Quality Improvement for Healthcare Epidemiology: Creating a Culture of Excellence
Quality Improvement for Healthcare Epidemiology: Creating a Culture of Excellence
Julia E. Szymczak
DEFINING QUALITY IMPROVEMENT IN HEALTHCARE
It has been 20 years since the Institute of Medicine (IOM) published two landmark reports on patient harm and inconsistent healthcare quality in the United States: To Err Is Human: Building a Safer Health System (1999) and Crossing the Quality Chasm: A New Health System for the 21st Century (2001).1,2 The former report contained disturbing figures. At least 44 000 and perhaps as many as 98 000 people die in U.S. hospitals each year as a result of preventable medical errors. At the time, these numbers exceeded the numbers of deaths attributable to other public health threats such as breast cancer, human immunodeficiency virus (HIV), and car accidents. Beyond the loss of life, preventable medical errors were seen to exact other substantial tolls on society including total costs ranging from $17 to $29 billion, loss of public trust in the healthcare system, widespread burnout among the health professions, and overall lower levels of population health and well-being.
Crossing the Quality Chasm demonstrated that the U.S. healthcare system failed to deliver the consistent, highquality care that all Americans deserved. Beyond direct patient harm, the report documents a gap between care that is based on the best scientific knowledge and what people actually receive. The authors of the report put it bluntly “Indeed, between the healthcare that we now have and the healthcare that we could have lies not just a gap, but a chasm.”2 A number of complex factors interacted to create this chasm: rapidly advancing biomedical knowledge and technology, increased life expectancy, and increased prevalence of chronic diseases resistant to traditional therapeutic approaches used for acute, episodic conditions. Fundamental reinvention of the healthcare system was needed, they argued, in order “to continually reduce the burden of illness, injury, and disability, and to improve the health and functioning of the people of the United States.”2
Notably, these reports focused on medical error and low-quality care as a function of broken systems and not recklessness on the part of individual healthcare professionals.3 Adverse events in medicine were the result of faulty processes of care and work conditions that led people to make mistakes or fail to prevent them, instead of the result of malicious individuals intent on causing harm. The vast majority of healthcare professionals come to work each day wanting to provide the absolute best care possible but encounter obstacles to consistently achieving this goal. Improving care requires a redesign of the system at all levels to make it harder for people to do something wrong and easier for them to do it right.4 It also requires a cultural change in how we think about, talk about, and make sense of adverse events in healthcare.
TABLE 8-1 IOM Six Aims of Healthcare Quality
Dimension
Definition
Safe
Avoiding injuries to patients from the care that is intended to help them.
Effective
Providing services based on scientific knowledge to all who could benefit and refraining from providing services to those not likely to benefit.
Patient-centered
Providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions.
Timely
Reducing waits and sometimes harmful delays for both those who receive and those who give care.
Efficient
Avoiding waste, including waste of equipment, supplies, ideas, and energy.
Equitable
Providing care that does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status.
Institute of Medicine (IOM). Crossing the Quality Chasm: A New Health System for the 21st Century, 2001.
To Err Is Human and Crossing the Quality Chasm stimulated profound changes in healthcare practice, policy, and oversight in the United States and around the globe. In the intervening two decades, much progress has been made, as the field of quality improvement science in healthcare has expanded rapidly.5 While there is no one agreed-upon definition of “quality” in healthcare, the IOM has identified six aims that should underpin efforts to improve care, as specified in Table 8-1.
The modern healthcare epidemiologist and infection preventionist are engaged in work that addresses many of these aims at once.6 Infection prevention seeks to avoid harm to patients from care that is intended to help them. Preventing the transmission of infection in healthcare settings involves attention to individual behavior, the dynamics of groups, the physical environment, and systems of care at all levels. Antibiotic stewardship seeks to provide treatment to patients based on the best scientific evidence to those who are most likely to benefit while refraining from providing treatment to those not likely to benefit. Promoting the judicious use of antibiotics requires behavioral change, effective communication, robust health information technology systems, and the promotion of evidencebased practice across diverse groups of professionals. The outcomes of infection prevention and antibiotics stewardship are patient-centered. Achieving them leads to more timely, efficient, and equitable care. As such, those working in healthcare epidemiology should be familiar with key principles and tools of quality improvement.
KEY PRINCIPLES OF QUALITY IMPROVEMENT IN HEALTHCARE: DATA, UNDERSTANDING SYSTEMS, AND ENGAGEMENT
The field of quality improvement in healthcare is vast, and there are a multitude of specific approaches, tools, and methods that one can use to change the way care is delivered to achieve better outcomes for patients. A novice can get lost in terminologies, acronyms, concepts, and specific methodologies. The intent in this chapter is not to exhaustively review all of them but, instead, to provide the reader with a synthesis of core principles that cut across approaches. At the end of the chapter, we have provided a list of resources, organizations, and readings that can be utilized for a more in-depth understanding of this diverse and varied field.
