Chapter 18 RISK ASSESSMENT
INTRODUCTION
This chapter gives an overview of risk assessment, with particular emphasis on falls, abuse and neglect of older people, and aggression. Risk assessment involves the consideration of risk factors, harm and likelihood (McSherry 2004). These factors are covered in this chapter, with the addition of intervention strategies and, in relation to abuse and neglect specifically, the different types are identified. In the final section, after aggression, there is a short discussion on the perplexing issue of self-neglect. Suicide is another important topic in regard to risk assessment and this is dealt with in Chapter 21.
FALLS
One of the most significant risks for older people relates to the incidence of falls. In Australia, for the year 2005–06, the estimated number of hospitalised injury cases due to falls in people aged 65 years and over was 66,800—a rise of 10% since 2003–04. Half of all fall injury cases for people aged 65 years and older occurred in the home (Bradley & Pointer 2008). Mild to serious physical injury can occur from falls, but with any fall the older person usually suffers some longer term psychological distress and fear of falling again. The result of this is that they reduce their activities, which can increase dependency, limit activities of daily living (ADL) and instrumental activities of daily living (IADL) function, increase morbidity and reduce their ability to socialise and overall quality of life (Kressig et al 2001).
Causative factors related to falls are multifactorial (i.e. intrinsic factors or extrinsic factors, or a combination of both, contribute to the problem). Listed below are some of these factors (American Geriatrics Society 2001, Lord et al 2007):
Falls assessment
There are numerous general and specific falls assessment instruments that have been developed over the years. A number of reviews assessing the value of these instruments have been undertaken. If the mental health worker intends to use one or more of the available instruments, it would be prudent to examine the reviews which summarise many of the characteristics and will make an informed choice somewhat easier. Reviews in this area have been conducted by Haines et al (2007), Lundin-Olsson et al (2003) and Perell et al (2001).
Prevention of falls
An enormous amount of effort has gone into prevention interventions and programs for falls (Lord et al 2007). A Cochrane Database Systematic Review to assess the effects of interventions to reduce the incidence of falls in older people living in the community found a number of interventions to be effective (Gillespie et al 2009). Over 100 trials involving 55,303 people were included in the review. The interventions likely to be beneficial in reducing the risk and rate of falls were tai chi and multiple component exercise (individual and group). Other prevention strategies such as multifactorial assessment and intervention, home safety interventions and vitamin D supplements still require further research to confirm their effectiveness. There was some evidence that falls prevention strategies can be cost effective.
ABUSE AND NEGLECT
Abuse and neglect often go undetected and there are many reasons as to why this happens. An older person, for example, may not be able to report the abuse due to cognitive impairment or communication difficulties caused by a stroke. They could be afraid of the perpetrator and fear retaliation, or if they lose the support of this person they may have to go into an RACF or some other form of supportive accommodation. Feelings of shame and embarrassment may prevail if it is a family member who is the perpetrator. Also, it can be very difficult to differentiate normal ageing changes from signs of neglect and mistreatment. For example, weight loss and bruising and other such signs can be easily explained away as poor appetite or a fall (Anetzberger 2005, Carney et al 2003).
Elder abuse is defined as any pattern of behaviour that causes physical, psychological, financial and social harm to an older person (World Health Organization 2002). Abuse and neglect is a complex and multifactorial issue and can occur in a variety of ways. Determining the type of abuse will be helpful in planning how to intervene. It is generally categorised in the following ways:
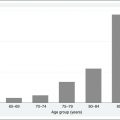
The extent of this problem is very difficult to determine, as it is often not reported. However, a recent national prevalence study of elder abuse was conducted in private households in England, Scotland, Wales and Northern Ireland (Biggs et al 2009). Of the 2111 respondents, 2.6% reported abuse by family members, close friends or healthcare workers. The predominant type of reported abuse was neglect (1.1%), followed by financial abuse (0.6%), with 0.4% of respondents reporting psychological abuse, 0.4% physical abuse and 0.2% sexual abuse. Women were significantly more likely to have experienced abuse than men.
Risk factors
The perpetrators often have a mental illness, abuse substances or are somehow dependent on the older person. They are usually family members, such as a spouse or adult children and grandchildren.
Carer burden is also a significant risk factor. If a carer is not getting enough support financially, emotionally and physically, or even simple recognition for their caring role, they can become very resentful (Choi & Mayer 2000).


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


