Cervical cancer is the second most common cancer in women worldwide. In developed countries screening programs have decreased the incidence of this disease and improved the detection of early-stage disease amenable to surgical intervention. This article discusses the scope of surgical treatment of cervical carcinoma, including conization for the earliest-stage and lowest-risk patients, radical hysterectomy with lymphadenectomy, radical trachelectomy for appropriately selected patients who desire future fertility, and pelvic exenteration for recurrent disease. In addition, current surgical advances such as surgical staging methods and minimally invasive approaches are discussed.
Cervical carcinoma is the second most common cancer worldwide with global estimates exceeding 530,200 new cases and 275,000 deaths in 2010. In developed countries, screening programs have dramatically decreased the incidence of this disease, with estimates of 12,710 new cases and 4290 deaths in the United States in 2011. Improved screening has increased the proportion of early-stage disease amenable to surgical intervention. Although primary chemoradiation achieves equal cure rates to radical hysterectomy with lymphadenectomy for early-stage disease, treatment must be chosen carefully taking into account side effect profiles, medical comorbidities, histopathologic data, reproductive plans, and patient and physician preference. These are important considerations in a population that is generally younger than in other gynecologic malignancies and includes a significant portion of women in their reproductive years. Many of these women with early-stage disease achieve a cure and have a lengthy lifespan, shifting focus of treatment toward quality-of-life issues and maintaining hormone production and reproductive options.
Cervical carcinoma remains a clinically staged disease because of the predominance of patients treated with definitive radiation globally. However, clinical staging is often inaccurate in estimating the true extent of disease, with many patients being upstaged from surgical findings. In developed countries, surgery remains the mainstay of treatment of early disease. The scope of surgical treatment of cervical carcinoma is discussed here and includes conization for the earliest-stage and lowest-risk patients, radical hysterectomy with lymphadenectomy, radical trachelectomy for appropriately selected patients who desire future fertility, and pelvic exenteration for recurrent disease. In addition, current surgical advances such as surgical staging methods and minimally invasive approaches are discussed.
Radical hysterectomy for early-stage disease
Radical hysterectomy is the standard surgical approach for early-stage cervical cancer, with the exception of the earliest-stage and lowest-risk disease. Stage IA1 squamous cell carcinoma without lymphovascular space invasion (LVSI) carries a small risk of metastatic spread and may be treated with cervical conization or simple hysterectomy alone. The risk of lymph node metastasis in this group is less than 1% and does not require lymphadenectomy. Patients with IA2, IB1, early IIA, and some IB2 cancers are candidates for radical hysterectomy with pelvic and para-aortic (PA) lymphadenectomy.
The operation originally described by Meigs in 1944 and classified by Piver and colleagues in 1974 involves the en bloc resection of the uterus, parametrium, and upper vagina in varying degrees of radicality. The Piver-Rutledge-Smith classification described 5 types of hysterectomy based on extent of uterine vascular and ligamentous resection as outlined in Table 1 . The type II and III classification are most commonly performed for cervical carcinoma; however, the degree of vaginal resection has been criticized by some as overly aggressive and rarely necessary. Type IV and type V procedures are rarely performed, and have been largely replaced by radiation therapy and pelvic exenteration.
| Classification | Description | Disease |
|---|---|---|
| Type I: extrafascial hysterectomy | Simple hysterectomy | Benign IA1 cervical cancer |
| Type II: modified radical hysterectomy | Uterine artery ligation at the ureters Proximal cardinal and uterosacral ligaments Upper third vagina | IA2 cervical cancer |
| Type III: radical hysterectomy | Uterine artery ligation at its origin Entire cardinal and uterosacral ligament Upper half vagina | IA2–IIA cervical cancer |
| Type IV: extended radical hysterectomy | Dissection of ureter off vesicouterine ligament Resection of superior vesicle artery Upper three-fourths vagina | Central recurrence |
| Type V: partial exenteration | Resection of portion of bladder or ureter with reimplantation | Central recurrence |
A new classification was published in 2008 by Querleu and Morrow that describes 4 categories of radical hysterectomy with subcategories, where appropriate, as outlined in Table 2 . Lymphadenectomy is considered separately, and divided into 4 levels. This simplified classification is based on lateral dissection, and takes into account the curative intent and adverse effects of the procedure, namely bladder dysfunction. Devised in the spirit of international standardization for research and communication purposes, this system can be applied to both fertility-sparing surgery and hysterectomy, and adapted for open, vaginal, laparoscopic, and robotic approaches.
