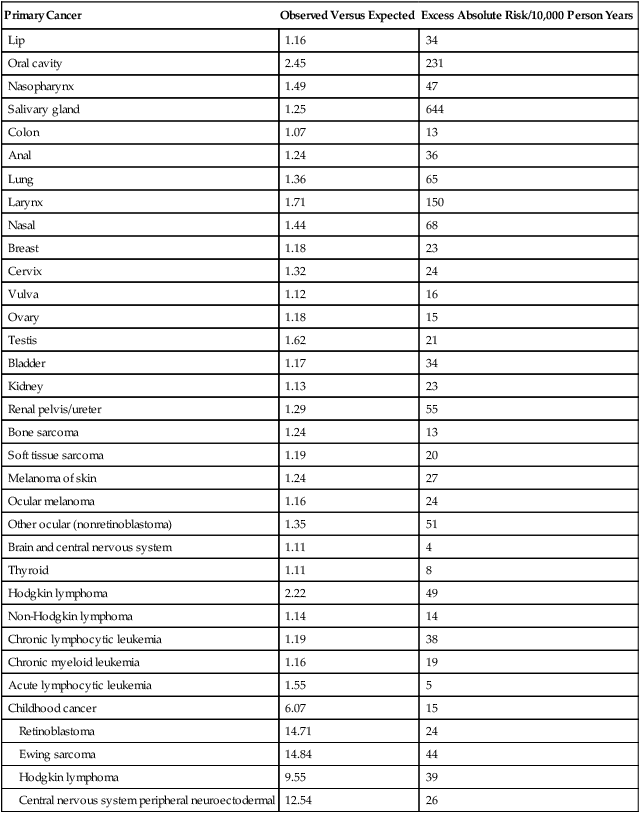
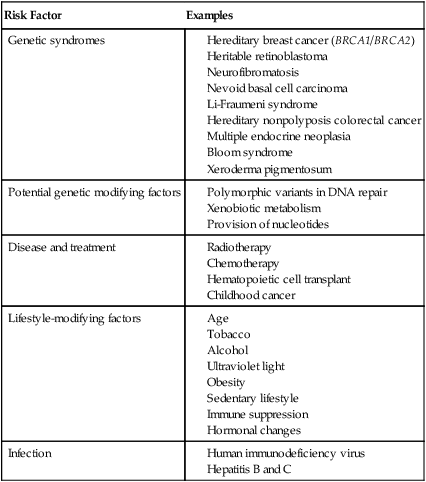
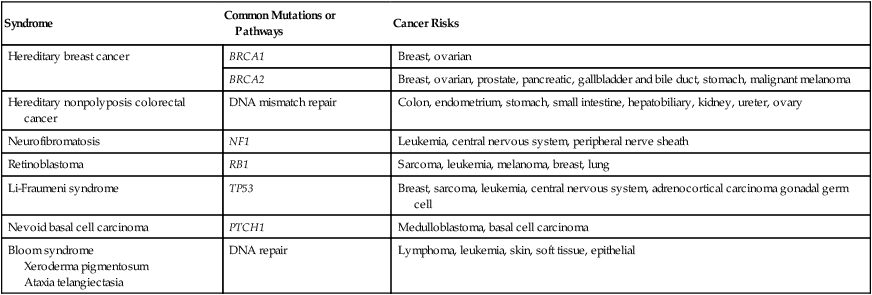
• Subsequent malignancies after successful treatment for cancer occur in a meaningful minority of persons. • Etiology is often multifactorial and includes known hereditary conditions, unrecognized genetic predisposition, primary cancer, therapeutic exposures, age, and lifestyle practices. • Guidelines for screening are available for some but not all situations; health care providers and patients should be aware of such guidelines. • Further research is needed to identify persons at highest risk so more useful preventive strategies can be developed. The American Cancer Society estimated that 1,638,910 cases of new cancer would be diagnosed in the United States in 2012, a figure that excludes cancer in situ and nonmelanoma skin cancer. In the same time period, 577,190 persons were expected to die from cancer. Because of the rising incidence of and survival from cancer, an estimated 12.8 million survivors of cancer are now alive in the United States, with 5-year survival rates of 67% for adults and 82% for children now being diagnosed with cancer, according to the National Cancer Institute (NCI) Surveillance Epidemiology and End Results (SEER). With a growing cohort of cancer survivors now living, efforts have focused on decreasing the risk for adverse long-term health-related outcomes, the most significant of which are subsequent malignant neoplasms (SMNs). According to current data from SEER, SMNs represent 16% (1 in 6) of reported cancers.1 The most recent monograph from the NCI on subsequent malignancies, published in 2006, does not reflect the current percentage because it reports on the period from 1973 to 2000,2 expanding on the prior report issued more than 20 years earlier.3 However, this monograph represents the largest overview of subsequent malignancies that includes data on both adult and pediatric cancers. In this report, among 2 million patients with cancer who survived at least 2 months with close to 11 million person-years at risk, cancer survivors had a 14% higher risk of having a new malignancy than would have been expected in the general SEER population (observed/expected = 1.14). A total of 185,407 new primary cancers were observed compared with the expected number of 162,602 which translates to an excess absolute risk (EAR) of 21 per 10,000 person-years. However, the risk of SMN compared with the general population was highly dependent on the age of the patient at first cancer diagnosis, because risk for cancer rises with increased attained age in the general population. For example, for persons younger than 18 years at initial diagnosis, the relative risk (RR) was 6.13 and the EAR was 15 per 10,000 person-years. The RR and EAR for persons 70 to 79 years at initial diagnosis dropped to their lowest values, 1.02 and 4, respectively. The highest EARs of 32 to 39 were noted in young to middle-age adults ages 30 to 59 years at initial cancer diagnosis. Gender also influenced risk, with a slightly increased risk for females (RR = 1.17) compared with males (RR = 1.11), a pattern that remained even when gender-specific malignancies were excluded from the analyses. Blacks also had elevated RR and EAR (1.31 and 46, respectively) compared with whites (1.12 and 20, respectively). Overall, an SMN developed in 14% of SEER patients by 25 years of follow-up. Although RRs were highest in the first 5 years from diagnosis, cumulative incidence increased by years of follow-up: 5.0%, 8.4%, 10.8%, and 13.7% at 5, 10, 15, and 25 years, respectively. More than 80% of multiple primary cancers reported arose in separate or independent organ systems. New malignancies that occurred in the same site or organ as the first primary cancer accounted for 13.2%, with the most common sites being the female breast, colon, lung, and skin (melanoma). Another 3.8% of new