Fig. 9.1
Anterior exenteration for a case of recurrent endometrial carcinoma treated primarily by radiation
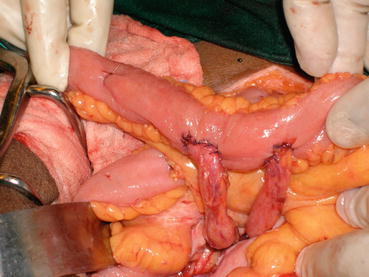
Fig. 9.2
Ileal conduit with ureteric anastomosis
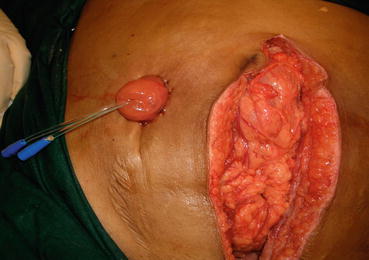
Fig. 9.3
Ileal conduit
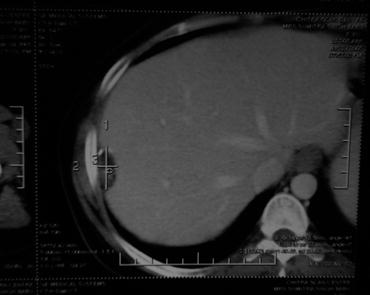
Fig. 9.4
Recurrence on liver surface in a case of papillary serous adenocarcinoma of endometrium

Fig. 9.5
Para-aortic nodal recurrence in endometrial carcinoma case after 3 years

Fig. 9.6
Complete retroperitoneal node dissection in endometrial carcinoma with isolated nodal recurrence
Cisplatin, Doxorubicin, Plus Paclitaxel
GOG 177 enrolled 273 women with previously untreated stage III/IV or recurrent endometrial cancer and randomized them to treatment with AP (cisplatin [50 mg/m2] plus doxorubicin [60 mg/m2] administered on day 1 every 3 weeks) or to TAP (doxorubicin [45 mg/m2 on day 1], cisplatin [50 mg/m2 on day 1] plus paclitaxel [160 mg/m2 over 3 h on day 2] every 3 weeks) [17]. Compared to AP, TAP resulted in:
Overall response rate (ORR) – 57 % vs 34 %
PFS – 8 months vs 5 months
OS −15 months vs 12 months
TAP – increased incidence of grade 3 neuropathy (12 % vs 1 %)
Carboplatin Plus Paclitaxel
GOG 209 (which was not included in the 2012 meta-analysis) administered carboplatin (area under curve = 6) plus paclitaxel (175 mg/m2) every 21 days and was compared to TAP in a trial that enrolled 1300 women with chemotherapy naive stage III, IV, or recurrent endometrial carcinoma [17]:
ORR – 51 % in both arms
PFS – 13 months in both arms
OS – 37 months vs 40 months (AP vs TAP)
A statistically significant reduction in the incidence of grade 2 or greater toxicity, including sensory neuropathy (19 % vs 26 %), thrombocytopenia (12 % vs 23 %), emesis (4 % vs 7 %), diarrhea (2 % vs 6 %), and metabolic derangements (8 % vs 14 %)
Second-Line Therapy
For women who have received adjuvant chemotherapy, the approach to second-line treatment depends on the interval between the end of adjuvant treatment and the diagnosis of relapse:
Greater than 6 months – repeat treatment with a platinum-based combination
Short treatment-free interval (<6 months) – single-agent therapy rather than a combination chemotherapy regimen. Commonly used agents include:
Doxorubicin
Ifosfamide
Ixabepilone
Docetaxel
Topotecan
Oxaliplatin
Novel Agents
BevacizumabRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree