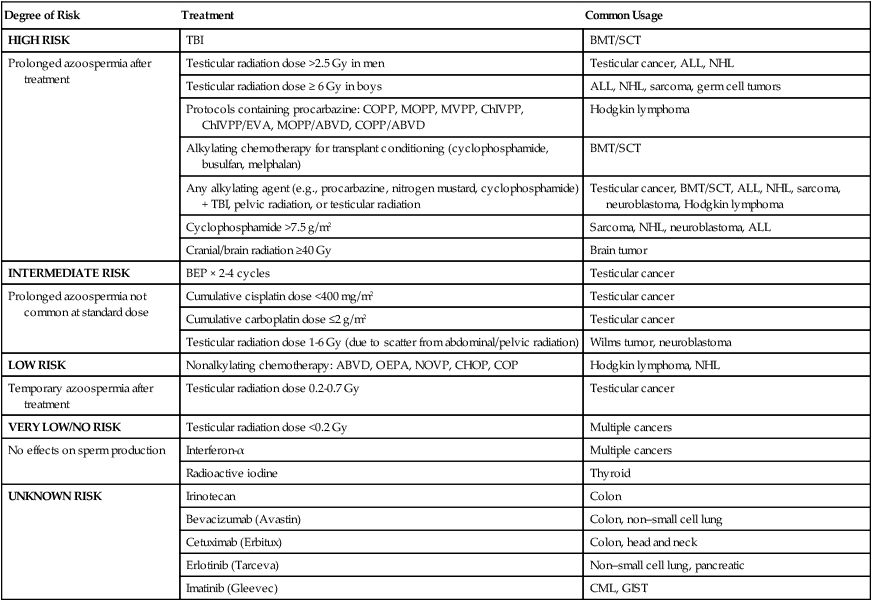
Lynda Kwon Beaupin, Tracey O’Connor and Donald L. Trump • Reproductive complications resulting from cancer or its treatment are expected to increase as the number of cancer survivors increases. • The risks of infertility related to cancer therapy and the available fertility preservation options should be discussed with all patients of reproductive age before cancer therapy begins. • Oligospermia is present in more than 50% of patients with Hodgkin lymphoma and testicular cancer. • Prostatectomy and other pelvic surgeries are associated with erectile dysfunction; retroperitoneal dissection is associated with retrograde ejaculation. • Erectile dysfunction occurs within 2 years after treatment in 60% to 80% of patients with prostate cancer who are treated with external beam radiation. • The use of sildenafil has reestablished potency in a large number of patients with surgery- or radiation-induced erectile dysfunction. • Radiation can affect testicular spermatogenesis after doses as low as 15 cGy. Ovarian function is more resistant, but the effects are age related. • Gonadal shielding and ovarian transposition ameliorate the effects of radiation on gonadal function. • Gynecologic surgery can have a direct impact on sexual function by altering the normal female genital anatomy. • Alkylating agents are associated with the highest rates of infertility in men and women. • Doses and duration of chemotherapy agents are directly associated with the risk of infertility. • The return of menses does not indicate preservation of ovarian function. • Cancer complicates 1 in every 1000 pregnancies. • The highest risk of congenital abnormalities is associated with chemotherapy or radiation exposure during the first trimester of pregnancy. • It has not yet been determined whether the use of gonadotropin-releasing hormone analogs protects ovarian function and preserves spermatogenesis. The ovary produces mature fertilizable eggs, sex steroids, and reproductive/gonadal peptides. These activities are carried out in an integrated manner within the follicle. Humans have approximately one million follicles at birth. During the reproductive years, typical cyclic follicular recruitment, selection, and dominance eventually deplete the ovary of follicles, leading to cessation of ovarian function and menopause.1 In males, the testes secrete androgenic hormones and produce mature spermatozoa. These two processes are highly interrelated and regulated by multiple factors. Much like the ovary, compartments of the testes serve different functions. Spermatogenesis occurs in Sertoli cells within the seminiferous tubules. The interstitial or Leydig cells are essential for testosterone synthesis. Testosterone is transported from the Leydig cells to the seminiferous tubules, where it enhances spermatogenesis.2 The main regulators of testicular and ovarian function are the gonadotropins, follicle-stimulating hormone (FSH), and luteinizing hormone (LH). The biosynthesis and secretion of gonadotropins are modulated by an interplay of hypothalamic factors: gonadotropin-releasing hormone (GnRH), intrapituitary factors (pituitary peptides—activin and follistatin), and feedback by gonadal factors.1,2 Depending on the reproductive stage, estrogens can either increase or decrease gonadotropin production. Increased levels of estrogen in females or testosterone in males downregulate gonadotropin secretion. However, increased levels of estrogens at the time of LH surge exert a positive feedback effect. The gonadal proteins activin, inhibin, and follistatin also modulate the release of FSH.3 Inhibin decreases and activin stimulates gonadotropin function. Follistatin also inhibits FSH but is less potent than inhibin. Regulatory effects of gonadotropins on the ovaries and testes are similar. Activation of gonadotropin receptors on the plasma membranes of Leydig cells and granulosa and theca cells induces the regulation and production of testosterone and of female steroid hormone production and follicular maturation, respectively.1,2 Central nervous system damage by primary or metastatic cancer or indirectly through paraneoplastic involvement can have a considerable impact on reproductive function. Pituitary prolactin-secreting adenomas are commonly associated with impotence in men and amenorrhea and galactorrhea in women. Other pituitary adenomas can affect reproductive function by destroying LH- and FSH-producing gonadotropes. Metastatic disease that affects the