malignancies originated in neighboring tissues or organs.2 Table 62-1 shows the significant relative and excess absolute risks by primary cancer site. As is obvious, risk is highest for survivors of childhood cancer. However, for adult-onset cancers, although detailed lifestyle or environmental data were clearly not obtained for this analysis, the EAR for cancers occurring at tobacco- or alcohol-related sites, such as the oral cavity, pharynx, esophagus, larynx, and lung, was 114 cases per 10,000 person-years and overall accounted for 10,000 excess subsequent cancers.2 Table 62-1 Risk Factors for Subsequent Malignancy in the United States by Site* *Adapted from National Cancer Institute. New malignancies among cancer survivors: SEER cancer registries, 1973-2000, <http://seer.cancer.gov/publications/mpmono/>; 2013 [accessed 25.04.13]. The etiology of SMNs is multifactorial. Host and environmental factors clearly play a role, but defining those contributions can be difficult. Superimposed on this general population risk for second and subsequent primary cancers are treatment-associated malignancies, where chemotherapy and radiotherapy for the primary cancer can increase risk for a subsequent cancer. This risk is then modified by host and environmental factors that affect risk of primary cancer, such as lifestyle (e.g., use of tobacco and alcohol, sun exposure, and diet), workplace and home exposures to carcinogens, viruses, age, gender, genetics, infection, immune function, hormone levels, and interactions of all of these factors. It is difficult to evaluate disease separate from known genetic associations with those diseases (e.g., breast, colon, and retinoblastoma) or separate from exposure to specific therapeutic modalities used to treat those malignancies (e.g., chemotherapy and radiation therapy). Table 62-2 summarizes common risk factors for SMNs in these general categories, but categories are not fully exclusive of one another. Table 62-2 Potential Risk Factors for Subsequent Malignancy When considering the risk of SMNs associated with genetic predisposition, one must consider genetic disorders with high risk for both primary and subsequent malignancy, as well as less well-defined gene-environment interactions. The former category, which accounts for a small minority of SMNs, includes hereditary breast cancer (BRCA1/BRCA2), heritable retinoblastoma, neurofibromatosis, nevoid basal cell carcinoma (BCC), Li-Fraumeni syndrome, hereditary nonpolyposis colorectal cancer (Lynch syndrome), multiple endocrine neoplasia, Bloom syndrome, xeroderma pigmentosum, and other syndromes.4,5 Table 62-3 summarizes these syndromes and common sites for primary and subsequent neoplasms; in addition, several are discussed here. Table 62-3 Common Hereditary Cancer Syndromes Mutations in BRCA1 and BRCA2 are associated with high risk for secondary breast cancer.6,7 In a study of 810 women with a stage I or II primary breast cancer in the setting of BRCA1 or BRCA2, a contralateral breast cancer developed in 149 subjects (18.4%), with a 15-year actuarial risk of 36.1% and 28.5%, respectively, for women with a BRCA1 or BRCA2 mutation. Younger age (<50 years) at primary breast cancer diagnosis and having two or more first-degree relatives with breast cancer also increased risk. A reduction of risk was noted with oophorectomy (RR = 0.47).6 Among 396 women with stage I or stage II primary breast cancer in the setting of a BRCA1 or BRCA2 mutation, the 5-year actuarial risk of ipsilateral breast cancer was 5.8%, and the 10-year risk was 12.9%. Receipt of chemotherapy and radiotherapy both reduced risk (RR = 0.45 and 0.28, respectively). Oophorectomy was associated with a significant risk reduction (RR = 0.33). On average, after a diagnosis of breast cancer, the annual risk of ipsilateral breast cancer risk in BRCA mutation carriers is 1.2% per year.7 Of course, in addition to these risks, patients with BRCA1 