Cancer of the oral cavity represents ˜30% of all cancers of the head and neck. Squamous cell carcinoma (SCC) constitutes 90% of all oral malignancies whereas the remaining 10% include cancer arising in minor salivary glands, and odontogenic cancers, and sarcomas.1 The incidence of oral carcinoma is ˜6 cancers per 100,000 in Americans with a male-to-female ratio of 2.2:1. In North America, this represents ˜1.4% of all new malignancies and 0.6% of all cancer-related mortality. Based on the most recent Surveillance, Epidemiology, and End Results (SEER) Program of the National Cancer Institute data, the overall 5-year survival for cancer of the oral cavity is 62.2% (2003 to 2009) compared to 53% two decades earlier (1975 to 1979). The average age of diagnosis is 60 years and the vast majority of patients (>95%) are older than 40 years (http://seer.cancer.gov). Although these data are important, they can be misleading because the cancer of the oral cavity encompasses diverse anatomy from the lips to the tonsillar pillars. Although the lips and the oral tongue are anatomically close, cancer in these regions of the oral cavity may behave differently. For example, carcinoma of the lip behaves very differently from carcinoma of the lateral tongue; and carcinoma of the lateral tongue behaves differently from cancers of the hard palate. The lip, the tongue, and the hard palate are anatomically included within the oral cavity site, yet malignancy in each of these subsites behaves very differently. This must be considered as one interprets the data because the majority of data are the results of studies inclusive of patients across the various oral cavity subsites.
ETIOLOGY
The risk factors for developing SCC of the oral cavity in North America and Europe are tobacco and alcohol consumption. Independently, they are associated with a dose-dependent risk of developing oral SCC. Cigarettes contain over 60 carcinogens.2 Despite a decline in the rate of cigarette smoking since the release of the first US Surgeon General’s Report on Smoking and Health in 1964, 21.6% of men and 16.5% of women continue to use tobacco; ˜80% of tobacco users are daily smokers.
Alcohol is another common carcinogen contributing to mucosal irritation and increased cell permeability. Excessive alcohol consumption is associated with vitamin and nutritional deficiencies, which independently contribute to oral carcinogenesis. Combined, these toxins have synergistic effects and translate to a relative risk of developing oral SCC of between 7.2 and 35.3,4,5 Smokeless tobacco is associated with a twofold increased risk of oral SCC, is estimated to be used by 6% of the US adult male population, and is significantly more common in the southern United States where the rate raises to 30%.6 In areas where chewing betel or areca nut is more commonplace, such as South Asia, this behavior is associated with a sevenfold increased risk of developing oral SCC.7 The practice of reverse smoking, commonly practiced in India, further contributes to an increased rate of oral cavity SCC, which constitutes an impressive 25% of all cancers in that region.8 Less well-studied risk factors include poor oral hygiene and ill-fitting dentures; however, these conditions have both been recognized as independent risk factors. The proposed etiology is that mechanical irritation produces a cascade of inflammatory mediators that contribute to the development of dysplasia and carcinoma.9
Over the past three decades, there has been a rise in human papillomavirus (HPV)-associated cancer of the oropharynx, oropharyngeal squamous cell carcinoma (OPSCC).10 It is suggested that this trend may correspond with changing sexual behaviors and is consistent with the mode of transmission of HPV and the relative increased rate in males versus females.11 The correlation between HPV and cancer of the oral cavity is less clear. Some reports demonstrate that up to 24% of oral cavity carcinomas are associated with HPV; however, most literature suggests a significantly lower association.12,13 There remains a significant proportion of oral squamous cell carcinoma (OSCC) that cannot be attributed to the traditional risk factors of tobacco or alcohol use, particularly among women and young patients.5 Recent epidemiologic studies have identified an increasing incidence of SCC of the oral tongue in younger patients and found that gene-specific mutation and copy number alteration frequencies were similar between young and old patients. This observation supports the recent developments illucidating the significant role that genetic instability and genetic susceptibility play in the etiology of oral SCC and the poorly understood functional impact of smoking on carcinogenesis.14,15,16
ANATOMY
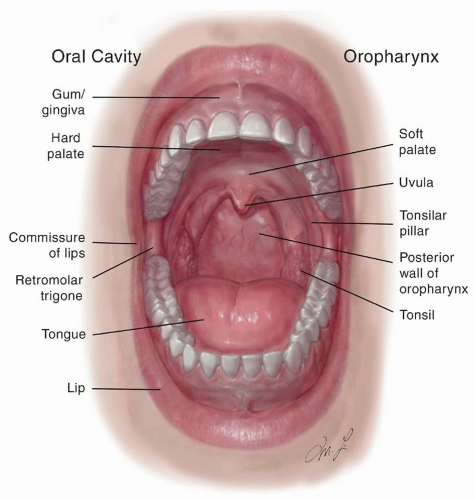
The anterior border of the oral cavity is at the junction of the skin and vermilion border of the lip.16,17 Posteriorly, the oral cavity is limited by the junction of the hard and soft palates superiorly and the circumvallate papilla inferiorly. The anterior tonsillar pillars define the posterior lateral aspects of the oral cavity. The oral cavity is composed of the oral cavity gingiva, lip, hard palate, oral tongue, floor of the mouth, retromolar trigone, and buccal mucosa (Fig. 13.1). In addition, the underlying mandible and maxilla are often included in the anatomy of the oral cavity. The oral cavity is lined by squamous cell epithelium populated by minor salivary glands. Although minor salivary glands can be demonstrated throughout the mucosa of the oral cavity, they are most concentrated within the hard and soft palate. For this reason, minor salivary gland tumors exist most commonly within these sites in the oral cavity.