| Radical Hysterectomy | Lymphadenectomy | ||
|---|---|---|---|
| Type A | Extrafascial hysterectomy Paracervix medial to ureter <10 mm vagina | Level 1 | External and internal iliac |
| Type B | Partial uterosacral and vesicouterine ligaments Paracervix at the ureter 10 mm vagina B1: without lateral paracervical lymph nodes B2: with lateral paracervical lymph nodes | Level 2 | Common iliac (including presacral) |
| Type C | Uterosacral ligaments at the rectum Vesicouterine ligaments at the bladder Paracervix at the internal iliac vessels 15–20 mm vagina C1: with hypogastric nerve preservation C2: without hypogastric nerve preservation | Level 3 | Inframesenteric PA |
| Type D | Complete paracervical resection D1: with hypogastric vessels D2: with hypogastric vessels and adjacent fascia and muscular structures | Level 4 | Infrarenal PA |
For patients with early-stage disease, definitive chemoradiation achieves equal cure rates to radical hysterectomy and pelvic lymphadenectomy. However, surgical treatment confers several benefits, especially in a younger population with a longer life expectancy if cure is attained. Surgery allows complete assessment of the extent of disease and tailoring of further treatment if necessary. Ovarian function is preserved in premenopausal patients, and if future radiotherapy is anticipated the opportunity is provided to transpose the ovaries out of the radiation field. Although vaginal length is slightly reduced, caliber is maintained and the risk of radiation fibrosis, atrophy, and stenosis avoided. Sexual functioning in general is underreported, and reports vary by radicality of the surgery. However, a retrospective study 5 years out from either radical hysterectomy with lymphadenectomy or radiation therapy reported significantly improved sexual function in the surgical group compared with the radiation group, and was comparable with age-matched controls without a history of cancer.
However, surgical treatment carries its own set of risks, complications, and side effects, many of which are perioperative considerations. Radical surgery naturally carries a risk of intraoperative injuries to pelvic vessels and nerves, the ureters, bladder, and rectum, and blood loss generally ranges from 500 to 1500 mL for open radical procedures. The postoperative period is inevitably complicated by voiding dysfunction and prolonged recovery of bowel function. Less common complications include infectious morbidity, venous thromboembolic events, fistula, lymphocysts, and ureteral stricture. Late complications include bladder atony and lymphedema, both of which can prove distressing to patients and significantly affect quality of life. Long-term voiding dysfunction may necessitate timed voiding with accessory muscle use or even intermittent self-catheterization and has been reported in 0.8% to 8.3% of patients.
Surgical damage to the pelvic autonomic nerves has been implicated in defecatory, voiding, and sexual dysfunction. In an effort to maintain radical resection and minimize these long-term complications, the nerve-sparing radical hysterectomy was developed. The technique as described by Trimbos and colleagues involves dissection of the hypogastric nerve lateral to the uterosacral ligament and underneath the ureter, lateralizing the hypogastric plexus within the parametrium, and preservation of the most distal portion of the nerve in the posterior vesicouterine ligament. Postoperative recovery of bladder function and quality of life 1 year from surgery were found to be significantly improved with nerve-sparing radical hysterectomy in a prospective randomized trial by Wu and colleagues. Oncologic outcomes are likely not affected by the nerve-sparing procedure, but long-term prospective studies are needed.
