and Karl Reinhard Aigner3
(1)
Department of Surgery, The University of Sydney, Mosman, NSW, Australia
(2)
The Royal Prince Alfred and Sydney Hospitals, Mosman, NSW, Australia
(3)
Department of Surgical Oncology, Medias Clinic Surgical Oncology, Burghausen, Germany
In this chapter, you will learn about:
Fibrosarcoma
Liposarcoma
Rhabdomyosarcoma
Leiomyosarcoma
Neurosarcoma
Malignant fibrous histiosarcoma (MFH)
Angiosarcoma
Synovial sarcoma (synoviosarcoma or malignant synovioma)
A sarcoma is a cancer of connective tissue such as muscle, bone, cartilage, fat, nerves, fascia, tendons and blood and lymph vessels. Hence, sarcomas can develop in any part of the body although they are not as common as carcinomas that develop from epithelial tissues such as the skin and other lining cells and glands. This is probably because there is not such a constant turnover of cells in connective tissues as in epithelial tissues.
Sarcomas are classified into two groups, soft tissue sarcomas and hard sarcomas of the bone or cartilage (osteosarcomas and chondrosarcomas). There are no known causes.
The soft tissues are those connective tissues that surround the bones of the body and include muscles, fat, fascia, nerves, tendons, blood vessels and lymphatic vessels. The majority of soft tissue tumours are not malignant – it is only when they are malignant that the term sarcoma applies. Thus, most tumours of fatty tissue are lipomas – it is only when one of these is malignant that it is called a liposarcoma. Similarly, most tumours of fibrous tissue are benign and are called fibromas, and most tumours of nerves are benign and are called neuromas. Most tumours of blood or lymph vessels are benign and are called angiomas, either haemangiomas composed of primitive blood vessels or lymphangiomas composed of primitive lymphatic vessels (Fig. 20.1).
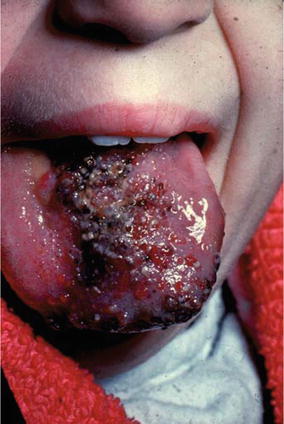
Fig. 20.1
Photograph of a large benign haemangioma of the tongue in a young woman
Soft tissue sarcomas are classified according to the type of tissue from which they arise and the type of tissue they most resemble.
The following is a list of tissues from which soft tissue sarcomas develop:
Fibrous tissue – fibrosarcoma
Fatty tissue – liposarcoma
Nerve tissue – neurosarcoma
Histiocytes (protective cells – malignant fibrous histiocytoma (MFH))
Synovial membrane lining a joint or tendon sheath – synovial sarcoma (synovioma)
Blood vessels – haemangiosarcoma
Lymphatic vessels – lymphangiosarcoma
Muscle – myosarcoma
Myosarcomas may be further classified as rhabdomyosarcoma and leiomyosarcoma. A rhabdomyosarcoma is a malignant tumour of a voluntary muscle (i.e. one of the muscles of the body over which we have control in moving arms, legs, abdomen, back, head and neck or the muscles used in breathing). A leiomyosarcoma is a malignant tumour of involuntary muscle, that is, one of the muscles over which we have no conscious control such as the muscle in the wall of the stomach or bowel or the muscles in the wall of the uterus or the wall of large blood vessels.
Soft tissue sarcomas make up only about 2 % of malignant tumours. They can occur in people of all ages from birth to old age and are relatively more common in children and young adults than are most carcinomas. Unless radically excised, sarcomas have a tendency to recur locally. Whilst most cancers tend to metastasise via the lymph vessels, to lymph nodes first, most sarcomas have a greater tendency to metastasise via blood vessels to lungs rather than to lymph nodes.
20.1 Classification: Pathological Types
20.1.1 Fibrosarcoma
These tumours develop in fascia or fibrous tissue that covers and surrounds muscles, nerves and other tissues and is distributed widely throughout the body. Thus, a fibrosarcoma may develop almost anywhere in the body especially in a limb or in the tissues of the trunk. One very fibrous and slowly growing type of fibrosarcoma, called a desmoid tumour, has a tendency to grow into nearby tissues and to recur locally after surgical excision but rarely metastasises to other organs. Other more cellular and less fibrous types have a greater tendency to metastasise.
20.1.2 Liposarcoma
These tumours develop from fatty tissue and may arise in any tissue or organ where fat is present. They tend to vary from a low-grade malignancy likely to recur locally after excision but unlikely to metastasise to a high-grade malignancy in which both local recurrence and metastatic spread to lungs are common. As a rule, the deeper they are (sometimes they are deep in muscle tissue) and the larger they have become, the more likely they are to be a higher grade of malignancy (Fig. 20.2).

Fig. 20.2
A large liposarcoma of shoulder region in a 73-year-old man
20.1.3 Rhabdomyosarcoma
This tumour presents most commonly in infants and young children as a swelling in voluntary muscle, especially in muscles of the head and neck, genitourinary tract, thorax and limbs. It is the sarcoma most likely to metastasise to lymph nodes although it does metastasise to lungs (Fig. 20.3).