Highlights
- •
The overall survival rate for patients undergoing PC-RPLND with resection of the aorta, IVC, and/or iliac artery is 45% at 2 years.
- •
Among 41 men undergoing complex PC-RPLND with replacement of major vasculature, the overall complication rate was 56%, with a 24% rate of Clavien–Dindo III/IV complications, and 2 postoperative mortalities.
- •
Reoperative PC-RPLND patients had significantly worse survival compared to initial attempt at PC-RPLND (9.3 vs. 162 months, P = 0.03).
- •
For patients with limited treatment options, these complex surgeries may offer survival benefit with an acceptable morbidity profile.
ABSTRACT
Background and objective
For patients with metastatic testicular cancer undergoing retroperitoneal lymph node dissection (RPLND), the burden of metastatic disease can require consideration for resection and replacement of major vessels despite chemotherapy. We aimed to clarify the outcomes for patients undergoing these major vascular procedures in a modern era.
Methods
Between 2000 and 2020, 2,054 patients with metastatic testicular cancer underwent a PC-RPLND; of those men, 41 also underwent an aortic, iliac, and/or inferior vena cava (IVC) resection. For men who required a vascular resection, clinicopathologic and operative details were collected. Kaplan–Meier curves were generated to estimate overall survival.
Results
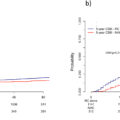
The median preoperative mass size was 9cm in the retroperitoneum. Viable malignancy or teratoma was present in 85% of resected specimens. Following PC-RPLND and vascular resection, 22 (54%) patients recurred. The median (IQR) time to relapse was 4.6 (2.5–8.0) months. 18 (44%) patients died of disease. The overall complication rate was 56%. Ten (24%) patients had Clavien–Dindo III/IV complications, with 2 postoperative mortalities. The median overall survival was 14.9 months. Among the 41 patients, 18 patients had re-operative PC-RPLND and vascular resection; the re-operative PC-RPLND patients had significantly worse survival compared to initial attempt at PC-RPLND (9.3 vs. 162 months, P = 0.03).
Conclusions
The overall survival rate for patients undergoing PC-RPLND with resection of the aorta, IVC, and/or iliac artery is 45% at 2 years. For patients with limited treatment options, these complex surgeries may offer survival benefit with an acceptable morbidity profile.
1
Introduction
In 2023, 9,190 men were estimated to be diagnosed with testicular cancer in the United States [ ]. Fortunately, testicular cancer has a greater than 95% five-year survival rate [ ], and remains a model cancer for multidisciplinary management to help generate cures in patients with metastatic disease [ ]. Testicular cancer metastases typically occur in the retroperitoneum, following well-defined lymphatic drainage patterns [ , ]. For men with bulky retroperitoneal metastasis, or rising tumor markers after orchiectomy, chemotherapy is recommended to eradicate disease, with well-documented efficacy [ ]. Unfortunately, 30% of men following first-line chemotherapy will have persistent or progressive retroperitoneal disease on imaging, or relapse with rising serum tumor markers, reflecting active malignancy, teratoma, or necrosis/fibrosis [ ]. Postchemotherapy RPLND (PC-RPLND) is indicated in the setting of new or persistent retroperitoneal adenopathy >1cm in size [ , ].
Patients with bulky metastatic testicular cancer may present with massive retroperitoneal or pelvic disease that encompasses the aorta, inferior vena cava (IVC), or iliac vessels. Initial and subsequent treatment options, including induction and salvage chemotherapy, may not be able to fully control the metastatic disease process. Some of these patients, including those with late relapse, are recognized to have poor responses to chemotherapy, limiting their therapeutic options to surgery [ ]. Thus, the only option for cure in some of these patients is PC-RPLND with resection or replacement of the aorta, IVC, or iliac arteries. Our group has previously reported on this patient population from the 1970s to 1990s [ ], however, limited recent data has been reported to understand the value of this approach in a more contemporary cohort of patients.
For this retrospective cohort study, we sought to evaluate the outcomes and complications of patients with metastatic testicular cancer from 2000 to 2020 who had significant retroperitoneal disease requiring a PC-RPLND with aortic, iliac, or caval resection and/or replacement. We hypothesized that this procedure would yield reasonable cure rates with acceptable levels of postoperative complications to warrant the indication for surgery.
