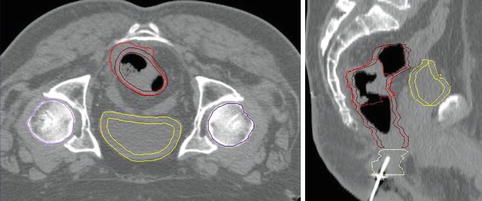
1.1 Contour of rectum (pale yellow) and anal canal (green). Radiopaque marker seen in the anal canal (3.3 cm long) and visualization of the anal margin (not contoured). The rectum appeared rather large probably containing stools
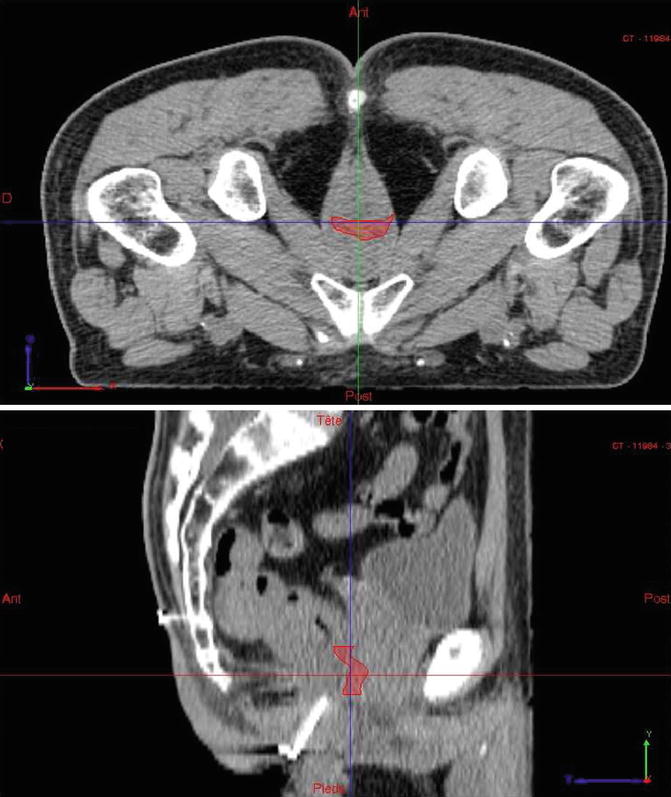
1.3 Rectal tumor contouring and positioning of GTV. Volume of tumor (GTV): 9 ccm
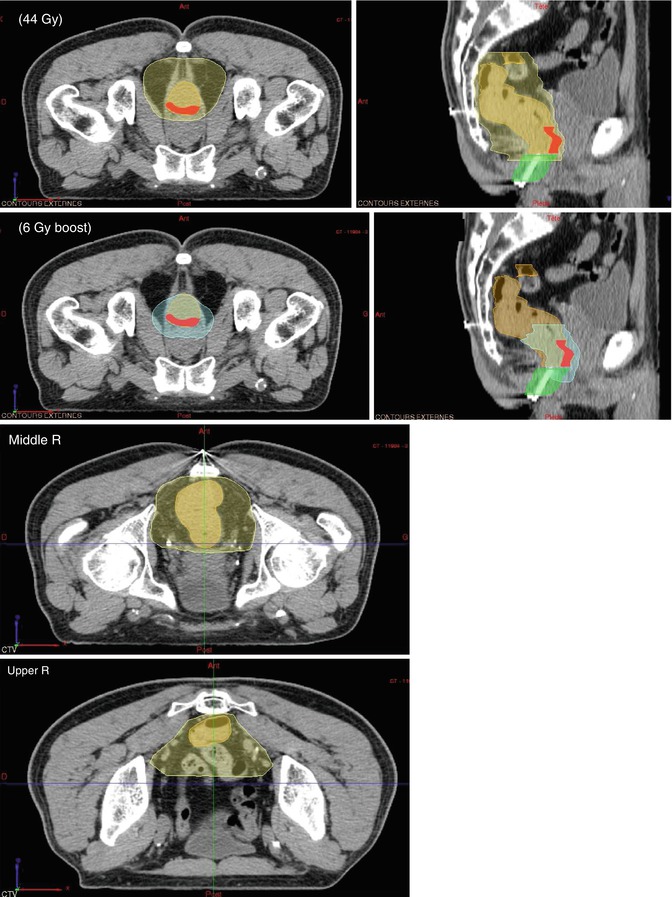
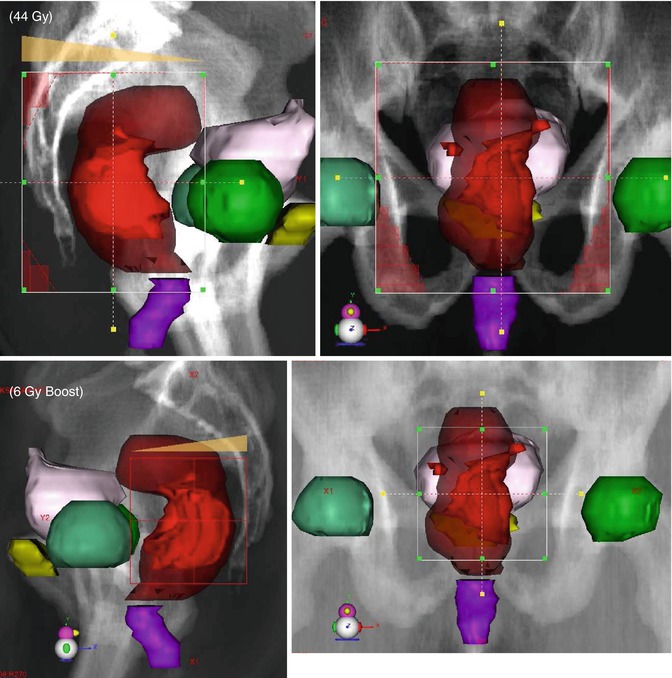
1.4 CTV contouring: CTV 44 Gy (sagittal view; axial view for low rectum with GTV, middle rectum, upper rectum); CTV boost 6 Gy (sagittal and axial views)
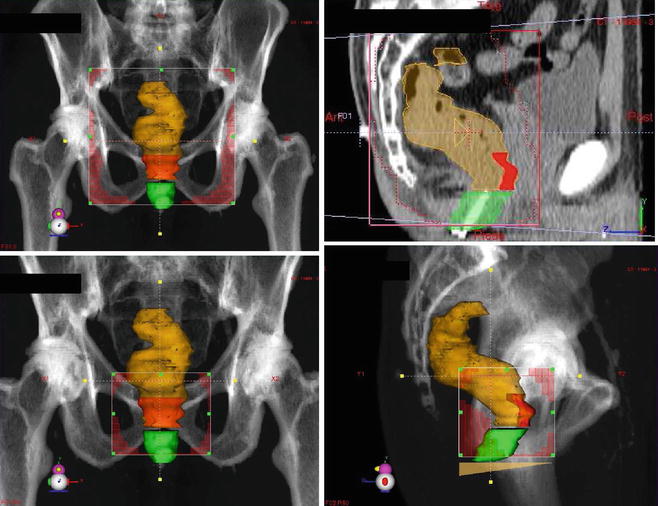
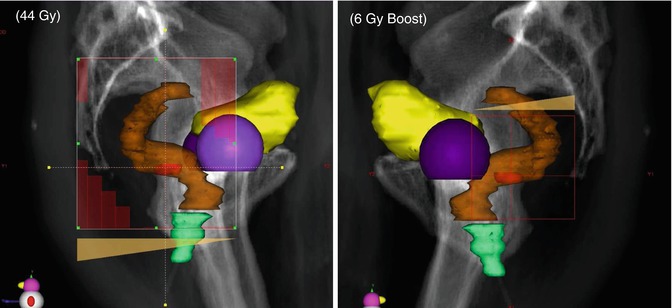