Figure 13.1. Anatomy of the oral cavity. The anterior border of the oral cavity is at the junction of the skin and vermilion border of the lip. Posteriorly, the oral cavity is limited by the junction of the hard and soft palates superiorly and the circumvallate papilla inferiorly. The anterior tonsillar pillars define the posterior lateral aspects of the oral cavity. The oral cavity is composed of the oral cavity gingiva, the lip, the hard palate, the oral tongue, the floor of the mouth, the retromolar trigone, and the buccal mucosa.
In addition, the mandibular and maxillary alveoli are included in the oral cavity. The retromolar trigone, which is an area located in the posterior oral cavity posterior to the last mandible tooth, is a common site for cancer of the oral cavity. The overlying periosteum is particularly thin in the area of the retromolar trigone, making invasion of the cortex a common occurrence. The floor of the mouth extends from the inner margin of the inferior alveolus to the ventral surface of the oral tongue. The structures of the floor of the mouth are supported by mylohyoid, geniohyoid, and genioglossus musculature. These muscles insert along the mylohyoid line found on the medial aspect of the mandible. The sublingual structures lie cranial to the mylohyoid line, whereas the submandibular structures lie below the mylohyoid line. The oral tongue located within the floor of the mouth is lined with squamous epithelium and fungiform, filiform, and circumvallate papilla. The intrinsic muscles responsible for swallowing and the articulation of speech generate the complex movement of the tongue. Several branches of the external carotid artery, including the facial and lingual arteries, provide the blood supply of the oral cavity structures.
The pattern of lymphatic drainage of the oral cavity has been well established in the literature.18,19,20 The presence of cervical lymph node metastasis has been repeatedly correlated with the size, depth of invasion, location, and the degree of differentiation of the primary tumor. In general, the frequency of lymph node metastasis increases with the size and depth of penetration of the lesion. Additionally, the more posteriorly a primary is located, the higher the risk of lymphatic spread to lower echelon nodal basins (level III to IV). The lymphatic spread of oral SCC generally occurs in an orderly manner, involving first levels I to II, followed by levels II to III, and finally the inferior cervical lymph nodes, level IV. However, “skip” metastases have been reported, wherein metastatic spread from oral cavity structures to lymph nodes in level IV of the neck can occur in the absence of nodal involvement in levels I, II, and III.
