Figure 8.1
The upper pole is prepared and resected with ligation of the superior thyroid artery and vein
Figure 8.2
The superior parathyroid gland and the recurrent laryngeal nerve (RLN) are routinely identified
8.2.2 Mediastinal Extension
In cases of very large intrathoracic goiters, invasive tumors, dense adhesions from prior surgery, uncontrollable bleeding, or with the rare truly ectopic intrathoracic gland with its major blood supply from intrathoracic vessels, a mediastinal approach using sternotomy is required. As an alternative to complete sternotomy, a partial upper sternal split (i.e., manubriotomy) is sufficient in most cases to achieve adequate exposure. This means that only the manubrium is split downwards to the manubriosternal junction. Figure 8.3 depicts the skin incision for partial sternotomy (manubriotomy). After division of the subcutaneous layer, the fascia of the pectoral muscles is incised, and access to the sternal periosteum is freed.
The suprasternal notch is prepared and the innominate vein and the pleura are freed from the posterior surface of the manubrium. The manubrium is then divided using either sternal scissors (i.e., Schumacher’s scissors) or a sternal saw in the midline and is gently spread with a right-angled retractor (Fig. 8.4). A pediatric thoracotomy retractor is helpful in this situation. Bleeding points from the anterior and posterior sternal periosteum and from the bone are coagulated. For better visualization, the thyroid gland is rotated forward, and the esophagotracheal groove and the angle formed by the arch of the aorta and the innominate artery are carefully prepared. The RLN is then dissected off the gland. The RLN can take unusual courses owing to the growth of large goiters, so it is wise to transect the thyroid vessels after proper identification of the RLNs. Thereafter, the inferior pole vessels are divided, followed by the branches of the inferior thyroid artery, always close to the thyroid capsule. Here, the search for the lower parathyroid glands is very important. If these glands cannot be preserved at their vascular supply or doubt about their viability arises, they should be taken out, cut in small pieces, and transplanted into a formed pouch of the sternocleidomastoid muscle.
The manubriotomy or sternotomy is closed using sternal wires that are supported by strong, absorbable threads.
Large goiters with intense adhesions to the pleura or pericardium may require the excellent exposure available with a complete sternotomy. For a complete sternotomy, the skin incision is extended to just above the xiphoid process, and the pericardial and diaphragmatic attachments are freed from the back of the sternum before its division (Fig. 8.5). The following surgical dissection steps and the wound closure are similar to the description above for Fig. 8.4.
Occasionally, substernal goiters developing on the left side can cross over to the right mediastinum dorsally from the trachea, perhaps because their downward progression has been stopped by the aortic arch on the left side. For resection of this posterior mediastinal goiter, a combined approach and right anterolateral thoracotomy through the 4th or 5th intercostal space can be helpful. The patient is placed in a 45° oblique position with the right arm extended over the head (Fig. 8.6). This approach permits simultaneous cervical and thoracic exploration, and the table may be rotated from side to side to facilitate whichever part of the dissection is being performed.
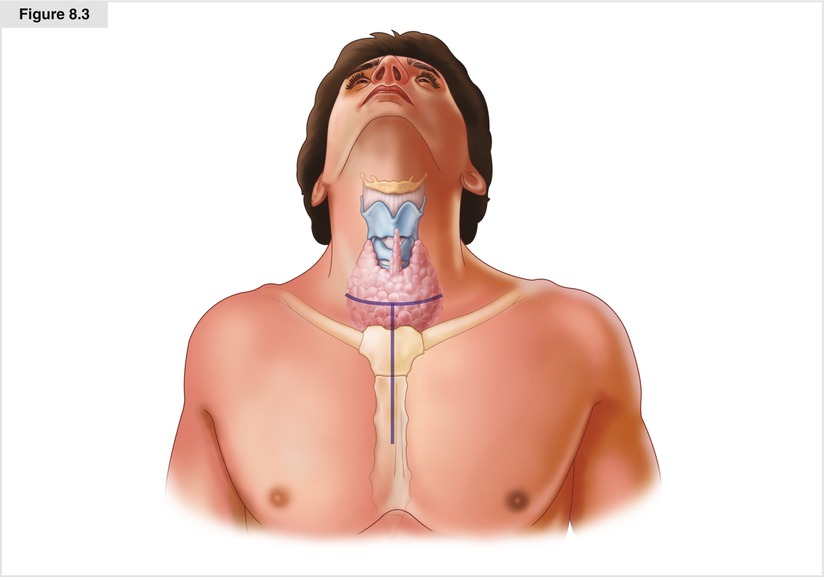
Figure 8.3
 Thyroid Lobectomy and Total Thyroidectomy
Thyroid Lobectomy and Total Thyroidectomy
 Mediastinal/Thoracoscopic Parathyroidectomy
Mediastinal/Thoracoscopic Parathyroidectomy
 Posterior Retroperitoneoscopic Adrenalectomy
Posterior Retroperitoneoscopic Adrenalectomy
 Small Bowel Resection and Lymphadenectomy for Jejunoileal Neuroendocrine Tumors
Small Bowel Resection and Lymphadenectomy for Jejunoileal Neuroendocrine Tumors
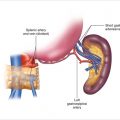 Laparoscopic Distal Pancreatectomy
Laparoscopic Distal Pancreatectomy
 Subtotal Parathyroidectomy for Parathyroid Hyperplasia
Subtotal Parathyroidectomy for Parathyroid Hyperplasia




The skin incision for manubriotomy (partial sternotomy)
Related posts:
Thyroid Lobectomy and Total Thyroidectomy
Mediastinal/Thoracoscopic Parathyroidectomy
Posterior Retroperitoneoscopic Adrenalectomy
Small Bowel Resection and Lymphadenectomy for Jejunoileal Neuroendocrine Tumors
Laparoscopic Distal Pancreatectomy
Subtotal Parathyroidectomy for Parathyroid Hyperplasia
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