1.5 After PTV definition positioning of fields with MLC: lateral field and posterior field for initial 44 Gy; lateral field and posterior field for 6 Gy boost
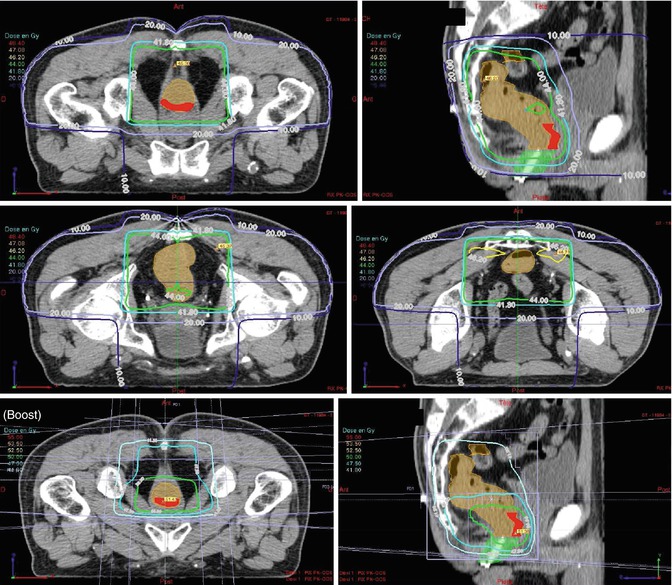
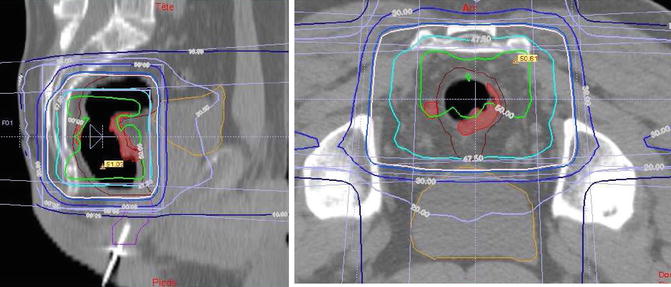
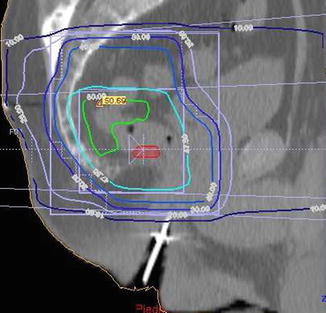
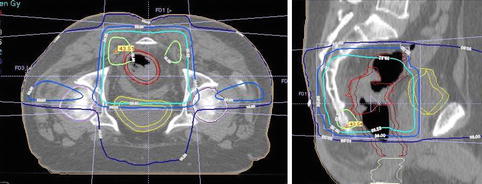
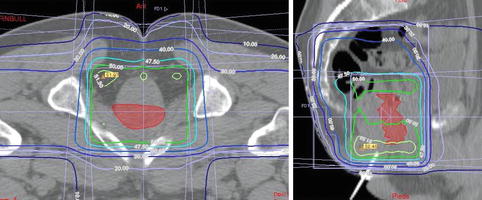
1.6 Isodose display for 44 Gy. Visualization of the 95 % isodose (relative to ICRU reference point) which corresponds to 41.8 Gy (turquoise color); sagittal view and axial view of low pelvis with GTV and middle and upper pelvis. In the upper plane, the external iliac arteries, which are calcified, can be easily seen (not included in the CTV due to their anterior location). On the opposite the hypogastric arteries (also calcified) are in the posterior pelvis and well in the CTV with no need for IMRT technique. Isodose display in sagittal plane for 6 Gy boost (95 % isodose, 5.7 Gy) and for 50 Gy. The turquoise isodose is the 41.8 Gy line which is the 95 % isodose relative to the 44 Gy prescription dose and reported for the ICRU point in the middle of the PTV
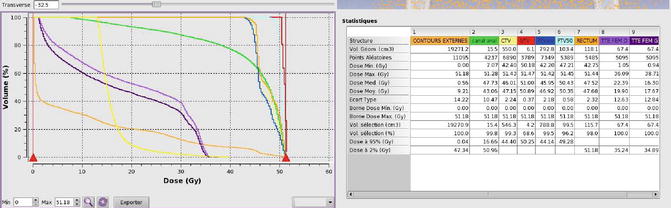
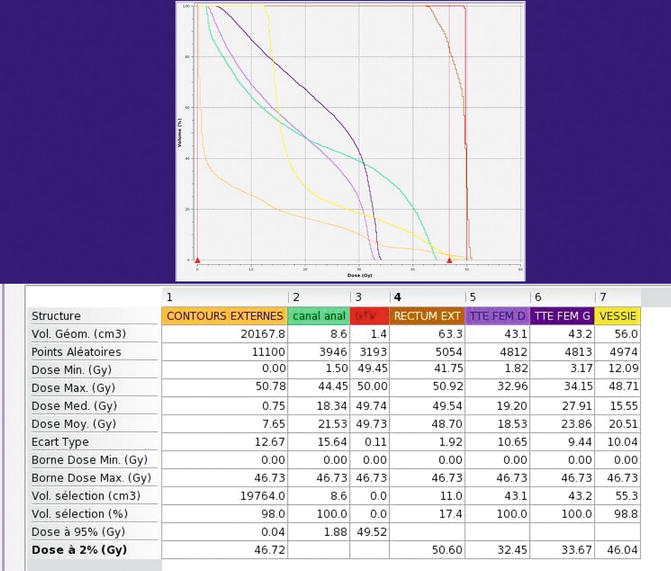
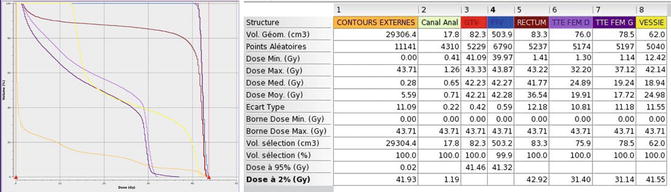
1.8 The DVH shows the following volumes: anal canal, 15.5 ccm; rectum, 118 ccm; GTV, 9 ccm; CTV, 550 ccm; isodose, 41.8 Gy (envelope isodose encompassing the PTV, 994 ccm). It can be seen that the upper boarder of the envelope isodose (PTV/CTV) is at the level of S2–S3 interspace. Most of the small bowel is above and receives only small doses
2.