2
Patients and Methods
2.1
Patients and baseline characteristics
With institutional review board approval, the prospectively maintained Indiana University testicular cancer database was queried. We identified 2,054 patients from 2000 to 2020 with metastatic testicular cancer that underwent an PC-RPLND at our institution. Of these, 41 men simultaneously underwent a vascular resection of the aorta, iliac vessels, and/or IVC. 17 of these cases (41%) were performed between 2000-2005; 6 (15%) between 2006-2010; 7 (17%) between 2011-2015; and 11 (27%) between 2016-2020.
2.2
Surgical management
The category of PC-RPLND was defined by type and number of prior treatments in addition to disease status. All patients were classified as at least having a salvage RPLND which was defined as an operation that is performed while a mass is growing or enlarging following salvage chemotherapy with normalized tumor markers. We defined elevated serum tumor markers as alpha-fetoprotein (AFP) > 25 ng/mL, and human chorionic gonadotropin (HCG) > 5 mIU/mL. Desperation RPLND was defined as PC-RPLND, following induction or salvage chemotherapy, performed in the setting of elevated or rising serum tumor markers [ ]. A late relapse was defined as a recurrence that appears more than 2 years after complete remission [ ].
2.3
Patient outcomes
Short- and long-term postoperative complications were documented retrospectively using the modified Clavien–Dindo Classification [ ]. Short-term and long-term complications were defined as complications occurring <SPAN role=presentation tabIndex=0 id=MathJax-Element-1-Frame class=MathJax style="POSITION: relative" data-mathml='≤’>≤≤
≤
30 days and > 90 days postoperatively. For patients with disease relapse, date of relapse was the first documentation of any of the following: increase in serum tumor markers, progression of disease on imaging, or date of biopsy in which disease recurrence was identified.
2.4
Statistical analysis
Overall survival was calculated using the Kaplan–Meier method for all 41 men. Subgroup survival analyses were decided a priori for patients who had the vascular graft or resection at the time of their first PC-RPLND, versus those who presented for a reoperative PC-RPLND. The log rank test was used to determine differences between groups using MATLAB R2022b and Stata IC 15.1 (Stata, College Station, TX). A P -value <0.05 was considered significant.
3
Results
3.1
Patient race/ethnicity and clinical stage
41 patients were included in the final analysis. The clinical and sociodemographic characteristics are reported in Table 1 . At the initial presentation of testicular cancer or primary retroperitoneal germ cell tumor, 27% were in stage I, 37% were stage II, 34% were stage III, and 2% were missing clinical stage.
| Characteristic | N | % |
|---|---|---|
| Race/Ethnicity | ||
| White, non-Hispanic | 38 | 93% |
| African American, non-Hispanic | 2 | 5% |
| Hispanic | 1 | 2% |
| IGCCCCG Risk Classification a | ||
| Good Prognosis | 24 | |
| Intermediate Prognosis | 13 | |
| Poor Prognosis | 3 | |
| Clinical Stage at Initial Presentation | ||
| I | 11 | 27% |
| II | 15 | 37% |
| III | 14 | 34% |
| Missing Clinical Stage | 1 | 2% |
| Site of Primary Tumor | ||
| Left Testis | 15 | 37% |
| Right Testis | 23 | 56% |
| Unknown Testis | 1 | 2% |
| Retroperitoneum | 2 | 5% |
| Orchiectomy Pathology | ||
| Missing Pathology | 4 | 10% |
| Sertoli Cell Tumor | 2 | 5% |
| Embryonal rhabdomyosarcoma | 1 b | 2% |
| Pure Seminoma | 8 | 20% |
| NSGCT: | 27 | 66% |
| Unknown | 6 | |
| Embryonal Carcinoma | 18 | |
| Yolk Sac Tumor | 9 | |
| Teratoma | 9 | |
| Choriocarcinoma | 1 | |
| Elevated Markers | ||
| AFP | 15 | 37% |
| HCG | 5 | 12% |
| Preoperative Pelvic Mass Size (cm), Median, [Range] | 19 | [17.4, 21] |
| Number of Pelvic Mass Patients | 2 | 5% |
| Preoperative RP Mass Size (cm), Median, [Range] | 9 | [2.6, 18.4] |
| Number of RP Mass Patients | 39 | 95% |
| < 2 cm | 0 | 0% |
| 2–5 cm | 2 | 5% |
| 5–10 cm | 26 | 63% |
| > 10 cm | 11 | 27% |
| Age, Median, (IQR) | 40 | (32–48) |
| Length of Hospital Stay (Days), Median, (IQR) | 7 | (5–10) |
| Late Relapse | 21 | 51% |
| Desperation RPLND | ||
| Prior RPLND | 19 | 46% |
| Yes | 18 | 44% |
| No | 23 | 56% |
a 40 patients listed in IGCCCCG risk due to 1 patient having a sex cord stromal tumor.