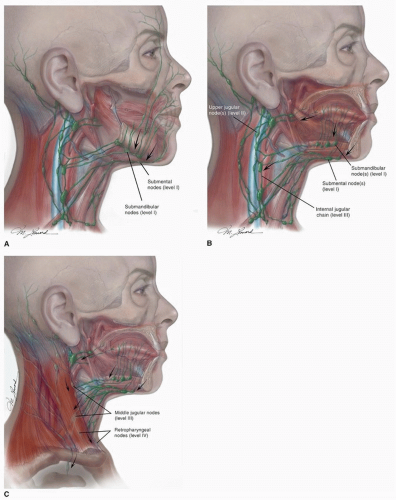
The pattern of lymphatic spread often follows the vascular territory of the region in which the primary cancer is located. The lip, cheek, and anterior gingiva drain to submandibular and submental lymph node basins (level I to II) and occasionally the inferior parotid nodal basin (Fig. 13.2A-C). The posterior gingiva and palate drain to the internal jugular chain and lateral retropharyngeal nodes (level II to IV). Lymphatic drainage for the tongue and floor of the mouth includes the internal jugular, subdigastric, omohyoid, submandibular, and submental nodal basins (level I to III). The deep lymphatic network for the oral tongue consists of anterior, lateral, and central lymphatic pathways. The anterior pathway drains the tip of the oral tongue and primarily drains to level III (or less commonly level I to II). The lateral group drains the lateral one-third of the dorsum of the tongue from the tip to the circumvallate papillae to submandibular, and internal jugular nodal basins and occasionally the submental node basin (level I to III). The central pathway drains the central two-thirds of the tongue. These vessels drain to the submental region (level I) or the upper cervical chain nodal basin via the sublingual nodes (level III).21 Primary cancers, which approach midline, often drain to bilateral nodal basins. This is especially true for cancers of the tongue and floor of the mouth as there exists significant lymphatic crossover in this region.22,23
Figure 13.2. A-C: The lymphatic spread of oral SCC generally occurs in an orderly manner, involving first levels I to II, followed by levels II to III, and finally the lower cervical lymph nodes, level IV. The pattern of lymphatic spread often follows the vascular territory of the region in which the primary tumor is located. The anterior pathway drains the tip of the oral tongue and primarily drains to level III (or less commonly levels I to II). The lateral group drains the lateral one-third of the dorsum of the tongue from the tip to the circumvallate papillae to submandibular, and internal jugular nodal basins and occasionally the submental node basin (level I to III).
Premalignant Lesions of the Oral Cavity
Unlike other head and neck sites, the oral cavity can be easily examined and is therefore amenable to screening protocols to identify early cancers. Awareness of the common signs and symptoms of premalignant and malignant oral lesions is paramount to the early detection and recognition of these lesions. Pain is the presenting symptom in 50% to 60% of malignant lesions and should therefore prompt further evaluation with a biopsy, excision, or close follow-up, especially in the setting of pain that persists.24 Patients with symptomatic lesions often present to primary care physician or dental health professional. In contrast, asymptomatic lesions can grow undetected. This underscores the importance of screening. The American Dental Association has enacted a screening program that has proven successful in identifying oral premalignancies and early cancers.
It is often difficult to differentiate premalignant lesions from early invasive cancers. Invasive SCC often develops as a result of an evolution of molecular transformations in suppressor and/or promoter genes.24 The evolution, however, does not always follow a prescribed pathway resulting in an invasive carcinoma. Premalignant lesions of the oral cavity may be detected at any point in this progression. Some may be actively progressing toward malignancy, whereas others may remain in a state of abeyance, neither progressing nor regressing. Suspicious findings on examination include a nonhealing or indurated ulcer or a mucosal lesion with a palpable firm mass.
Leukoplakia
Leukoplakia is a descriptive term, not a pathologic diagnosis. This descriptive terminology refers to white patches on the mucosal surface that histologically correlate with hyperkeratosis, acanthosis, and inflammatory cell changes. These changes may be premalignant or associated with atypia. Tobacco is the most commonly associated risk factor for developing leukoplakia. In a large case series of clinically diagnosed leukoplakia reviewed microscopically, only 7.6% had severe dysplasia or invasive carcinoma.25 Over a 10-year period, leukoplakia has been reported to progress to carcinoma in 0.9% to 17% of cases.26 Leukoplakia may also occur without a preexisting environmental exposure. In either case, the presence of leukoplakia often warrants a biopsy, with smaller lesions undergoing an excisional biopsy. Some suggest observation of a small confluent leukoplakia lesion if there is no evidence of progression, ulceration, or change in character. Some tobacco-related keratosis present as a very thin confluent white patch over the mucosal surface in direct contact with the tobacco. These lesions are less suspicious for transformation with cessation of tobacco use. They should be followed up closely with biopsy reserved for transforming lesions.
Erythroplakia
Erythroplakia, defined as a flat red patch, is a more concerning lesion than leukoplakia and is more likely associated with atypia or progression to carcinoma. The homogeneous type of oral erythroplakia has been correlated with a 51% rate of invasive carcinoma and a 40% rate of carcinoma in situ.27 Therefore, these lesions should be promptly biopsied and appropriately managed. Erythroplakia may present as an isolated lesion or in the presence of leukoplakia. In some cases, leukoplakia may progress to erythroplakia as the lesion develops into an invasive carcinoma.