T3 N1 – middle rectum (male patient, 57 years, tumor 70 % of circumference partly anterior with one node of 1 cm in diameter close to the tumor on the right side of the rectum, which was seen on MRI and palpable on DRE)
2.5 Positioning of fields with MLC: lateral and posterior fields for 44 Gy; lateral and posterior fields for 6 Gy boost
2.6 Isodose display for 50 Gy; sagittal and axial views through the tumor
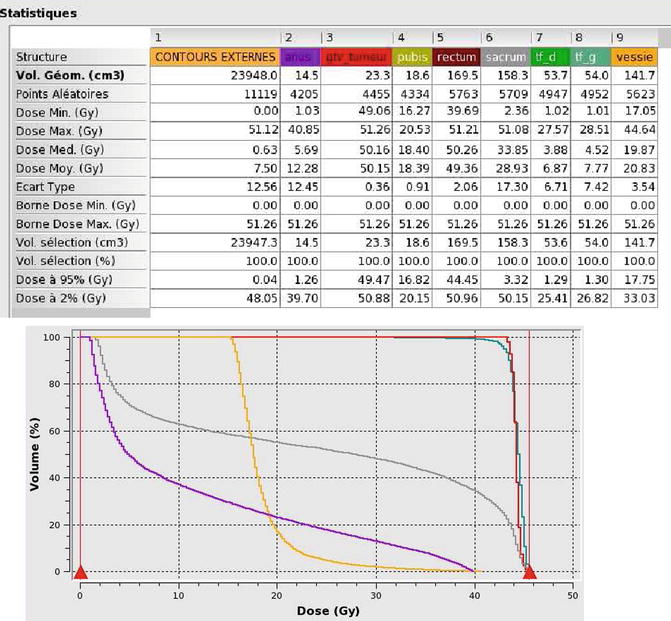
2.8 The DVH showed the following volumes: anal canal, 14.5 ccm; rectum, 169 ccm; GTV, 23 ccm; 95 % isodose of 44 Gy, 1,050 ccm
3.
T2 N0 – distal anterior rectum (male patient)
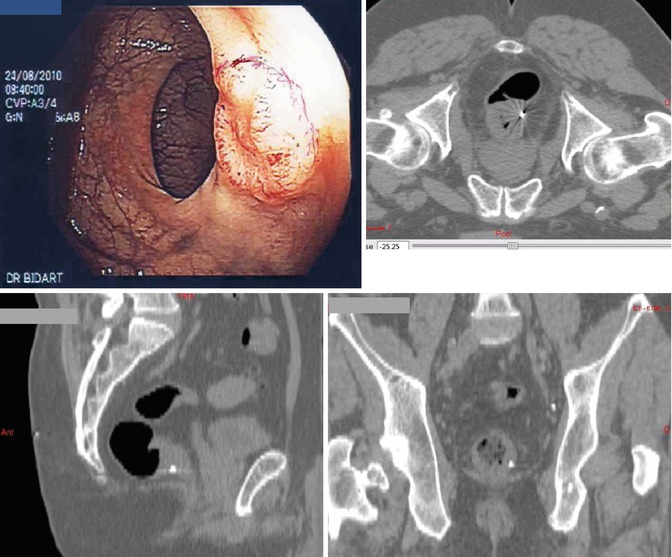
3.1 Endoscopic visualization of the tumor (2.5 cm in diameter). Radiopaque fiducial marker implanted at the lower limit of the tumor (patient prone)
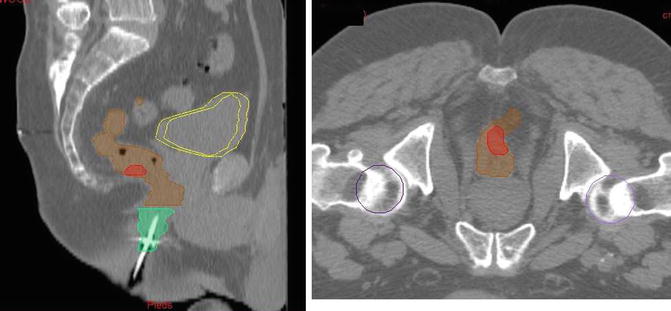
3.3 Rectal tumor (GTV) contouring with OAR (sagittal and axial views)
3.5 Positioning of fields with MLC. Lateral field for 44 Gy; lateral field for 50 Gy
3.6 Isodose display for 50 Gy (sparing of the anal canal; upper limit at S2–S3 interface)
3.8 DVH showing the following volumes: anal canal, 18 ccm; rectum, 63 ccm (small!); GTV, 1.4 ccm (small T2)
This 75-year-old patient referred by a surgeon for curative irradiation alone was treated with 50 kV X-ray contact brachytherapy: 110 Gy in 4 fractions, combined with EBRT (CAP 50 regimen derived from the ACCORD 12 trial). Two years later the patient was alive with local control and good bowel function.