Minimally invasive approaches to radical hysterectomy
In the last 20 years, minimally invasive approaches have been pursued to decrease the morbidity of surgery and improve recovery times, and maintain surgical and oncologic outcomes. With the advent of and subsequent improvement in laparoscopic surgical techniques, minimally invasive approaches became a reality in the treatment of cervical carcinoma. Dargent and Salvat performed the first lymphadenectomy in women with cervical cancer in 1989, and later combined the procedure with radical vaginal hysterectomy. Multiple subsequent reports confirmed decreased blood loss and transfusion rates, shorter hospital stays, less postoperative pain, and similar recurrence rates, but longer operating times with laparoscopic-assisted radical vaginal hysterectomy compared with abdominal radical hysterectomy.
With further improvement and acceptance of laparoscopic technologies, total laparoscopic radical hysterectomy has gained momentum. Its safety and feasibility have been well established, with multiple investigators reporting reduced blood loss, shorter hospital stay, maintenance of lymph node counts, and decreased perioperative morbidity. One of the largest studies to date by Putambekar and colleagues included 248 patients and reported a median operative time of 92 minutes, median blood loss of 165 mL, median hospital stay of 3 days, and median number of lymph nodes of 18. Other studies have generally reported longer operating times of 203 to 344 minutes and shorter hospital stays of 1 to 2 days. Although longer follow-up is needed, intermediate follow-up times have shown similar oncologic outcomes among laparoscopic and abdominal radical hysterectomy. Both Spirtos and colleagues and Putambekar and colleagues report 3-year follow-up data on patients with IA2 to IB cervical cancer treated with laparoscopic radical hysterectomy and lymphadenectomy with recurrence rates of 5.1% and 2.8%, respectively. Pomel and colleagues also reported a 5-year survival rate of 96% in patients with stage IA2 to IB1 cervical cancer treated with laparoscopic radical hysterectomy. Li and colleagues compared laparoscopic and abdominal radical hysterectomy and lymphadenectomy in stage IB to IIA cervical cancer, reporting similar respective recurrence rates (13.75% vs 12%, P >.05) and mortality (10% vs 8%, P >.05) at 26 months’ median follow-up.
Despite the advantages and equivalent outcomes there are still barriers to treating cervical cancer with minimally invasive approaches. Complex radical procedures performed with traditional laparoscopy are associated with long learning curves and increased operating time. They also require an expert assistant and are limited by two-dimensional viewing and lack of dexterity. Furthermore, many practicing gynecologic oncologists and fellows, when surveyed, believed that their laparoscopic training was inadequate to perform such procedures.
Recent advances in minimally invasive surgery have incorporated the use of robotic technology. The da Vinci surgical system (Intuitive Surgical, Sunnyvale, CA, USA) is a robotic surgical platform that was approved for gynecologic procedures in 2005. Three-dimensional stereoscopic viewing and wristed instruments provide improved visualization, precision, and dexterity, and allow a single surgeon to perform complex procedures with a less experienced bedside assistant. Robotically assisted laparoscopic surgery has also been shown to have a shorter learning curve and decreased operating time when compared with conventional laparoscopy.
Several investigators have confirmed the safety and feasibility of robot radical hysterectomy, with operative characteristics similar to traditional laparoscopy. A multi-institutional study of 42 patients who underwent robotic-assisted type II or III radical hysterectomy reported favorable operative characteristics and a low complication rate. Overall median operative time was 215 minutes, median estimated blood loss was 50 mL, median lymph node count was 25, and median hospital stay was 1 day. Intraoperative complications included 1 conversion to laparotomy and 1 ureteral injury. The postoperative complication rate was 12% and included infectious morbidity (7.1%), deep venous thrombosis (2.4%), and prolonged catheterization (2.4%). A series by Magrina and colleagues compared 27 patients undergoing robotic radical hysterectomy with matched patients who underwent radical hysterectomy by traditional laparoscopic or open approaches. These investigators reported decreased blood loss and shorter hospital stays in the laparoscopic and robotic group compared with the laparotomy group, and decreased operative times in the robotic and laparotomy group compared with the laparoscopic group. The robotic group had no intraoperative complications or conversion to laparotomy.