Data for Improvement
Data are the bedrock of any healthcare quality improvement method.7 The purpose and use of data in a quality improvement context are different than a research context, in which scientists gather data with the primary goal of testing hypotheses to produce generalizable knowledge.4 In quality improvement, data itself are part of the change process. This means that the hypothesis changes as the system improves, a concept that is antithetical to scientific research. Data for quality improvement have to be good enough to allow us to know whether an intervention is working in a given setting. They do not have to be created with the goal of reproducibility or generalizability across settings. Data for research must be gathered with great care and thoroughness, which can take a long time. Data gathering for quality improvement must balance efficiency with thoroughness.8
In the quality improvement context, data are powerful because they stimulate learning about the present state of a system and provide information about whether an improvement has actually occurred as the result of an intervention and whether that change is sustained over time. Because humans may under- or overestimate the performance of a system based on their own cognitive biases, data serve an important function in separating what people think is happening in a system from what is actually happening. In this way, data can serve a powerful psychological purpose by helping people understand that a change is needed. Data on their own can be compelling; however, care should be taken by those engaging in quality improvement work to provide context for data with a clear communication plan.9 The plan should communicate were the data come from, why they were gathered, and what interpretations should be drawn from them.
Both quantitative and qualitative data are important components of all quality improvement methods. Quantitative data are composed of numbers obtained using a quantifiable measurement process. These data can be analyzed using statistical methods. Common sources of quantitative data in healthcare quality improvement include information gathered from the electronic medical record (eg, number of visits where an antibiotic was ordered for a condition in which antibiotics are not needed) or observation of practice (eg, percent compliance with hand hygiene indications during an episode of care). Qualitative data are composed of words, phrases, and visual images. These data have descriptive rather than numeric properties and cannot be used to draw statistical inferences. Qualitative data contain knowledge about perceptions, beliefs, processes, patterns of behavior, and the influence of context on an outcome.9,10 Common sources of qualitative data in healthcare quality improvement include interviews, focus groups, free-text responses to a survey, or observations of group behavior.
Understanding Systems and Processes
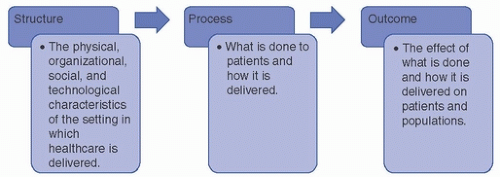
As described earlier, To Err Is Human made an important contribution to our understanding of medical error and low-quality care by emphasizing how these outcomes are produced by a faulty system. Solutions to improve healthcare needed to move away from “blaming and shaming” of individuals toward understanding and repairing clinical work systems.11,12 The field of healthcare quality improvement has predominantly utilized the Donabedian model to assess the quality by understanding systems.13 Developed in 1966 by Avedis Donabedian, a physician and health services researcher, the model suggests that care delivery systems can be understood as the relationship between structure, process, and outcome, as illustrated in Figure 8-1.
In order to improve the quality of care delivered in a system, ideally both structures and processes must be addressed together. Measurements are needed to understand the system. Each element in the model corresponds to a measurement that reflects whether and how change has occurred in an improvement effort.14
Structure measures reflect the physical, organizational, social, and technological characteristics of the healthcare setting. Examples of structure measures include nurse-patient ratios, hospital safety climate, the number of full-time equivalents (FTE) devoted to supporting infection prevention staff, and availability of an electronic medical record.
Process measures reflect the way a system works to deliver a patient outcome. Examples of process measures include compliance with techniques that are thought to produce a desired outcome, such as hand hygiene, proper care of a central line insertion site, elevation of the head of a patient’s bed, and quality of terminal room disinfection.
Outcome measures reflect the impact of a process on a patient. They are arguably the most important measure in quality improvement since they directly reflect what has happened to the patient as a result of the care she has received, but they can sometimes be difficult to define and may take time to assess. Examples of outcome measures include rates of healthcareassociated infections, mortality, length of stay, and patient satisfaction.
FIGURE 8-1 The Donabedian model for quality of healthcare.
Systems are composed of processes, as the Donabedian model makes clear. To improve the quality in healthcare, we need not only to measure moments in a process but to create a visualization of what is done (care provided) and how it is done (when, where, and by whom care is delivered). Process mapping is an approach that originated in the field of engineering and has been widely utilized in healthcare quality improvement.15 A process map, also known as a flowchart, is a visual representation of the steps that comprise an episode of care. The work of creating a process map can help organizations to identify areas in particular need of improvement or weakness. It is also an opportunity for key stakeholders to come together and build consensus. Examples of processes that healthcare epidemiologists might find useful to map include central line insertion, the way restricted antibiotics are approved, how hospital visitors are screened for illness during influenza season, and the manner in which patients are identified for contact isolation status. The steps used in creating a process map are described in Table 8-2.16
Considering Culture: Engaging Staff
While data, measurement, and a thorough understanding of workflow processes are necessary to improve the quality of healthcare delivered to patients, these elements are not enough to produce and sustain change. There is an oft-cited aphorism in management that epitomizes the importance of social dynamics in producing organizational success: culture eats strategy for breakfast. A company can have an elaborate plan about how success will be produced, sophisticated technologies, and scientific knowledge about a particular organizational process. Yet that company can fail to achieve success by not taking into account how that plan will be received by the groups of people whose actions are critical for producing successful organizational outcomes.
Only gold members can continue reading. Log In or Register to continue
Jun 8, 2021 | Posted by drzezo in INFECTIOUS DISEASE | Comments Off on Quality Improvement for Healthcare Epidemiology: Creating a Culture of Excellence
 Role of the Microbiology Laboratory and Molecular Diagnostics in Healthcare Epidemiology and Infection Prevention
Role of the Microbiology Laboratory and Molecular Diagnostics in Healthcare Epidemiology and Infection Prevention
 Healthcare-Associated Bloodstream Infections (Non-device related)
Healthcare-Associated Bloodstream Infections (Non-device related)