and BRCA2 also have an increased risk for primary ovarian cancer,8 and patients with BRCA2 have an increased risk for prostate cancer, pancreatic cancer, gallbladder and bile duct cancer, stomach cancer, and malignant melanoma.9 Of note, mutations in BRCA1, BRCA2, or TP53 are not thought to be responsible for the increased incidence of SMN among Hodgkin lymphoma survivors. In a study of 44 patients who experienced one or more SMNs, mutations in the TP53 gene were examined in all 44 patients and BRCA1 and BRCA2 were examined in 19 female patients in whom one or more secondary breast cancer developed. One of 44 patients tested for TP53 harbored a novel homozygous germline abnormality, and one of 19 patients tested for BRCA2 carried a previously described heterozygous inactivating mutation; no germline BRCA1 mutations were identified.10 Mutations in mismatch repair genes in persons with hereditary nonpolyposis colorectal cancer can lead to the more site-specific colorectal cancer syndrome associated with other gastrointestinal cancers (Lynch syndrome type I) or the family cancer syndrome, in which early-onset endometrial and stomach cancers are seen in addition to colorectal cancer (Lynch syndrome type II).11,12 Neurofibromatosis type 1 (NF1), which results from a mutation in the NF1 gene at chromosome 11q12, is not associated with malignancy in the majority of patients with this syndrome. However, patients (and particularly children) with NF1 have an increased risk for leukemias, central nervous system (CNS) tumors, and peripheral nerve sheath tumors.13,14 In a report from the Late Effects Study Group, NF1 was second only to retinoblastoma among children with a predisposition to SMN.15 Retinoblastoma, which is associated with germline mutation of the RB1 gene at chromosome 13q14, is the most common hereditary syndrome associated with SMN after childhood cancer.18–18 Survivors of retinoblastoma have a significantly increased risk of sarcomas both inside and outside the radiotherapy field, along with leukemia, melanoma, and epithelial tumors such as breast and lung cancers. In a cohort of 1604 patients treated from 1914 to 1984, the cumulative incidence of SMN was 51% and 5% at 50 years for heritable and nonheritable retinoblastoma survivors, respectively.19 A follow-up 9 years later found 50-year cumulative incidences to be 36% and 5.7%, with standardized incidence ratios (SIRs) of observed/expected SMNs of 19 and 1.2, respectively, for persons with heritable disease versus nonheritable disease. Radiotherapy increased SMN risk in heritable patients 3.1-fold.20 The cumulative probability of death from SMN was 25.5% for bilateral disease survivors, and the increased risk extended beyond 40 years after retinoblastoma diagnosis.21 Li-Fraumeni syndrome, which is associated with germline mutation in the TP53 gene at chromosome 17q13, is characterized by increased risk for breast cancer, sarcoma, leukemia, brain tumors, adrenocortical carcinoma, and gonadal germ cell tumors.22,23 Several small studies have reported an excess of multiple primary tumors in patients with Li-Fraumeni syndrome, but this phenomenon has not been systematically studied.10,24,25 Nevoid BCC syndrome associated with mutation of the PTCH1 gene on chromosome 9 is associated with BCC and medulloblastoma, and many BCCs can develop during a patient’s lifetime. Although multiple BCCs are reported in survivors of childhood cancer, it is likely that only persons who experience these along the track of radiotherapy within a very short latency of 6 months have this genetic predisposition. In other persons, including those treated with total body irradiation (TBI) for stem cell transplant or radiotherapy after childhood cancer, early-onset nonmelanoma skin cancers are noted, although environmental and lifestyle factors have not been systematically collected and represent an area of future research.26,27 Bloom syndrome, xeroderma