hypothalamus-pituitary axis also leads to reproductive dysfunction. Paraneoplastic syndromes are an infrequent but well-documented cause of reproductive dysfunction.4 Although men with Hodgkin lymphoma may have pretreatment impairment of spermatogenesis, no well-defined predictors of semen quality at the time of diagnosis have been identified. Some studies have indicated a correlation between elevated erythrocyte sedimentation rate and semen quality.5,6 In other studies, no correlation has been found between semen abnormalities and disease stage or systemic symptoms.7 A recent study of patients with early-stage Hodgkin lymphoma reported that 90% had good or intermediate sperm quality.8 In this study of 474 patients, no relation was found between sperm quality and age, clinical stage, or smoking. However, B symptoms (fever, weight loss, and night sweats) had a statistically negative effect on sperm quality, especially fever and night sweats. No association has been found between sperm quality and pretreatment FSH levels. The association between testicular cancer and abnormalities of spermatogenesis is even more pronounced. The degree of spermatogenic abnormalities in these patients is greater than can be attributable to local tumor effect or the degree of systemic involvement. A recent study found that total sperm count was lower in men with testicular germ cell cancer (median, 29 × 106/mL vs. 162 × 106/mL) compared with healthy men.9 Histologic investigations have revealed a high prevalence of dysfunctional spermatogenesis even in the contralateral testicle that is uninvolved with cancer.10 An increased risk of testicular cancer has also been observed in men with an abnormal semen analysis and infertility. Infertile men with abnormal semen analyses have a twentyfold higher incidence of testicular cancer compared with the general population.11 The specific links between the pathological events that cause infertility and testicular cancer remain unclear. Erectile dysfunction in patients undergoing radical prostatectomy commonly occurs after surgery.12–15 Steineck and colleagues16 randomly assigned 376 patients to radical prostatectomy versus watchful waiting; the incidence of erectile dysfunction was significantly higher in the surgical group (80%) compared with the observation group (45%). Bilateral nerve-sparing surgeries are considerably more effective in allowing the patient to maintain an erection compared with unilateral nerve-sparing surgeries. Potency rates after bilateral sparing surgery at 3 years were 76% compared with 30% with unilateral nerve-sparing surgery in previously potent patients younger than 60 years. The rates of potency are lower in older patients and in patients with known erectile dysfunction before surgery.17 A recent study also indicated that incontinence and sexual dysfunction remain high with robotic-assisted laparoscopic radical prostatectomy; patients should not expect fewer adverse effects with this newer method.18 Retroperitoneal lymph node dissection (RPLND) frequently damages the sympathetic nerves that innervate the seminal vesicles and the bladder neck, which leads to loss of seminal vesicle emission or emission without bladder neck closure (retrograde ejaculation).19,20 In a recent report on long-term survivors of testicular cancer, when comparing different treatment modalities, only RPLND was associated with sexual dysfunction related to ejaculatory dysfunction.21 A selective RPLND, as described by Donohue and colleagues,22 results in the sparing of a unilateral sympathetic chain and preservation of antegrade ejaculation. Jacobsen and colleagues23 reported preserved antegrade ejaculation in 89% of patients undergoing an RPLND after chemotherapy. Conventional rectal surgery is associated with high rates of impotence and retrograde ejaculation, likely because of the damage of the pelvic autonomic parasympathetic and sympathetic nerves by blunt dissection. However, the introduction of total mesorectal excision (TME) has been associated with a lower rate of local recurrence and a higher rate of potency preservation. A comparison of sexual outcomes of patients with conventional surgery and TME showed that the ability to have intercourse dropped from 75% to 13% in the conventional surgery arm compared with a drop from 67% to 29% in the TME group.24 A more recent study demonstrated earlier recovery of normal voiding and sexual function for patients undergoing robotic-assisted TME compared with patients who underwent laparoscopic