Recently, oncologic outcomes of robotic-assisted radical hysterectomy have been evaluated. A retrospective analysis was conducted comparing 63 consecutive robotic type III radical hysterectomies for early-stage (IA1–IIB) cervical cancer with a historical cohort of open type III radical hysterectomies. The robotic and open groups did not differ with regards to age, body mass index (calculated as weight in kilograms divided by the square of height in meters), histology, or stage. As with other studies, patients in the robotic group benefited from decreased blood loss, shorter hospital stays, and increased lymph node retrieval. Progression-free survival (94% vs 89%, P = .27) and overall survival did not differ between groups at 36 months’ follow-up. Although longer follow-up is needed, with clear benefits to minimally invasive surgery and mounting evidence of equivalent surgical and oncologic outcomes, robotics offers a platform to overcome barriers to use of minimally invasive approaches in patients with early-stage cervical cancer. A prospective multicenter trial is under way to establish equivalence of total laparoscopic or robotic radical hysterectomy compared with abdominal radical hysterectomy with respect to disease-free survival. This biphasic trial will enroll 740 patients and evaluate morbidity, cost-effectiveness, recurrence patterns, quality of life, intraoperative sentinel node sampling, and overall survival.
Minimally invasive approaches to radical hysterectomy
In the last 20 years, minimally invasive approaches have been pursued to decrease the morbidity of surgery and improve recovery times, and maintain surgical and oncologic outcomes. With the advent of and subsequent improvement in laparoscopic surgical techniques, minimally invasive approaches became a reality in the treatment of cervical carcinoma. Dargent and Salvat performed the first lymphadenectomy in women with cervical cancer in 1989, and later combined the procedure with radical vaginal hysterectomy. Multiple subsequent reports confirmed decreased blood loss and transfusion rates, shorter hospital stays, less postoperative pain, and similar recurrence rates, but longer operating times with laparoscopic-assisted radical vaginal hysterectomy compared with abdominal radical hysterectomy.
With further improvement and acceptance of laparoscopic technologies, total laparoscopic radical hysterectomy has gained momentum. Its safety and feasibility have been well established, with multiple investigators reporting reduced blood loss, shorter hospital stay, maintenance of lymph node counts, and decreased perioperative morbidity. One of the largest studies to date by Putambekar and colleagues included 248 patients and reported a median operative time of 92 minutes, median blood loss of 165 mL, median hospital stay of 3 days, and median number of lymph nodes of 18. Other studies have generally reported longer operating times of 203 to 344 minutes and shorter hospital stays of 1 to 2 days. Although longer follow-up is needed, intermediate follow-up times have shown similar oncologic outcomes among laparoscopic and abdominal radical hysterectomy. Both Spirtos and colleagues and Putambekar and colleagues report 3-year follow-up data on patients with IA2 to IB cervical cancer treated with laparoscopic radical hysterectomy and lymphadenectomy with recurrence rates of 5.1% and 2.8%, respectively. Pomel and colleagues also reported a 5-year survival rate of 96% in patients with stage IA2 to IB1 cervical cancer treated with laparoscopic radical hysterectomy. Li and colleagues compared laparoscopic and abdominal radical hysterectomy and lymphadenectomy in stage IB to IIA cervical cancer, reporting similar respective recurrence rates (13.75% vs 12%, P >.05) and mortality (10% vs 8%, P >.05) at 26 months’ median follow-up.
