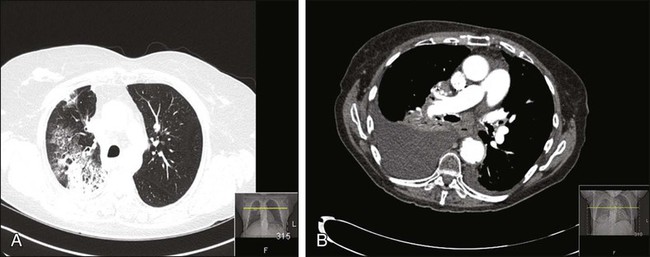
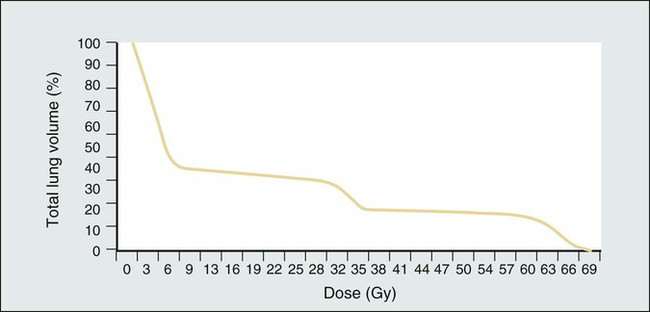
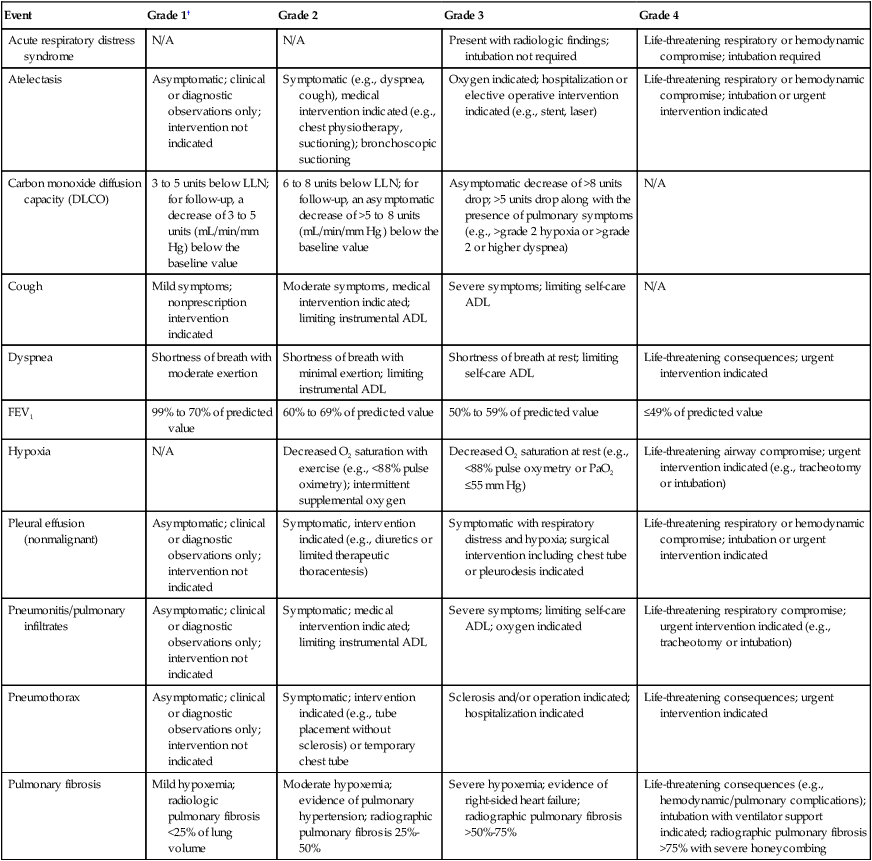
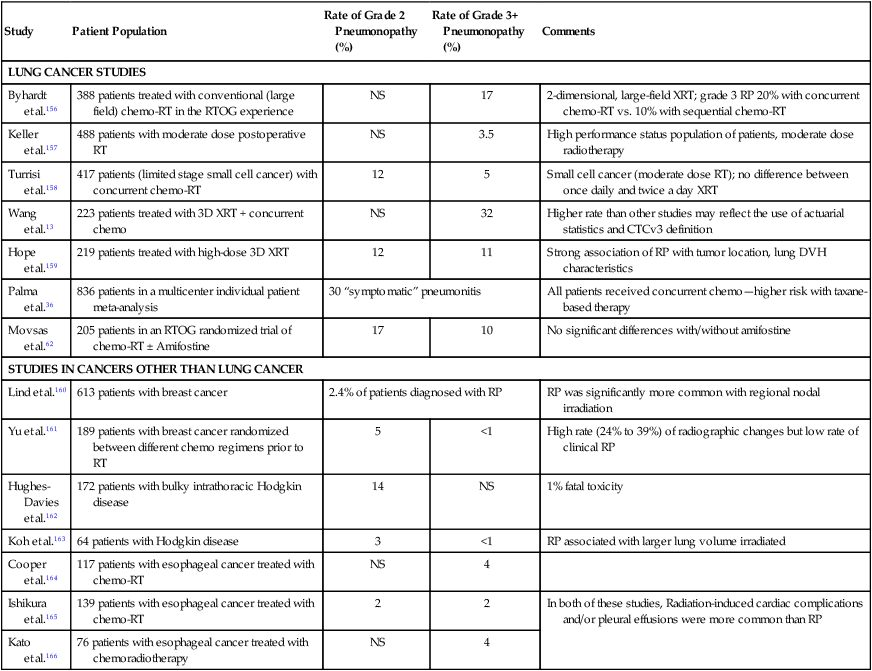
Neelesh Sharma, Ellen Kim and Mitchell Machtay Radiation-Induced Lung Injury (Radiation Pneumonitis and/or Fibrosis) • Risk factors include radiation dose and volume of lung irradiated, which may be expressed as mean lung dose or as the Vx, that is, the percentage of normal lung tissue irradiated to a dose above a certain threshold dose. • Older age, co-morbidities (including chronic obstructive pulmonary disease), and/or low performance status are risk factors. • The location of the tumor is a risk factor; irradiation of lower lobe primary lung tumors may carry a higher risk than irradiation of other tumors, although this may reflect the higher volume irradiated with lower lobe tumors. • Biological factors can carry risk, including levels of circulating cytokines such as transforming growth factor–β and interleukin-6. • The predominant symptoms are dyspnea and hypoxia, especially upon exertion. • Fever (usually low grade if present at all), cough, pleuritic chest pain, and other pulmonary symptoms also frequently occur. • Diffusing capacity of the lung for carbon dioxide is the most sensitive pulmonary function. • Interstitial or ground-glass infiltrate usually corresponds to the irradiated volume. • Findings at bronchoscopy are unremarkable (bronchial lavage may reveal lymphocytosis). • Pulmonary embolism, infection, and progressive tumor must be ruled out. These conditions can co-exist with radiation pneumonitis. • Response to corticosteroids is usually relatively rapid. • Prevention is far more important than treatment. Patients must be selected carefully for thoracic radiation, and irradiated volumes must be limited. • Corticosteroids are very useful in the management of acute and subacute pneumonitis (although they have no prophylactic or therapeutic value in the management of long-term radiation fibrosis). • A pulmonologist should be consulted for all grade 3 cases and most grade 2 cases. • Oxygen should be administered as indicated to prevent hypoxia. • High doses of corticosteroids (60 mg/day of prednisone) should be administered with slow tapering (over several weeks to months) for severe grade 2 or any grade 3 radiation pneumonitis. • If prolonged corticosteroid treatment is anticipated, prophylaxis against corticosteroid complications is needed, including gastrointestinal, infectious, and osteoporosis prophylaxis and dietary and pharmacologic management of hyperglycemia. • Antibiotics, bronchodilators, diuretics, and anticoagulation should be used as indicated for co-existing cardiopulmonary illnesses. • Usually, bleomycin, nitrosoureas, and mitomycin or combinations of several potentially pneumotoxic agents that on their own may only have modest pneumotoxicity (e.g., gemcitabine