TME.25 Limited information is available about sexual dysfunction in women with rectal cancer. One study reported that 39% of sexually active women and 62% of all women treated for rectal cancer had Female Sexual Function Index scores that were considered abnormal despite the use of nerve-sparing surgery at the reporting institution.26 Gynecologic surgeries can alter sexual function directly by affecting the anatomy of the female genital tract. In one study of 50 women who underwent pelvic surgery for vulvar, cervical, or endometrial cancer, 83% reported sexual problems compared with 20% of the control group.27 They also reported decreased sexual desire and impaired vaginal lubrication. A recent study found that in 179 women with a history of invasive cervical cancer, the majority of patients were sexually active. Women who had hysterectomies less often reported a lack of interest in or desire for sexual activity compared with those who had not had hysterectomies.28 Among women with breast cancer, several prospective studies show no difference in quality of life outcomes or sexual functioning on the basis of surgical treatment.29,30 In younger women with breast cancer (≤50 years), sexual problems were significantly greater immediately after surgery, and although these problems decreased over time, they were still greater at 1 year after surgery than before diagnosis.31 Pituitary dysfunction as a result of irradiation is attributed to a disturbance in the hypothalamic-pituitary axis. In both men and women, it has been shown that cranial irradiation of 35 to 40 Gy or greater disturbs the hypothalamic-pituitary axis and increases the risk of infertility.32 A study of 593 long-term survivors of childhood acute lymphoblastic leukemia disclosed an increased rate of infertility among those treated with whole-brain radiation.33 The testis is one of the most radiosensitive tissues; very low doses of radiation cause significant impairment of testis function. Permanent Leydig cell dysfunction occurs with a dose of 2000 to 3000 cGy. Therapeutic irradiation (2400 cGy) to the testes in patients with acute leukemia causes Leydig cell dysfunction, which is manifested by low testosterone levels or a poor testosterone response to gonadotropins.34,35 Radiation doses as low as 15 cGy transiently suppress spermatogenesis, and doses higher than 600 cGy permanently destroy the germinal elements.35 Berthelsen36 evaluated the effects of adjuvant irradiation for seminoma on gonadal function. Retroperitoneal and ipsilateral iliac irradiation resulted in an estimated 200 to 1300 cGy scatter to the unaffected contralateral testicle. Azoospermia developed in two thirds of patients, and it took a median of 540 days from the end of treatment before spermatozoa were again found in semen samples. A median of 1250 days passed before the pretreatment sperm count was reached. Sperm counts were low (median: 6 × 106 per ejaculate) up to 5 years after treatment, and serum FSH was elevated (median: 61 IU/L). No evidence of an increase in posttreatment congenital abnormalities was found, and the posttreatment conception rate was 60% to 70%. Human oocytes are sensitive to the effects of radiation, and it has been suggested by Wallace et al.37 that the LD50 (the radiation dose that is required to kill 50% of oocytes) is less than 2 Gy. In a review of the risk of premature menopause because of cancer treatment, it was found that younger ovaries are less sensitive to the effects of irradiation. Although a radiation dose of 6 Gy is sufficient to result in permanent ovarian failure in women older than 40 years, higher doses in the range of 10 to 20 Gy result in permanent ovarian failure in the majority of patients who are treated in childhood.38 Radiation therapy is commonly used as definitive treatment for patients with localized or locally advanced prostate cancer. Although the etiology of erectile dysfunction after definitive radiation therapy for prostate cancer is likely to be multifactorial, the arteriogenic mechanism appears to be more significant than the cavernosal mechanism. Maintenance of normal erection requires both vasodilation of penile arteries (arteriogenic element) and concomitant relaxation of the corporal smooth muscles (cavernosal element). Duplex ultrasonography can assess arteriogenic function by measuring peak penile blood flow and cavernosal function by measuring distension of the corpora cavernosa in the setting of normal penile flow.39 In patients with prostate cancer