Despite the advantages and equivalent outcomes there are still barriers to treating cervical cancer with minimally invasive approaches. Complex radical procedures performed with traditional laparoscopy are associated with long learning curves and increased operating time. They also require an expert assistant and are limited by two-dimensional viewing and lack of dexterity. Furthermore, many practicing gynecologic oncologists and fellows, when surveyed, believed that their laparoscopic training was inadequate to perform such procedures.
Recent advances in minimally invasive surgery have incorporated the use of robotic technology. The da Vinci surgical system (Intuitive Surgical, Sunnyvale, CA, USA) is a robotic surgical platform that was approved for gynecologic procedures in 2005. Three-dimensional stereoscopic viewing and wristed instruments provide improved visualization, precision, and dexterity, and allow a single surgeon to perform complex procedures with a less experienced bedside assistant. Robotically assisted laparoscopic surgery has also been shown to have a shorter learning curve and decreased operating time when compared with conventional laparoscopy.
Several investigators have confirmed the safety and feasibility of robot radical hysterectomy, with operative characteristics similar to traditional laparoscopy. A multi-institutional study of 42 patients who underwent robotic-assisted type II or III radical hysterectomy reported favorable operative characteristics and a low complication rate. Overall median operative time was 215 minutes, median estimated blood loss was 50 mL, median lymph node count was 25, and median hospital stay was 1 day. Intraoperative complications included 1 conversion to laparotomy and 1 ureteral injury. The postoperative complication rate was 12% and included infectious morbidity (7.1%), deep venous thrombosis (2.4%), and prolonged catheterization (2.4%). A series by Magrina and colleagues compared 27 patients undergoing robotic radical hysterectomy with matched patients who underwent radical hysterectomy by traditional laparoscopic or open approaches. These investigators reported decreased blood loss and shorter hospital stays in the laparoscopic and robotic group compared with the laparotomy group, and decreased operative times in the robotic and laparotomy group compared with the laparoscopic group. The robotic group had no intraoperative complications or conversion to laparotomy.
Recently, oncologic outcomes of robotic-assisted radical hysterectomy have been evaluated. A retrospective analysis was conducted comparing 63 consecutive robotic type III radical hysterectomies for early-stage (IA1–IIB) cervical cancer with a historical cohort of open type III radical hysterectomies. The robotic and open groups did not differ with regards to age, body mass index (calculated as weight in kilograms divided by the square of height in meters), histology, or stage. As with other studies, patients in the robotic group benefited from decreased blood loss, shorter hospital stays, and increased lymph node retrieval. Progression-free survival (94% vs 89%, P = .27) and overall survival did not differ between groups at 36 months’ follow-up. Although longer follow-up is needed, with clear benefits to minimally invasive surgery and mounting evidence of equivalent surgical and oncologic outcomes, robotics offers a platform to overcome barriers to use of minimally invasive approaches in patients with early-stage cervical cancer. A prospective multicenter trial is under way to establish equivalence of total laparoscopic or robotic radical hysterectomy compared with abdominal radical hysterectomy with respect to disease-free survival. This biphasic trial will enroll 740 patients and evaluate morbidity, cost-effectiveness, recurrence patterns, quality of life, intraoperative sentinel node sampling, and overall survival.
Fertility-sparing radical surgery
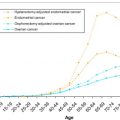
Cervical cancer affects a significant number of reproductive age women, with 40% of cervical cancer cases diagnosed less than the age of 45 years. Younger women are diagnosed at an earlier stage and with disease amenable to surgical treatment more often than their postmenopausal counterparts. Because many of these patients have yet to complete their childbearing, fertility-sparing options have increasingly been explored and refined. Dargent and colleagues first described the radical vaginal trachelectomy (RVT) in 1994 for fertility-sparing treatment of early cervical cancer. In combination with pelvic lymphadenectomy, it is the most common and accepted fertility-sparing option for cervical cancer, with equivalent surgical and oncologic outcomes compared with radical hysterectomy and acceptable obstetric results.
