Although the physiologic reserve of the respiratory system declines with age, dyspnea with usual activity is abnormal and should trigger an investigation for underlying disease.
The perception of dyspnea appears to be blunted in the elderly and may delay seeking medical attention.
An alveolar-to-arterial oxygen gradient of 20 to 25 mm Hg is the upper limit of normal in any population, and a higher gradient in the elderly patient warrants further evaluation.
The most common causes of cough include postnasal drip, cough-variant asthma, chronic bronchitis, and gastroesophageal reflux disease. Therapy should be directed at the underlying mechanism following diagnostic evaluation.
The differential diagnosis of asthma in the elderly is broad and often overlooked.
Asthma may present at any age.
The negative predictive value of methacholine challenge testing is higher than the positive predictive value, so that it is more useful in ruling out a diagnosis of asthma than establishing one.
Special treatment considerations in the elderly with asthma and chronic obstructive pulmonary disease include a higher risk of adverse effects of medication and exacerbation of coexistent disease, medical noncompliance, and precipitation of bronchospasm by commonly used medications for comorbid illness.
Although a number of medications are indicated for symptomatic relief in chronic obstructive pulmonary disease, smoking cessation and supplemental oxygen therapy are the only therapies shown to favorably impact outcome.
Elderly patients with pneumonia often present with nonspecific symptoms and may not manifest the classic constellation of fever, dyspnea, and cough. This may lead to delayed diagnosis or misdiagnosis and a greater mortality risk.
Initiation of appropriate antibiotic therapy for pneumonia within the first 8 hours of presentation has been shown to significantly reduce mortality.
Prevention may be the best way to reduce the morbidity and mortality associated with pneumonia in the elderly. Recommended immunizations include the 23-valent pneumococcal polysaccharide and influenza vaccines.
Because of the waning of cell-mediated immunity, the two-step purified protein derivative skin test is recommended in those elderly with an initial nonreactive test result.
The risk of isoniazid-induced hepatitis is low. Therefore, isoniazid-based treatment regimens are recommended for the treatment of both latent and active tuberculosis in the elderly.
Sleep patterns change with normative aging, and sleep disturbances such as insomnia, nocturnal awakening, and sleep-disordered breathing appear to be more common in the elderly population. Their clinical significance is unclear.
in origin. A thorough history including acuity of onset, exacerbating factors such as exertion and positional change, and associated symptoms are vital in determining the etiology of dyspnea. Abrupt onset points to relatively acute processes such as pulmonary infection, pulmonary embolism (PE), and congestive heart failure (CHF). Subacute or chronic presentations of dyspnea are more likely to be indicative of underlying chronic bronchitis, emphysema, interstitial lung disease (ILD), or chronic CHF. Dyspnea may occur at rest or may only be apparent on exertion. In making an assessment of the severity of chronic dyspnea, it is important that the practitioner ask the patient “what are your usual daily activities?” and “what activities have you had to discontinue recently?” because patients often reduce activities to minimize discomfort.4
TABLE 30.1 COMMON CAUSES OF DYSPNEA | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||
histamine-2 (H2) blockers and proton pump inhibitors. Symptomatic treatment with antitussive agents such as dextromethorphan, and narcotics such as codeine is useful to supplement specific therapy, but is ineffective alone.
TABLE 30.2 MAJOR CAUSES OF HEMOPTYSIS | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Mean bronchiolar diameter, the main determinant of airways resistance, has been found to decrease significantly after age 40.21 This change is thought to be the result of alterations in the collagenous matrix and elastic components of the underlying connective tissue, which support the airways, tethering them open.20 With age, the alveolar ducts become enlarged, and the alveolar sacs shallower, resulting in a decrease in the airspace surface area-to-lung volume ratio.22 In addition, there is some evidence that changes in the alveolar basement membrane composition and, thickness may also occur with aging.5,20 Taken together, these changes contribute to a decline in the measured DLCO. This decline occurs later in women than in men, perhaps secondary to estrogen effects.5,20
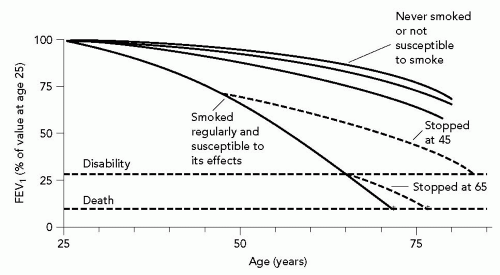 Figure 30.1 Decline in lung function with aging. As depicted in this graph, forced expiratory volume in 1 second (FEV1) decreases over time with normative aging. In susceptible smokers, the rate of decline in FEV1 has a much steeper slope. After smoking cessation, the rate of decline reverts to that of a nonsmoker. (From Fletcher C, Peto R. The natural history of airflow obstruction. Br Med J. 1977;1:1645-1648. Graph reproduced with permission from the BMJ Publishing Group). |
In these individuals, there is often a significant drop in TLC and a resultant restrictive defect. Just as RV increases with aging, so does functional residual capacity. Therefore, the small airways (terminal bronchioles) close early, especially in the dependent parts of the lung, leading to V/Q mismatching and increased dead space ventilation. These contribute to the increase in the alveolar-to-arterial oxygen gradient (A-a gradient).5,20
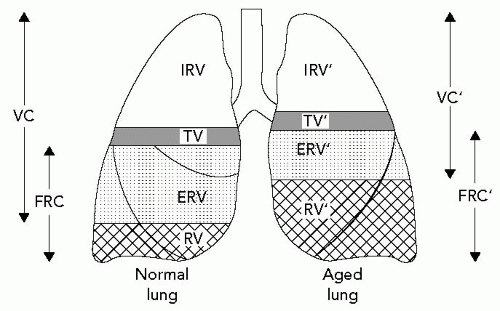 Figure 30.2 Changes in lung volume associated with aging. As depicted above, vital capacity (VC) decreases with aging. Correspondingly, residual volume (RV) and functional residual capacity (FRC) increase so that total lung capacity (TLC) does not significantly change. TV, tidal volume; IRV, inspiratory reserve volume; ERV, expiratory reserve volume. (From Chan ED, Welsh CH. Geriatric respiratory medicine. Chest. 1998;114:1704-1733. Reproduced with permission from Chest). |
 |
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