who have radiation therapy–induced erectile dysfunction, duplex ultrasonography confirmed a 63% rate of arteriogenic dysfunction. By contrast, with prostatectomy-induced erectile dysfunction, only 32% of patients had arteriogenic dysfunction and 52% had cavernosal dysfunction.39 Erectile dysfunction is frequently seen after external beam radiation for prostate cancer and increases in frequency with time. In 290 patients with prostate cancer who were treated with radiation, 62% and 41% of those who were potent before treatment maintained potency at 12 and 24 months, respectively, and potency rates dropped further with time.40 Conformal radiation therapy limits the radiation field while delivering a high dose of radiation to the prostate and may be associated with a lower degree of impotence.41,42 Mantz and colleagues42 described a 5-year potency rate of 53% among 287 patients with prostate cancer who were treated with 6000 to 7200 cGy conformal radiation therapy.42 The use of brachytherapy in the treatment of prostate cancer has also been associated with a lower incidence of impotence. Prostate brachytherapy as monotherapy was associated with 5- and 6-year potency rates of 76% and 52%, respectively, among previously potent patients. Furthermore, the addition of external beam radiation or antiandrogen therapy to brachytherapy decreases the rates of potency substantially.43,44 The use of intensity-modulated radiation therapy for nonmetastatic prostate cancer has increased significantly in the past decade, and although patients receiving this therapy are less likely than those receiving conformal radiation therapy to undergo additional cancer treatments, there is an increased association with erectile dysfunction 45. Pelvic radiotherapy for cervical carcinoma is associated with vaginal atrophy, shortening, or agglutination, making intercourse difficult or impossible for women who receive this therapy.46 At 2 years of follow-up, Jensen and colleagues47 reported that 85% of women had no interest in sex, 55% had dyspareunia, and 50% had vaginal shortening. These problems were very significant in comparison with the women’s own premorbid sexual function and age-matched control subjects. Abdominal and pelvic radiation therapy may be part of therapy for management of Wilms tumor, pelvic rhabdomyosarcoma, and Ewing sarcoma of the pelvis or spine. Young patients exposed to flank radiation (20 to 30 Gy) may have preservation of ovarian function. Women who do conceive after treatment with this degree of abdominal radiation have a significant risk of preterm delivery, low birth weight infants, and infants who are small for gestational age compared with control subjects.48 Other data also found a particularly high risk of preterm delivery and low birth weight but no congenital malformations in women who conceive within 1 year after completion of irradiation. These data imply that uterine or hormonal defects are the cause of these abnormalities.49 Leuprolide and goserelin are two potent GnRH analogs that are commercially available in the United States. These two analogs are much more potent in stimulating gonadotropin release than is GnRH. Initial treatment with GnRH agonists results in an LH and FSH surge with resultant gonadal steroid synthesis stimulation. However, after 10 to 14 days of continuous exposure to GnRH analogs, GnRH receptors on gonadotropin cells in the pituitary are downregulated, resulting in inhibition of LH/FSH release and gonadal suppression. After prolonged GnRH analog therapy, testosterone and estrogen levels are suppressed to castrate levels. In men, this is usually associated with substantial loss of sexual desire and a marked decrease in frequency, magnitude, duration, and rigidity of nocturnal erections.50 Treatment for longer than 2 years results in atrophic testes, which might not recover even if GnRH is discontinued.51 In women, the use of GnRH in the adjuvant treatment of breast cancer is associated with an increased rate of sexual dysfunction, but the symptoms are usually reversible upon discontinuation of therapy.52 Antiandrogens bind to and block the activity of androgen receptors. Androgen receptor blockage is associated with a rise in FSH/LH and a resultant rise in serum testosterone.53 Antiandrogens, such as flutamide, bicalutamide, or nilutamide, are commonly used in the management of prostate cancer either with luteinizing hormone-releasing hormone (LHRH) analogs or after LHRH agonist/antagonist failure. A recent prospective study combining flutamide and leuprolide demonstrated a decrease in libido, sexual activity, and perceptions of masculinity during therapy.54 Once therapy ended, these levels improved during a 2-year period, although not to baseline levels. Erectile function, however, did return to baseline. High-dose bicalutamide has been evaluated as monotherapy in patients with advanced prostate cancer. Although some studies suggest comparable clinical activity, significantly less impotence and loss of libido occur with antiandrogen monotherapy.55 The ability to maintain potency while receiving antiandrogen monotherapy is limited. A study evaluating flutamide as monotherapy in 147 previously untreated patients with prostate cancer resulted in 22% preservation of sexual activity and 20% preservation of morning erection at 2 to 6 years from the start of therapy.56 The median time to loss of morning erections and sexual activity was 12.9 and 13.7 months, respectively. In a randomized study of standard (n = 45) versus high-dose (n = 53) tamoxifen, patients experienced hot flashes (85%), vaginal dryness and/or dyspareunia (47%), and decreased sexual desire (44%).57 Decreased sexual interest correlated significantly with vaginal dryness and/or dyspareunia. These symptoms decreased significantly after discontinuation of tamoxifen. Other reports have shown that tamoxifen does not make a significant contribution to sexual dysfunction in women older than 50 years,58 and in a randomized study that examined only premenopausal women, patients receiving tamoxifen alone did not report decreased sexual function.59 Aromatase inhibitors are increasingly used as the standard hormonal therapy for postmenopausal women with breast cancer and are successful in increasing distant and overall disease-free survival, as well as preventing contralateral breast cancer, compared with tamoxifen. Aromatase inhibition results in a marked decrease in estrogen synthesis, leading to minimal levels of circulating estrogen. In a recently published report of the quality-of-life measurements of postmenopausal women participating in the “Arimidex, Tamoxifen, Alone or in Combination” (ATAC) trial, patients reported diminished libido (34% vs. 26%) and dyspareunia (17% vs. 8%) significantly more frequently with anastrozole (Arimidex) treatment than with tamoxifen treatment.60 Many chemotherapeutic agents are gonadotoxic. Temporary infertility among men is not uncommon during cancer treatment as a result of cytotoxic damage to rapidly differentiating spermatogonia.61,62 Fertility in men may be evaluated through semen analysis and assessment of sperm concentration, motility, and morphology. Among chemotherapeutic agents, higher dose alkylating agents (e.g., cyclophosphamide, chlorambucil, procarbazine, and busulfan) and cisplatin are most commonly associated with prolonged or permanent infertility.61,62 Table 60-1 summarizes commonly used cancer therapy regimens and the degree of risk of azoospermia among men. Combination chemotherapies that contain alkylating agents impair fertility far more than do nonalkylating combinations. The majority of men with Hodgkin lymphoma who are treated with mechlorethamine, vincristine, procarbazine, and prednisone (MOPP) become severely oligospermic or azoospermic, and testicular biopsies confirm germinal aplasia.63,64 Comparison of MOPP with the Adriamycin, bleomycin, vinblastine, and dacarbazine (ABVD) regimen revealed a considerably higher azoospermia with MOPP (100%) than with ABVD (35%), and men treated with MOPP rarely resumed spermatogenesis.65 Azoospermia also occurred considerably less often in patients receiving two cycles of MOPP compared with six cycles.66 Table 60-1 Adapted from www.fertilehope.org. In men with testicular cancers, combination chemotherapy is associated with FSH elevation and oligospermia. These findings are complicated further by the fact that the majority of patients with testicular cancer have abnormal spermatogenesis before the initiation of therapy. In 89 patients who were normospermic before chemotherapy, the postchemotherapy count was normospermic in 64%, oligospermic in 16%, and azoospermic in 20%. Clear evidence for recovery beyond 1 year was found, and the probability of spermatogenesis increased to 48% at 2 years and 80% by 5 years.67 Patients with pretreatment oligospermia or persistent FSH elevation 2 years after treatment are unlikely to recover normal spermatogenesis after treatment. Follicular growth and maturation are affected by chemotherapy