Patient selection is of particular importance to achieve successful outcomes. Candidates for RVT should undergo preoperative evaluation with magnetic resonance imaging (MRI) to assess endocervical extension in relation to the uterine isthmus. The following selection criteria are generally accepted and have remained essentially unchanged over the last 10 years :
- •
Desire and capability for future fertility
- •
Stage IA1 with LVSI, IA2, or IB1
- •
Squamous, adenocarcinoma, or adenosquamous histology
- •
Tumor limited to the cervix
- •
Tumor size ≤2 cm (2.5 cm can be considered in strictly exophytic lesions)
- •
Limited endocervical extension by MRI or intraoperative frozen section
- •
Absence of lymph node metastasis or distant metastatic spread.
The procedure entails laparoscopic pelvic lymphadenectomy with frozen section evaluation to rule out lymph node metastasis, followed by removal of the uterine cervix, parametrium, and upper vagina with preservation of the uterine fundus and adnexa. Frozen section of the superior cervical margin is obtained to assure adequate margins of 5 to 8 mm. A permanent cerclage is placed in the uterine isthmus and the vaginal cuff reapproximated to the neoectocervix. Several investigators have reported their experience with RVT for fertility preservation. When compared with radical hysterectomy, operative characteristics seem equivalent or better with regards to blood loss and hospital stay. One study reported a longer median operative time in the RVT group because of the long learning curve; however, other studies were equivalent. One of the largest series comparing RVT with laparoscopic-assisted radical vaginal hysterectomy reported comparable intraoperative complication rates of 2.5% and 5.8%, respectively. Similar results have been published in other series. The most common intraoperative complications were bladder injuries, followed by vascular injuries mainly occurring during the laparoscopic lymphadenectomy. RVT has some postoperative complications unique to this procedure including cervical stenosis, cerclage erosion, dysmenorrhea, menstrual irregularities, and hematometria.
The main concern with fertility-preserving therapy for cervical cancer is whether similar oncologic outcomes can be achieved with conservative surgery with regard to the need for adjuvant therapy, recurrence rates, and mortality. Despite careful selection, 10% to 12% of patients selected to undergo fertility-sparing surgery require adjuvant therapy. The largest series of RVT by Plante and colleagues includes 140 patients, 125 of whom successfully underwent the procedure. The procedure was abandoned in 10 patients for positive lymph nodes on frozen section, and in 5 patients for positive endocervical margins. After routine preoperative MRI was instituted, all abandoned procedures were a result of nodal metastasis rather than close endocervical margins, highlighting the usefulness of preoperative imaging for patient selection. Three patients with high-risk features on final pathology received adjuvant therapy after radical trachelectomy. This group reports favorable oncologic outcomes over a mean follow-up time of 95 months. There were 6 patients (4.8%) who developed a recurrence and 2 patients (1.6%) who died of disease for a 5-year recurrence-free survival of 96%. The only feature significantly associated with recurrence was tumor size greater than 2 cm ( P = .002). These results compare favorably with a review of more than 600 cases reporting an overall recurrence rate of 5.3% and mortality of 3.2%. Comparative studies of RVT and radical hysterectomy also show no differences in recurrence rate or 5-year overall survival. In one of these studies LVSI and depth of invasion correlated with recurrence risk, but not tumor diameter.