pigmentosum, and ataxia telangiectasia are all rare disorders of DNA repair that can lead to multiple primary cancers, including leukemia and lymphoma, skin cancer, soft tissue sarcomas, and epithelial tumors. However, these syndromes have well-recognized phenotypes and thus are not an occult cause of SMN.28–32 Data on the carcinogenic potential of ionizing radiation exposure from cancer treatment, other disease treatment, and environmental causes have been available for several decades. These data have shown that organs differ in their sensitivity for SMN and the dose needed to induce malignancy and that latency and age at time of exposure remain important risk factors.33–41 Risk of SMN from radiation therapy appears to be proportional to the number of premalignant stem cells created and the number of cells that survive radiation therapy, which in turn are related to cellular killing, cellular repopulation occurring between fractions and after the last fraction, and the ratio of proliferation rate for premalignant to normal cells.42 Furthermore, the type and energy of radiation and the time course during which exposure occurs all affect risk for SMNs. Low-linear-energy transfer radiation, such as x-rays and gamma rays, is sparsely ionizing and is generally less efficient in tumor induction than densely ionizing high-linear-energy transfer radiation (e.g., α particles and neutrons), for which the carcinogenic effectiveness is not diminished at high doses and may be increased with fractionation and protraction. Risk is related to age at treatment; generally, younger age is associated with increased risk, total dose, and mode of radiation therapy delivery. Latency periods are long, and risk appears to rise without a clear plateau for decades after radiation therapy is conducted.43–49 Many of the data on SMN in childhood cancer come from the Childhood Cancer Survivor Study (CCSS), which evaluates long-term outcomes in childhood cancer survivors treated between 1970 and 1987 who survived at least 5 years after the initial diagnosis. In this cohort, risk for SMN was examined with respect to therapeutic exposures, which were well documented through chart abstraction for each participant.50,51 In addition, radiation dosimetry was evaluated for some in-depth analyses of radiation risk.52 In the most recent report on subsequent neoplasms from the CCSS, among 14,359 survivors, 1402 individuals had a total of 2703 subsequent neoplasms, which included 802 second malignant neoplasms, 159 nonmalignant meningiomas, 169 benign or in-situ neoplasms, and 1574 nonmelanoma skin cancers. In multivariable analysis, risk of any subsequent neoplasm was increased 2.7-fold with radiotherapy exposure. Risk related to radiotherapy for malignant neoplasms other than nonmelanoma skin cancer was increased 2.6-fold, risk of meningioma was increased 16.6-fold, and risk of nonmelanoma skin cancer was increased 4.4-fold.46 Dose-response relationships also appear to differ between organs with respect to risk of SMN in childhood cancer survivors, as is evidenced by work done within the CCSS and reviewed by Armstrong.53 Among 116 survivors with a subsequent CNS neoplasm, compared with control subjects who did not have a subsequent CNS neoplasm, radiation therapy was associated with an increased risk for any subsequent CNS malignant neoplasm, and specifically for subsequent glioma (odds ratio [OR] = 6.78) and meningioma (OR = 9.94). Furthermore, linear dose-response relationships between radiation dose and secondary glioma and meningioma were identified. The excess RR per Gy, equal to the dose of the linear response function, was 0.33 per Gy for glioma and 1.06 per Gy for meningioma. With increasing length of follow-up, the number of new glioma cases declined, but the incidence of meningioma continued to increase with longer length of follow-up.54 In analyses of secondary thyroid cancer, risk increased with