through adverse effects on DNA function and prevention of cell division within ovarian cells. The risk of infertility is dependent on patient age, drug dose, and the duration and type of chemotherapy administered. Histologic evaluation of ovaries among women who have been treated with cytotoxic chemotherapy shows fibrosis and follicular destruction.68,69 Table 60-2 summarizes the risk of amenorrhea from commonly used cancer therapy regimens. Alkylating agents are strongly associated with ovarian dysfunction.70,71 Most series report a 50% or higher incidence of amenorrhea within 1 month of starting cyclophosphamide.72 Younger women are more tolerant of the effects of chemotherapy and have a better chance of resuming menstruation after completing chemotherapy.73 In one study among patients 30 to 40 years of age, a mean dose of 9.3 g of cyclophosphamide was associated with amenorrhea, whereas patients older than 40 years required a median dose of 5.2 g.74 A median of 20.4 g was required before the onset of amenorrhea in patients younger than 30 years.75 Menses resumed in 50% of patients younger than 40 years, and it rarely occurred in women older than 40 years.76 Other nonalkylating chemotherapies, such as antimetabolites, bleomycin, vinca alkaloids, and daunorubicin, are not a frequent cause of amenorrhea. Table 60-2
Reproductive Complications
Reproductive Physiology
Gonadal Form and Function
Hypothalamic-Pituitary-Gonadal Axis
Direct Effects of Cancer on Reproductive Function
Effects of Cancer Therapy on Sexual and Reproductive Function
Surgery
Prostate Cancer
Testicular Cancer
Rectal Cancer
Gynecologic Surgeries
Radiation Therapy
Central Nervous System Effects on Reproductive Function
Radiation Effects on Testicular Function
Radiation Effects on Ovarian Function
Pelvic Radiation as a Cause of Reproductive Dysfunction
Hormonal Therapy
Gonadotropin-Releasing Hormone Agonists and Antagonists
Antiandrogens
Endocrine Therapy and Breast Cancer
Chemotherapy
Effects in Men
Degree of Risk
Treatment
Common Usage
HIGH RISK
TBI
BMT/SCT
Prolonged azoospermia after treatment
Testicular radiation dose >2.5 Gy in men
Testicular cancer, ALL, NHL
Testicular radiation dose ≥ 6 Gy in boys
ALL, NHL, sarcoma, germ cell tumors
Protocols containing procarbazine: COPP, MOPP, MVPP, ChIVPP, ChIVPP/EVA, MOPP/ABVD, COPP/ABVD
Hodgkin lymphoma
Alkylating chemotherapy for transplant conditioning (cyclophosphamide, busulfan, melphalan)
BMT/SCT
Any alkylating agent (e.g., procarbazine, nitrogen mustard, cyclophosphamide) + TBI, pelvic radiation, or testicular radiation
Testicular cancer, BMT/SCT, ALL, NHL, sarcoma, neuroblastoma, Hodgkin lymphoma
Cyclophosphamide >7.5 g/m2
Sarcoma, NHL, neuroblastoma, ALL
Cranial/brain radiation ≥40 Gy
Brain tumor
INTERMEDIATE RISK
BEP × 2-4 cycles
Testicular cancer
Prolonged azoospermia not common at standard dose
Cumulative cisplatin dose <400 mg/m2
Testicular cancer
Cumulative carboplatin dose ≤2 g/m2
Testicular cancer
Testicular radiation dose 1-6 Gy (due to scatter from abdominal/pelvic radiation)
Wilms tumor, neuroblastoma
LOW RISK
Nonalkylating chemotherapy: ABVD, OEPA, NOVP, CHOP, COP
Hodgkin lymphoma, NHL
Temporary azoospermia after treatment
Testicular radiation dose 0.2-0.7 Gy
Testicular cancer
VERY LOW/NO RISK
Testicular radiation dose <0.2 Gy
Multiple cancers
No effects on sperm production
Interferon-α
Multiple cancers
Radioactive iodine
Thyroid
UNKNOWN RISK
Irinotecan
Colon
Bevacizumab (Avastin)
Colon, non–small cell lung
Cetuximab (Erbitux)
Colon, head and neck
Erlotinib (Tarceva)
Non–small cell lung, pancreatic
Imatinib (Gleevec)
CML, GIST
Effects in Women
Degree of Risk
Treatment Protocol
Common Usage
HIGH RISK
Whole abdominal or pelvic radiation doses ≥6 Gy in adult women
Whole abdominal or pelvic radiation doses ≥15 Gy in prepubertal girls ≥10 Gy in postpubertal girls
Multiple cancers
(>80% of women experience amenorrhea after treatment)
Wilms tumor, neuroblastoma, sarcoma, Hodgkin lymphoma
TBI radiation doses
BMT/SCT
CMF, CEF, CAF × 6 cycles in women 40+ yr
Breast cancer
Cyclophosphamide 5 g/m2 in women 40+ yr
Multiple cancers
Cyclophosphamide 7.5 g/m2 in girls <20 yr
NHL, neuroblastoma, ALL, sarcoma
Alkylating chemotherapy (e.g., cyclophosphamide, busulfan, melphalan) conditioning for transplant
BMT/SCT
Any alkylating agent (e.g., cyclophosphamide, ifosfamide, busulfan, BCNU, CCNU) + TBI or pelvic radiation
BMT/SCT, ovarian cancer, sarcoma, neuroblastoma, Hodgkin lymphoma Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access