and weekly docetaxel) are risk factors. • Bone marrow transplantation/high-dose chemotherapy with or without total body irradiation is a risk factor. • Concurrent or recent thoracic radiation therapy is a risk factor. • Poor baseline pulmonary function is a risk factor. • Dyspnea and hypoxia are predominant, but a wide range of possible symptoms exists. • Interstitial or ground-glass infiltrate usually is diffuse throughout both lungs and may be worse in the lower lobes. • Findings at bronchoscopy are unremarkable (bronchial lavage may reveal lymphocytosis). • Pulmonary embolism, infection, and progressive tumor must be ruled out and may co-exist with drug-induced lung injury. • Injury is usually (but not universally) responsive to corticosteroids; it is less likely to respond well to steroids than radiation pneumonitis but more likely to respond well than late radiation fibrosis. • When the diagnosis is suspected, the suspected causative agent should be discontinued. • Consultation with a pulmonologist is necessary. • Oxygen should be administered as indicated to prevent hypoxia (high fraction of inspired oxygen levels may be dangerous in bleomycin-related pneumonopathy). • High doses of corticosteroids (≥60 mg/day of prednisone) with slow taper may be needed for severe grade 2 or any grade 3 pneumonitis. • If prolonged corticosteroid treatment is anticipated, prophylaxis against corticosteroid complications entails gastrointestinal, infectious and osteoporosis prophylaxis and dietary or pharmacologic management of hyperglycemia. • Antibiotics, bronchodilators, diuretics, and anticoagulation should be administered to manage co-existing cardiopulmonary illnesses. Thoracic radiation is probably the most important cause of pulmonary toxicity in oncology. Lung toxicity from radiation is a clinically relevant issue for lymphoma, breast cancer, bone marrow transplantation (BMT), esophageal cancer, and lung cancer. Figure 58-1 illustrates two different cases of radiation pneumonitis and its sequelae. The mechanisms behind radiation-induced lung injury remain poorly understood despite decades of study. A detailed review of the histopathological and molecular events occurring in radiation pneumonopathy is beyond the scope of this chapter; several excellent reviews have been published in the past decade.3–3 Irradiation damages endothelial cells, epithelial cells (particularly surfactant-producing type II pneumocytes), and reticuloendothelial cells within the lung through several mechanisms, including apoptosis and induction of stress-response genes. It is now generally agreed that cytokines such as transforming growth factor beta (TGF-β) play a major role in promoting radiation pneumonopathy, including development of long-term fibrosis.4,5 It can be difficult histopathologically (or molecularly) to differentiate established radiation lung injury from other forms