Fig. 18.1
Robotic stereotactic body radiotherapy unit (Courtesy of Hacettepe University)
We do not recommend rSBRT in patients with collagen vascular disease and inflammatory bowel disease. We can treat patients with metal in the pelvis, which consists of artificial hips, since the delivery of multiple small beamlets can find appropriate alternative pathways.
18.5.2 Fiducial Placement
Once the patient is a candidate for rSBRT, the patient is scheduled for his fiducial placement and simulation. We used specific four golden fiducials manufactured to be used with CyberKnife® (Fig. 18.2). Prophylactic antibiotic and urinary antiseptics are given prior to procedure.
Fig. 18.2
Golden fiducials for CyberKnife
At our institution, the fiducials are inserted transrectally under ultrasound guidance by the urologist under local anesthesia (Fig. 18.3). We also try to place the fiducials in certain regions of the prostate gland due to the fact that all fiducials should be in certain geometry accordingly with the imaging X-ray tubes (Fig. 18.4). Once the fiducials have been placed, there should be 7–10 days before the simulation is done.
Fig. 18.3
Transrectal fiducial placement for rSBRT
Fig. 18.4
Locations for the fiducial placement within the prostate gland
18.5.3 Simulation
For the simulation, we place the patient in a supine position and place a 14 Gauge Foley catheter into the bladder to visualize prostatic urethra (Fig. 18.5). We then inflate its balloon with 6 cc of water. Once the Foley is placed, a non-contrast planning CT with less than 1 mm slice thickness is performed to the entire pelvis.
Fig. 18.5
14 G Foley catheter visualized within the prostatic urethra. Sample plan is showing hot points within the urethra that is not acceptable
18.5.4 Contouring
At our institution, the CTV for definitive prostate cancer patients is as per the following: prostate only for low risk; prostate proximal seminal vesicles (SV) for intermediate risk. Proximal is defined as the proximal 1 cm of the SV.
18.5.5 Dosing
The standard dose is 36.5 Gy in 7.3 Gy daily fractions either in consecutive (Monday–Friday) or every-other-day regimen (2 weeks regimen) (Fig. 18.6).
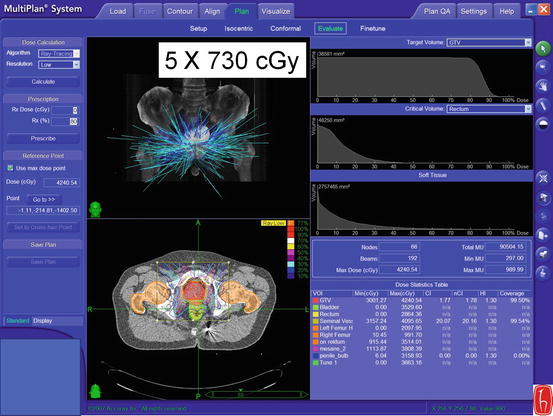
Fig. 18.6
Treatment plan of a patient receiving rSBRT with every-other-day protocol
18.5.6 Plan Evaluation
Our rSBRT treatment plan acceptance criteria are summarized as following:
PTV
PTV prescribed dose: 7.3 Gy in five fractions with a total dose of 36.5 Gy.
Inhomogeneities. 110–130% high-dose region within CTV if possible within GTV.
Maximum dose < 45.5 Gy.
Ninety-five percent volume of PTV should receive 36.25 Gy.
Minimum PTV dose 34.4 Gy.
Rectum
V33.5 Gy < 1 cc.
Minor variation: V33.5 Gy ≥ 1 cc but <3 cc.
Major variation: V33.5 Gy ≥ 3 cc.
Max dose (0.03 cc) ≤ 38.06 Gy.
Less than 3 cc volume may receive 34.4 Gy.
V32.6 Gy ≤ 90% rectum.
V29 Gy ≤ 80% rectum.
V18.125 Gy ≤ 50% rectum.
Bladder
V35 Gy < 5 cc
Minor variation: V35Gy ≥ 5 cc but <10 cc
Major variation: V35 Gy ≥ 10 cc
Max point dose (0.03 cc) ≤ 38.06 Gy
V32.625 Gy ≤ 90% bladder
V18.125 Gy ≤ 50% bladder
Urethra
V45.5 Gy < 10%
Minor variation: V45.5 Gy ≥ 10% but <20%
Major variation: V45.5 Gy ≥ 20%
Max Doz < 38.78 Gy
Penile Bulb
V27.5 Gy ≤ 50%.
Minor variation: V27.5 Gy ≥ 50% ama <70%.
Major variation: V27.5 Gy ≥ 70%.
Max dose does not exceed the prescribed dose.
V20 Gy < 3 cc.
Femur
V20 Gy < 10 ccRelated posts:
 Quality Assurance of Modern Radiotherapy Techniques in Prostate Cancer Treatment
Quality Assurance of Modern Radiotherapy Techniques in Prostate Cancer Treatment
 Guidelines for the Delineation of Lymphatic Target Volumes in Prostate Cancer
Guidelines for the Delineation of Lymphatic Target Volumes in Prostate Cancer
 Prostate Cancer Risk Grouping and Selection Criteria Based on Radiation Oncology Perspective
Prostate Cancer Risk Grouping and Selection Criteria Based on Radiation Oncology Perspective
 Proton Therapy for the Treatment of Prostate Cancer
Proton Therapy for the Treatment of Prostate Cancer
 Functional Imaging-Guided Radiotherapy and Radiolabelled Targeted Therapies in Prostate Cancer
Functional Imaging-Guided Radiotherapy and Radiolabelled Targeted Therapies in Prostate Cancer
 Histopathological Evaluation in Prostate Cancer
Histopathological Evaluation in Prostate Cancer

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