b The patient had orchiectomy pathology of NSGCT and embryonal rhabdomyosarcoma.
3.2
Primary tumor and pathology
The site of primary tumor was the testis in 38 (93%) patients. The orchiectomy pathology prior to PC-RPLND and vascular reconstruction consisted of 2 (5%) with Sertoli cell tumors, 8 (20%) with pure seminoma, and 27 (66%) with nonseminomatous germ-cell tumor (NSGCT).
3.3
Patient characteristics and preoperative treatment
At the time of PC-RPLND and vascular procedure, 39 patients had metastasis to the RP, with 37 (90%) having a preoperative RP mass size ≥ 5 cm (Range: 2.6-18.4 cm). Two patients had disease limited to the pelvis after previous RPLND. Both had preoperative pelvic masses > 10 cm (17.4-21 cm). Each of these patients had resection and replacement of iliac vasculature only. Twenty-one patients were considered a late relapse with a median late relapse of 12 years (IQR: 8-17 years). Nineteen (46%) patients had elevated markers at the time of surgery and thus would be considered to have had desperation surgery. Additionally, 18 (44%) patients had undergone a prior PC-RPLND before reoperative PC-RPLND with vascular resection and/or reconstruction at our institution. The median age of patients at surgery was 40 years old, with a median length of hospital stay of 7 days (IQR: 5-10 days; Table 1 ).
3.4
Chemotherapy and radiation regimens
Of the 41 patients requiring an RPLND and vascular replacement, 39 (95%) received a first induction regimen of chemotherapy. This cohort was heavily pretreated prior to surgery. Twenty-six (63%) patients received 2nd line chemotherapy prior to surgery, with nine (22%) patients receiving 3rd line chemotherapy or radiation, and two (5%) patients receiving a 4th line regimen of chemotherapy or radiation prior to surgery.
3.5
Intraoperative complications and adjunctive procedures
During PC-RPLND with vascular replacement, 4 patients had unplanned intraoperative complications, including vascular and ureteral injuries requiring reconstruction. Overall, 23 (56%) patients required an adjunctive procedure, with nephrectomy being most common. Other adjunctive procedures constituted 5% or less of additional procedures ( Table 2 ).
Related posts:
 A systematic review of family history, race/ethnicity, and genetic risk on prostate cancer detection and outcomes: Considerations in PSA-based screening
A systematic review of family history, race/ethnicity, and genetic risk on prostate cancer detection and outcomes: Considerations in PSA-based screening
 Neoadjuvant chemotherapy before radical cystectomy in patients with organ-confined and non-organ-confined urothelial carcinoma
Neoadjuvant chemotherapy before radical cystectomy in patients with organ-confined and non-organ-confined urothelial carcinoma
 Comparison of outcomes between single-port and multiport retroperitoneal robotic partial nephrectomy
Comparison of outcomes between single-port and multiport retroperitoneal robotic partial nephrectomy
 The learning curve for transperineal MRI/TRUS fusion prostate biopsy: A prospective evaluation of a stepwise approach
The learning curve for transperineal MRI/TRUS fusion prostate biopsy: A prospective evaluation of a stepwise approach
 Testosterone recovery after androgen deprivation therapy
Testosterone recovery after androgen deprivation therapy
 Testicular cancer malpractice trends
Testicular cancer malpractice trends
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