Submucosal Fibrosis
Oral submucosal fibrosis is a chronic condition with premalignant potential that predominately affects patients from Southeast Asia with a significant history of betel quid chewing. Histologically, submucosal collagen deposition and fibrotic bands characterize submucosal fibrosis. This translates clinically to thickened and keratotic bands that restrict the pliability and flexibility of the buccal mucosa. For these reasons, the buccal mucosa becomes thickened and tight and the patients develop trismus. These lesions should be closely monitored for the development of oral cavity SCC.28
CLINICAL PRESENTATION OF CANCER OF THE ORAL CAVITY MALIGNANCY
The presentation of cancers of the oral cavity may vary depending upon the histology and the location. Cancers may present as an ulcerative lesion, as a raised exophytic lesion, or as an irregular mucosal mass. Not uncommonly, ulcerative lesions may present as a subtle lesion on the surface; however, on further inspection and palpation, the lesion may extend deep into the soft tissue. For this reason, palpation is a key part of the examination. Similarly, cancers of the alveolus may present as an irregular patch of mucosa adjacent to a tooth socket. Peridental cancers may present as a limited lesion on the surface of the mucosa, yet they may extend deep into the tooth socket and mandibular canal. In contrast, exophytic lesions may present as a papillomatous mass often described as “cauliflower-like” growth. Although benign lesions may present in a similar fashion, bleeding or ulceration suggests malignancy.
Cancer of the oral cavity may present as a painful lesion; however, the presentation may be variable. Because cancers in this region are exposed to saliva, contamination with commensal and pathogenic organisms commonly leads to infection and pain. In contrast, if a malignant lesion erodes into sensory nerves, that is, the lingual or alveolar nerves, the patient may present with anesthesia or hypesthesia of the lip or oral cavity. Finally, when a patient presents with complaints of trismus, invasion of the pterygoid space must be assumed until proven otherwise. Although infection and inflammation may also result in trismus, invasion of the pterygoid muscular by carcinoma defines advanced local involvement.
Prognostic Indicators
The prognosis of oral cavity cancer is predicated on a variety of factors including stage, depth of invasion, and the presence of neural and vascular invasion. Other prognosticators include the histologic findings including an infiltrating pattern, minimal lymphocytic response, and the presence of tumor emboli. The American Joint Committee on Cancer (AJCC) tumor, node, and metastases (TNM) staging system for oral cavity (Table 13.1) accounts for some of these factors but not all of them. All patients evaluated for cancer of the head and neck should be staged according to the AJCC system because the staging system is designed to predict the patient’s prognostic based on their TNM status and also to provide a uniform platform to develop treatment strategies and compare results. It does not, however, account for all of the important histologic characteristics that may portend the biologic behavior of a cancer. The location of a cancer is another predictor of behavior, and this is often overlooked. Locoregional recurrence rates are highest in the buccal mucosa (75%), followed by the sinopalatal region (50%) and the mobile tongue (27%).29 Although all of these subsites are a part of the oral cavity, cancers in each subsite behaves differently. To account for many of the factors not included in the AJCC system, other staging systems have been proposed in order to improve accuracy, but they have failed to gain general acceptance.30
Tumor more than 2 cm but not more than 4 cm in greatest dimension
T3
Tumor more than 4 cm in greatest dimension
T4
(Lip) Tumor invades through cortical bone, inferior alveolar nerve, floor of mouth, or skin of face, that is, chin or nose
T4a
(Oral cavity) Tumor invades through cortical bone, into deep (extrinsic) muscle of tongue (genioglossus, hyoglossus, palatoglossus, and styloglossus), maxillary sinus, or skin of face
T4b
Tumor involves masticator space, pterygoid plates, or skull base and/or encases internal carotid artery
Regional Lymph Nodes (N)
NX
Regional lymph nodes cannot be assessed
N0
No regional lymph node metastasis
N1
Metastasis in a single ipsilateral lymph node, 3 cm or less in greatest dimension
N2
Metastasis in a single ipsilateral lymph node, more than 3 cm but not more than 6 cm in greatest dimension, or in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension
N2a
Metastasis in single ipsilateral lymph node more than 3 cm but not more than 6 cm in greatest dimension
N2b
Metastasis in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension
N2c
Metastasis in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension
N3
Metastasis in a lymph node more than 6 cm in greatest dimension
Distant Metastasis (M)
MX
Distant metastasis cannot be assessed
M0
No distant metastasis
M1
Distant metastasis
Anatomic Stage/Prognostic Groups
0
Tis
N0
M0
I
T1
N0
M0
II
T2
N0
M0
III
T3
N0
M0
T1
N1
M0
T2
N1
M0
T3
N1
M0
IVA
T4a
N0
M0
T4a
N1
M0
T1
N2
M0
T2
N2
M0
T3
N2
M0
IVB
Any
T N3
M0
T4b
Any N
M0
IVC
Any T
Any N
M1
Used with the permission of the American Joint Committee on Cancer (AJCC), Chicago, Illinois. The original source for this material is the AJCC Cancer Staging Manual, Seventh Edition (2010) published by Springer Science and Business Media LLC, www.springer.com.