radiation dose to the thyroid gland for doses as high as 29 Gy and decreased for doses greater than 30 Gy, with this linear exponential dose most pronounced in persons younger than 10 years at the time of exposure.55,56 Risk of breast cancer after chest radiation therapy is now well established. SIR (evaluating observed/expected) for breast cancer was 24.7 in women treated with chest radiotherapy in the CCSS compared with an SIR of 4.8 for women who were not treated with chest radiation therapy.46,57 Notably, receipt of ovarian radiation reduced rates of breast cancer (RR, 0.6). In Hodgkin lymphoma survivors who were treated with chest radiation, the cumulative incidence of breast cancer at age 40 years was 12.9%.57 To evaluate the dose-response relationship between chest radiation therapy and the development of breast cancer, 120 confirmed breast cancer cases were matched with control subjects, and a linear relationship was identified between risk of developing breast cancer and radiation dose. At a dose of 40 Gy to the breast, an elevenfold increased risk for the development of breast cancer was found. The slope of the dose-response curve was altered when the radiation dose to the ovaries was considered, because ovarian radiation exposure of 5 Gy or more decreased the risk of breast cancer.58 Risk of SMN related to radiotherapy among adults treated for cancer clearly differs from that among children. In a report from SEER, in patients ≥20 years who were diagnosed with a primary cancer between 1973 and 2002, an analysis compared risk for SMN among those treated with or without radiotherapy. In this group of 647,672 patients with cancer, a second solid organ malignancy developed in 60,271 (9%). For each of the first cancer sites, the RR of developing an SMN associated with radiotherapy was elevated and was highest for organs that typically received more than 5 Gy. As seen in studies of childhood cancer survivors, risk decreased with increasing age at diagnosis and increased with time since diagnosis. It was estimated that 3266 excess solid organ SMNs could be related to radiotherapy, and by 15 years after diagnosis, there were five excess cancers per 1000 patients treated with radiotherapy.59 However, survivors of adult-onset malignancies who were treated with radiotherapy are clearly at some increased risk for SMN, as evidenced by several large population-based studies of SMNs. Travis and colleagues60 identified 2285 second solid cancers in 40,576 1+-year survivors of testicular cancer who were treated between 1943 and 2001. Statistically significant increased risks of solid cancers were observed among patients treated with radiotherapy alone (RR = 2.0) or in combination with chemotherapy (RR = 2.9).60 In contrast, among 42,722 survivors treated between 1943 and 2002, secondary leukemia developed in 89 patients (EAR = 10.8 per 100,000 person-years). In multivariate analyses, leukemia risk was higher among patients whose initial management included chemotherapy compared with those receiving radiotherapy alone.61 Among 104,760 one-year survivors of cervical cancer, 12,496 SMNs were found overall (SIR = 1.33). Compared with the general population, patients with cervical cancer who were treated with radiotherapy, but not patients who did not receive radiotherapy, were at increased risk for all second cancers, particularly at the sites of the colon, rectum/anus, urinary bladder, ovary, and genitalia. The association of radiotherapy with second cancer risk was modified by age at cervical cancer diagnosis for the rectum/anus, genital sites, and urinary bladder, with higher hazard ratios for second cancer at younger ages of diagnosis of cervical cancer.62 In a cohort of 32,941 patients treated for Hodgkin lymphoma between 1935 and 1994, SMNs occurred in 2153 and the risk for solid tumors was elevated 2.3-fold in patients who were treated with radiation alone, 1.7-fold in those treated