4.
T4 NX – middle rectum (male patient, tumor fixed to the sacrum)
4.3 Rectum and OAR contouring. Contouring of the tumor (GTV) fixed to the left side of the sacrum (patient prone)
4.4 Positioning of fields with MLC. Lateral field for 44 Gy; lateral field for 50 Gy
4.6 Isodose display for 44 Gy (sagittal and axial views). Anal canal is spared; sacrum is fully encompassed, upper limit below S1–S2 interface. It would be easily possible to increase the dose to 60–64 Gy to a limited volume (<20 ccm) centered to the area where the tumor is fixed to sacrum with a risk of incomplete R1 or R2 resection
4.8 DVH showing the GTV of 82.3 ccm (“big” tumor)
5.
T4 N0 – distal rectum (male patient, tumor fixed to the prostate)
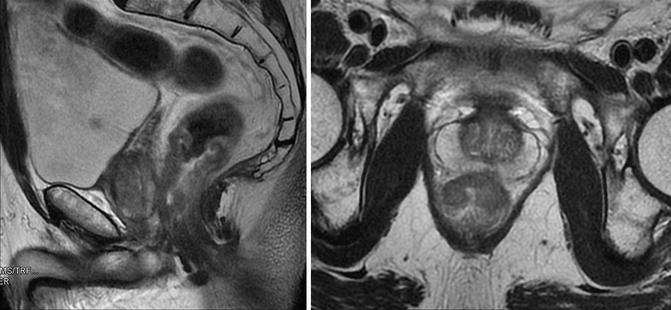
5.0 MRI showing a rectal tumor invading the prostate (sagittal and axial views)
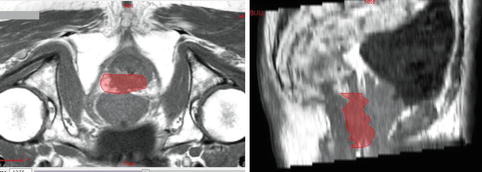
5.3 Rectal tumor (GTV) contouring with the help of image fusion (MRI + simulation CT scan). Axial and sagittal views. The tumor is infiltrating the posterior part of the prostate which was clinically obvious with a fixation on DRE
5.3 bis GTV = OAR contouring (rectum and prostate). Radiopaque marker in the anal canal
5.5 Field positioning with MLC. Lateral view (44 and 50 Gy)
5.6 Isodose display: lateral and axial views for 50 Gy. The anal margin is not in the treated volume (accurate positioning of isodose with the anal marker, prone position)
5.8 DVH showing the following volumes: prostate, 48.6 ccm; rectum, 197 ccm; GTV, 37.9 ccm
During surgery 6 weeks after administration of the CAP 50 regimen, a complete (R0) resection could be performed without removal of prostate tissue.
6.
Polypoid tumor adenocarcinoma T2 N0, 4.5 cm in diameter (“big polyp”). Middle anterior rectum. Tumor located just in front of a small bowel loop low in the pelvis after a previous hysterectomy. Patient had a traumatic fracture of sacrum after ski accident
6.3 GTV as seen on simulation CT scan (axial and lateral views). GTV contouring in red (axial and sagittal views)
6.5 Field positioning with MLC. Lateral view for 44 Gy
6.6 Isodose display. Sagittal view showing good protection of small bowel
Appendix 10.1
Volume of a sphere
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