In addition to equivalent oncologic outcomes, Plante and colleagues also reported favorable obstetric outcomes with the largest series of pregnancies after RVT. Fifty-eight women in this series conceived a total of 106 pregnancies. Of 125 patients, 15% experienced infertility issues, 40% of which were caused by cervical stenosis. The rate of first-trimester and second-trimester losses, 20% and 3% respectively, were comparable with the general population, and 55% of pregnancies were delivered at term. The rate of significant prematurity (<32 weeks) was only 4%. In a review of more than 250 published pregnancies after RVT, Gien and colleagues report pregnancy rates of 41% to 79%, with 40% of deliveries at term and a 12% rate of significant prematurity (<32 weeks). Infertility rates ranged from 25% to 30%. Possible causes include cervical stenosis, reported to affect 15% of patients who have undergone RVT, decreased cervical mucus, surgical adhesion formation, and subclinical salpingitis. First-trimester loss rates were comparable with the general population at 16% to 20%, and second-trimester loss rates were twice that of the general population at 8% to 10% compared with 4%. This finding may reflect a propensity for ascending infection because of decreased residual cervical length leading to chorioamnionitis or midtrimester premature rupture of membranes. These pregnancies are also at increased risk of preterm delivery, with rates of 20% to 30% compared with the national average of 12.2% in 2009. The superior preterm delivery rates and second-trimester loss rates reported by Plante and colleagues have been attributed to an attempt to leave 1 cm residual cervix as long as margins are adequate. Pregnancies after radical trachelectomy are high risk and should be managed by a maternal fetal medicine specialist.
With equivalent surgical and oncologic outcomes to radical hysterectomy and acceptable reproductive outcomes, RVT has become an accepted treatment option for early-stage cervical cancer in carefully selected young women desiring fertility. Despite hundreds of reported cases, its use has not been implemented widely, perhaps because of a lack of training in radical vaginal surgery. Alternative approaches such as abdominal radical trachelectomy (ART) and robotic radical trachelectomy have been investigated. ART has a more limited experience, with just more than 100 cases reported in the literature. The abdominal approach broadens the scope of fertility-sparing surgery to include patients with restrictive vaginal anatomy or larger tumors (up to 4 cm). The procedure differs slightly in that the round ligaments are divided and the uterine vessels are sacrificed at their origin from the internal iliac vessels. Care is taken to preserve the infundibulopelvic and utero-ovarian ligaments, which provide the sole blood supply to the uterus through the ovarian vessels. The remainder of the procedure is similar to a type III radical hysterectomy. The specimen is transected from the vagina and at the desired length from the uterine isthmus, and sent for frozen section. Again, a cerclage can be placed once an adequate margin is achieved and the vaginal cuff is then reapproximated to the uterus. In 1 comparative study the abdominal approach allowed for a wider parametrial resection (3.97 cm vs 1.45 cm, P <.0001), a shorter operative time (319 minutes vs 363 minutes, P = .01), and a similar complication rate, but resulted in greater blood loss (300 mL vs 100 mL, P = .001). The largest series of 33 patients who underwent ART by Ungar and colleagues reported no recurrences over a median follow-up of 47 months, and 9% of patients needed adjuvant therapy. Another series by Abu-Rustum and colleagues reported a higher adjuvant therapy rate of 32%, but may reflect an inherently higher-risk population because larger tumors were selected for this approach.
Robotic surgery has also been used to perform this procedure with the benefit of improved precision and visualization. Robotic radical trachelectomy for fertility preservation in early cervical cancer has been reported by several investigators as feasible and safe for surgeons trained in laparoscopy and radical pelvic surgery. A series of 4 patients reported favorable surgical outcomes, with a median operative time of 339 minutes, estimated blood loss of 62 mL, and hospital stay of 1.5 days; no patient required adjuvant therapy. The fine dissection capability also allows for nerve-sparing and uterine artery preservation as a refinement in the technique and potential for improved outcomes.
Fertility preservation has been a major advancement in the treatment of cervical cancer for young women over the last decade. With comparable morbidity, recurrence, and survival, radical trachelectomy has gained widespread acceptance, and should be offered to appropriately selected women wishing to maintain reproductive options. Future directions will focus on the role of ultraconservative surgery, such as simple trachelectomy or conization for low-risk disease and the role of neoadjuvant chemotherapy to broaden patient eligibility. Further investigation is needed to improve patient selection and preoperative evaluation, define prognostic factors for adjuvant therapy, and improve management of subsequent pregnancies.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


