Fig. 28.1
The position of the incisions. (a) One 2 cm incision is made 1 cm above the sternal notch (a) or close to the position of the tumor (b). (b) The main transverse incision is made at the suprasternal notch and other incisions at the anterior margin of the sternomastoid muscle (Reproduced with permission from Shimizu K. Minimally invasive thyroid surgery. In: Best practice & research clinical endocrinology and metabolism, vol. 15, No. 2. Elsevier; 2001. p. 123–37)
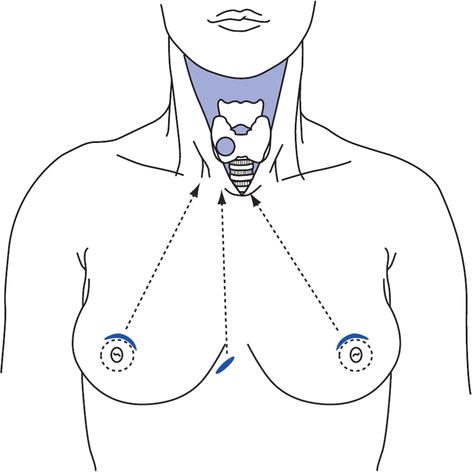
Fig. 28.2
Incisions along the mammary areola and at the parasternal site approaching the thyroid, indicated by dotted lines. The working space is created by carbon dioxide insufflation (Reproduced with permission from Shimizu K. Minimally invasive thyroid surgery. In: Best practice & research clinical endocrinology and metabolism, vol. 15, No. 2. Elsevier; 2001. p. 123–37)
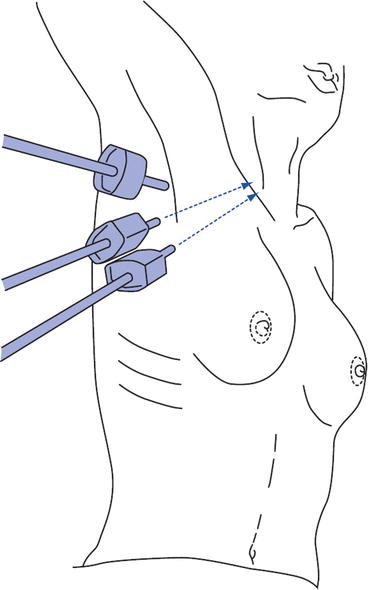
Fig. 28.3
Incisions at the axillary area. Three trocars and operative equipment are inserted through the wounds. The working space is obtained by carbon dioxide insufflation (Reproduced with permission from Shimizu K. Minimally invasive thyroid surgery. In: Best practice & research clinical endocrinology and metabolism, vol. 15, No. 2. Elsevier; 2001. p. 123–37)
Robotic Surgery
The use of robotic systems when operating on the thyroid gland has been developed in South Korea using the da Vinci three- or four-arm robot. There are now series of up 1,000 cases in the published literature and likely to be many more in the future as access to robotic surgery increases. Some argue the robot is better suited to the relatively confined space within the neck than laparoscopic instruments and, using specially designed retractors, has overcome many of the challenges in developing distant access surgery. Its use is being increased in North America and Europe. Surgical incisions are placed in the axilla, obviating the need for a neck incision (Fig. 28.4). There are no additional benefits to this approach however and wound morbidity may be increased due to the greater amount of dissection required as well as potential paresthesia to the upper chest.
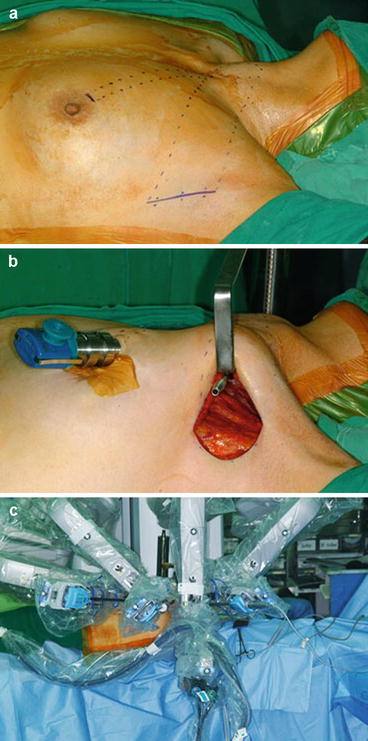
Fig. 28.4
Robotic thyroidectomy by a gasless unilateral axillobreast approach. (a) A 5–6-cm skin incision was made in the axillary fossa and a 0.8-cm incision was made on the circumareolar margin. (b) An external retractor was used to maintain the working space without CO2 gas insufflation. In the axillary port, an endoscope was placed in the center and two robotic arms were placed on either side of the endoscope. The fourth arm of the da Vinci S robot was placed through the breast port for retraction of the thyroid gland with Prograsp. (c) The view after placement of the four robotic arms (Reproduced with permission from Tae K, et al. Robotic thyroidectomy by a gasless unilateral axillo-breast or axillary approach: our early experiences. Surg Endosc. 2011;25:221–8, Springer)
In both minimal access and robotic surgery:
Access should not impair the surgical objectives.
Care should be taken with patient selection, particularly in obese patients or those advanced cancers or retro sternal goiter.
A consideration of additional costs should be made.
There may be increased length of hospital stay secondary to prolonged general anesthesia.
Surgical Equipment
Reducing bleeding intraoperatively and postoperatively has been a desirable objective and leads to a number of advances in all surgical fields. Much of the advancement has come from laparoscopic technology. There is increasing use in thyroid surgery of devices that coagulate and cut simultaneously including ultrasonic or harmonic scalpels and bipolar cutting devices. In some centers these devices have superseded traditional ligatures or diathermy techniques and are particular beneficial if access is limited, for example, when ligating the upper pole. Charring is minimal and the degree of heat transferred to lateral tissues is reduced. This has advantages when operating close to the laryngeal nerves and parathyroid glands. Use of the harmonic scalpel has been linked to significantly decreased surgical time as well as improved postoperative pain. Many also advocate the use of these devices to reduce operative time allow the surgeon to approach more challenging parts of the operation with less fatigue.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