with chemotherapy alone, and 3.1-fold with combined modality therapy.63 In a cohort of 770 female patients who had been diagnosed with Hodgkin lymphoma before age 41 years, breast cancer developed in 48. Risk of breast cancer increased statistically significantly with radiation dose: patients who received 38.5 Gy or more had an RR 4.5 times that of patients who received less than 4 Gy. Patients who received combined modality therapy had a statistically significantly lower risk than those treated with radiotherapy alone (RR = 0.45). Breast cancer risk increased with increasing radiation dose among patients who received radiotherapy alone at doses ≥38.5 Gy (RR = 12.7).64 The most common second cancers associated with radiotherapy exposure are shown in Table 62-4, together with the most common primary cancers for which the radiotherapy was administered. Table 62-4 Common Radiotherapy-Associated Cancers The relationship between chemotherapy and SMN is likely more complex than that with RT, because agents appear to have different oncogenic potential, and a number of different mechanisms are associated with SMN development. Table 62-5 summarizes some of the common chemotherapeutic agents and subsequent malignancies with which they are associated. Table 62-5 Common Chemotherapy-Associated Cancers
Second Malignant Neoplasms
Introduction
Primary Cancer
Observed Versus Expected
Excess Absolute Risk/10,000 Person Years
Lip
1.16
34
Oral cavity
2.45
231
Nasopharynx
1.49
47
Salivary gland
1.25
644
Colon
1.07
13
Anal
1.24
36
Lung
1.36
65
Larynx
1.71
150
Nasal
1.44
68
Breast
1.18
23
Cervix
1.32
24
Vulva
1.12
16
Ovary
1.18
15
Testis
1.62
21
Bladder
1.17
34
Kidney
1.13
23
Renal pelvis/ureter
1.29
55
Bone sarcoma
1.24
13
Soft tissue sarcoma
1.19
20
Melanoma of skin
1.24
27
Ocular melanoma
1.16
24
Other ocular (nonretinoblastoma)
1.35
51
Brain and central nervous system
1.11
4
Thyroid
1.11
8
Hodgkin lymphoma
2.22
49
Non-Hodgkin lymphoma
1.14
14
Chronic lymphocytic leukemia
1.19
38
Chronic myeloid leukemia
1.16
19
Acute lymphocytic leukemia
1.55
5
Childhood cancer
6.07
15
Retinoblastoma
14.71
24
Ewing sarcoma
14.84
44
Hodgkin lymphoma
9.55
39
Central nervous system peripheral neuroectodermal
12.54
26
Risk Factor
Examples
Genetic syndromes
Potential genetic modifying factors
Disease and treatment
Lifestyle-modifying factors
Infection
Genetic Risks for Subsequent Malignancy
Syndrome
Common Mutations or Pathways
Cancer Risks
Hereditary breast cancer
BRCA1
Breast, ovarian
BRCA2
Breast, ovarian, prostate, pancreatic, gallbladder and bile duct, stomach, malignant melanoma
Hereditary nonpolyposis colorectal cancer
DNA mismatch repair
Colon, endometrium, stomach, small intestine, hepatobiliary, kidney, ureter, ovary
Neurofibromatosis
NF1
Leukemia, central nervous system, peripheral nerve sheath
Retinoblastoma
RB1
Sarcoma, leukemia, melanoma, breast, lung
Li-Fraumeni syndrome
TP53
Breast, sarcoma, leukemia, central nervous system, adrenocortical carcinoma gonadal germ cell
Nevoid basal cell carcinoma
PTCH1
Medulloblastoma, basal cell carcinoma
Bloom syndrome
Xeroderma pigmentosum
Ataxia telangiectasia
DNA repair
Lymphoma, leukemia, skin, soft tissue, epithelial
Treatment-Associated Risks for Subsequent Malignancies
Radiation Therapy
Radiation Field
Common Primary Malignancy Treated
Common Subsequent Malignancies
Brain
Central nervous system, leukemia
Central nervous system
Neck
Hodgkin lymphoma
Thyroid
Thoracic
Hodgkin lymphoma, Wilms tumor, sarcoma, breast
Breast, lung
Abdomen
Sarcoma, Wilms, Hodgkin, gastrointestinal
Colon
Pelvis
Gonadal
Gonadal
Soft tissue
Sarcoma
Sarcoma
Bone
Sarcoma, retinoblastoma
Sarcoma
Chemotherapy
Chemotherapy
Common Primary Cancers
Subsequent Malignancies
Alkylating agents
Sarcoma
Lymphoma
Myelodysplastic syndrome, leukemia
Etoposide
Sarcoma
Hodgkin lymphoma
Leukemia
Anthracyclines
Sarcoma
Lymphoma
Breast cancerRelated posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