Histopathology
There are a series of histopathologic features that may have significant impact on the prognosis of oral cavity carcinoma. The depth of invasion, presence of perineural invasion (PNI), and lymphocytic response are examples of histopathologic parameters that are not included in the AJCC staging system. Extracapsular spread, which is associated with a 50% reduction in survival, has a significant impact on the prognosis of a patient with cancer of the oral cavity and regional metastases.
Depth of Invasion
The depth of invasion has been shown to accurately predict the likelihood of nodal metastasis and therefore prognosis.31,32 The depth of invasion that warrants elective lymph node dissection in the neck is controversial and has been reported to be between 3 and 5 mm.22 The deeper the cancer invades, the more likely the presence of occult nodal metastases and local recurrence. Yuen et al.31 reported a retrospective review of 85 glossectomy specimens and revealed that a depth of <3 mm, 3 to 9 mm, and >9 mm is associated with a 10%, 50%, and 65% rate of regional metastases, respectively. In patients with stage I or II tongue SCC with a clinically negative neck, a depth of invasion of >4 mm has been associated with a risk ratio of 9.4 in developing cervical metastases within a 5-year period.32 Ganly et al. retrospectively reviewed a cohort of 164 early-stage oral tongue SCC in which multivariate analysis indicated that cancer thickness <4 mm versus ≥ 4 mm independently and significantly predicted regional recurrence-free survival of 94% versus 72%, respectively.33 As a result of this study and others, 4 mm has emerged as the more commonly accepted depth of invasion mandating management of the neck. However, most of these studies are retrospective. The ability to detect occult micrometastases in cervical lymph nodes is dependent on the number of histologic sections prepared from each lymph node and may be missed during routine histopathologic evaluation.34 Therefore, the data related to this topic are only as reliable as the methods used to assess the lymph nodes.
Perineural Invasion and Lymphovascular Invasion
PNI and lymphovascular invasion (LVI) are poor prognostic features also not included in the TNM staging.29,35 As a result, these features influence the need for adjuvant therapy. The presence of PNI or LVI has independently been associated with a compromise in disease-free survival; however, the addition of postoperative radiation therapy has been shown to improve survival.36
Extracapsular Spaced and Positive Margins
The presence of extracapsular space (ECS) of pathologic lymph nodes is the most significant prognostic feature and has been associated with a 50% reduction in overall survival. Despite adjuvant therapy, up to one-third of patients with ECS will experience either locoregional or distant recurrence.37,38 Similarly, positive margins after surgical excision that cannot be re-resected in a timely manner are associated with a poor prognosis. A comparative analysis of the selection criteria, clinical and pathologic risk factors, and treatment outcomes of two randomized control trials (the EORTC39,40 and RTOG trials40) was performed to determine the indications for postoperative concurrent chemoradiation therapy that would offer a survival advantage. This study determined that microscopically involved resection margins and extracapsular spread of cancer from neck nodes are the most significant prognostic factors for poor outcome. Furthermore, this study demonstrated that concurrent chemoradiotherapy offered a significant survival advantage for advanced cancer of the head and neck in the setting of ECS or microscopically positive involved surgical margins.41 Although ECS is a nonmodifiable risk factor, the presence of positive margins can potentially be avoided, and therefore, when possible, it is critical to achieve a negative surgical margin.
Only gold members can continue reading. Log In or Register to continue