the time of injection, especially if rigorous antisepsis is not applied. May decrease the host immune response to the introduction of such bacteria.38
Periarticular joint injections
Injections are often prepared without the use of a sterile hood; infections can be introduced when these injections are compounded or at the time of infusion, as catheters are commonly used to deliver the medications.89
Wound care
Wounds that remain uncovered after surgery may be subject to environmental contamination or ongoing drainage that decreases the integrity of the surrounding skin.90,91
Tobacco Use Tobacco use is associated with adverse outcomes following surgery, including SSI. Postoperative wound healing complications occur more often in smokers and former smokers compared to those who never smoked. A systematic review identified four randomized trials that assessed the effect of preoperative smoking cessation (4- to 8-week interval of abstinence) on postoperative wound healing. This study showed that current or past smokers had an increased risk for postoperative infection (OR 1.9, CI 1.0-3.5).53
The many compounds that constitute tobacco smoke impair wound healing and increase SSI risk through several mechanisms.106,107,108 The physiologic mechanisms include vasoconstriction, which causes relative ischemia of operated tissues. Tobacco smoke also leads to a reduced inflammatory response and impaired innate immune system response to bacteria.108 Lastly, the elements in tobacco smoke can alter collagen metabolism, which is essential for skin and tissue integrity.
Obesity Obesity is another risk factor associated with developing SSI. One meta-analysis included 20 studies that evaluated SSI outcomes in orthopedic surgeries. The authors found that the risk of SSI for patients with obesity was almost two times the SSI risk for patients without obesity (RR 1.915; 95% CI 1.53-2.40).54 Studies including colorectal surgery patients (OR 1.59; 95% CI 1.32-1.91)109 and coronary artery bypass surgery patients (OR, 1.8; 95% CI 1.4-2.3)55 have reported similar conclusions. An additional recent study also found a trend of increasing risk of SSI for almost all surgery types when body mass index (BMI) increased from normal to morbidly obese.56
Obese patients may be at increased risk for SSI because of depth of adipose tissue, creation of dead space, and decreased blood flow in adipose tissue. Without adequate blood flow reaching the tissues, surgical wounds are less likely to heal. Decreased blood flow may also reduce antibiotic delivery and increase wound tension.85,110
Immunosuppressive Medications and Conditions Patients with suppressed immune systems are at increased risk of SSI because the inflammatory phase of wound healing may be blunted. The increase in SSI risk is seen in patients with various levels of immunosuppression, including transplant recipients, patients undergoing chemotherapy, and other patients taking immunosuppressing medications.57,58,59,60,111 Glucocorticoids, on the other hand, may not affect SSI risk as strongly as other immunosuppressive therapies.61 Some degree of anti-inflammation may prevent wounds from becoming chronically inflamed, while significant suppression of inflammation can prevent wound healing.112,113
Decreased Tissue Oxygenation Low oxygenation also increases the risk of SSIs. Oxygen tension is often low in wounds and in colorectal anastomoses at the end of surgery. This may reduce bacterial eradication, the body’s defenses against bacteria, and tissue healing. Possible mechanisms include diminished oxidative killing by neutrophils and impaired tissue healing caused by reduced collagen formation, neovascularization, and epithelialization.62,63,64,65 Further, many of the antibiotics used perioperatively for SSI prophylaxis are oxygen-dependent in their effect,66 and low oxygen levels may decrease their effectiveness.
Perioperative Hypothermia Maintaining normal body temperature is vital for the body to maintain its normal function. However, many factors that patients are exposed to in the operating room can cause hypothermia: anesthetic drugs, cold operating room, skin antisepsis, cold irrigation of a patient with the body uncovered, and the use of intravenous solutions. Most cellular functions are temperature-dependent, and hypothermia also provokes systemic responses.67 Several mechanisms help to explain why perioperative hypothermia impairs host defenses against surgical wound contamination, including vasoconstriction and subsequent diminished perfusion, decreased motility of key immune cells, and reduced scar formation, which is necessary to prevent wound dehiscence and recontamination.
Postoperative Hyperglycemia Postoperative hyperglycemia may increase SSI risk more than a diagnosis of diabetes. Hyperglycemia impairs innate immunity mechanism to fight bacteria. In addition, elevated glucose leads to glycosylation of proteins, which in turn slows wound healing.51 Latham et al. found that hyperglycemia during the immediate postoperative period was an independent risk factor for developing SSI even among patients without a history of diabetes and the risk of infection correlated with the degree of glucose elevation.68 Patients with blood glucose of 200 mg/dL or higher within 48 hours after surgery had 2.5 times the odds of developing an SSI as patients with glucose <200 mg/dL.
Anticoagulation While postoperative anticoagulation is an evidence-based practice to prevent deep vein thrombosis in the postoperative period, anticoagulants may increase the risk of SSIs. Several studies have implicated anticoagulation therapy as a cause of persistent oozing of the incision, slow wound healing, and subsequent SSIs.69,70,71,72
Only gold members can continue reading. Log In or Register to continue
 Role of the Microbiology Laboratory and Molecular Diagnostics in Healthcare Epidemiology and Infection Prevention
Role of the Microbiology Laboratory and Molecular Diagnostics in Healthcare Epidemiology and Infection Prevention
 Healthcare-Associated Infections Related to the Use of Intravascular Devices
Healthcare-Associated Infections Related to the Use of Intravascular Devices
 MDRO Infections: Gram-Negative Organisms
MDRO Infections: Gram-Negative Organisms