of end-stage lung disease, such as idiopathic pulmonary fibrosis, drug-induced injury, or even very advanced chronic obstructive pulmonary disease (COPD). In most cases, radiation lung injury is confined to the regions of the lung within the radiation field or portal. This conventional wisdom has been challenged by several researchers who have found evidence of “out-of-field” radiation injury, which may be manifested in a syndrome similar to bronchiolitis obliterans with organizing pneumonia.6 In the most severe cases, diffuse acute respiratory distress syndrome can result from partial lung irradiation even with steroid treatment.7 Autoimmunity has been hypothesized as a mechanism of out-of-field radiation lung injury, with the possibility that localized lung damage triggers diffuse lymphocyte-mediated hypersensitivity against pulmonary self-antigens.8 Radiation lung injury may have any of a variety of clinical and radiographic presentations, but the hallmark symptom is dyspnea out of proportion to other findings. The most common imaging finding is an interstitial infiltrate corresponding to the radiation portals, but it is not unusual to find consolidation, nodularity, or even pleural effusions. The extent of radiographic findings does not necessarily correlate with the extent of symptoms or the patient’s clinical course.9 This problem can make the differential diagnosis among recurrent/progressive cancer, infection, and radiation lung injury extremely difficult, particularly in patients with lung cancer. Positron emission tomography with fluorodeoxyglucose may be helpful for differentiating recurrence from radiation toxicity, although intense radiation pneumonitis and even actively developing fibrosis causes elevated fluorodeoxyglucose uptake.10 The most important factor influencing development of clinically relevant radiation lung injury is the volume of lung irradiated; this issue is extensively discussed in the radiation oncology literature.11–15 In radiation oncology, the lung is considered a parallel-architecture organ, meaning that destruction of very small portions of it should not cause overall organ dysfunction. This belief is supported by the fact that wedge resection of a small portion of lung tissue or stereotactic radiosurgery to a very small lung tumor is well tolerated by most patients. In contrast, other organs, such as the spinal cord, are considered series-architecture organs, in which destruction of one region will lead to irreversible dysfunction downstream from that injury.16 The series-architecture model of radiation-induced toxicity does apply to other tissues within the lung, such as major bronchi and/or pulmonary vessels, where the result of injury to a small volume can be catastrophic (e.g., fistula and massive hemorrhage).17 The percentage of lung irradiated is often expressed by radiation oncologists as the “Vx,” where x = a certain dose in Gy. V20 indicates the percentage of a patient’s total lung volume that was irradiated to a dose of at least 20 Gy. Mean lung dose (expressed in Gy) is another parameter commonly used to express the extent to which a patient’s lung volume has been irradiated. Most clinical trials for locally advanced lung cancer require that the V20 be under a certain threshold, such as 35%. However, no single parameter can express the total radiation exposure, which is best described by a two-dimensional graphical curve called a dose-volume histogram (Fig. 58-2 provides an example). Irradiation of the entire lung volume (bilateral lungs) is uncommon today, except as part of total body irradiation for selected BMT conditioning regimens. As reviewed by Sampath and colleagues,18 the therapeutic index for whole-lung irradiation is extraordinarily narrow and highly dependent on total dose, fractionation, partial lung transmission shielding, and dose rate. A typical dose of 12 Gy total body irradiation has an approximately 11% rate of severe pneumonitis, compared with approximately 2% when lung transmission shielding is used to reduce the lung dose to 6 Gy. At the other extreme, irradiation of small lung volumes, as with stereotactic body radiation therapy (SBRT, also known as radiosurgery) for early-stage non–small cell lung cancer (NSCLC) rarely results in high-grade RP, despite its use in a compromised patient population.21–21 The field of SBRT for lung cancer is evolving very quickly, and it is likely that with longer follow-up of patients, a greater understanding of the similarities and differences from conventional external beam radiation therapy (XRT) with regard to toxicity will be achieved. In tangential irradiation of the breast (after lumpectomy) or chest wall (after mastectomy), the risk of clinically significant RP is approximately 1%, increasing to approximately 5% with the addition of irradiation of the regional (axillary/supraclavicular) nodes.22 An association between dose-volume irradiated and pneumonitis risk has also been shown in patients treated for esophageal carcinoma.23 Level I evidence of a strong relationship between pneumonopathy and the volume irradiated comes from a randomized trial from China.24 This study showed that the incidence of RP was significantly reduced from 29% to 17% with the use of “involved-field” radiotherapy, despite the use of higher tumor radiotherapy doses in the involved field arm. Understanding the true incidence of radiation pneumonopathy is complicated by multiple factors, including ambiguities in scoring,26 uncertainties related to concurrent medical conditions, and limitations of the historical and current standards for defining and grading this illness.25 Kocak and colleagues25 found that 28% of their suspected RP had confounding medical conditions that made the clinical diagnosis uncertain. Yirmibesoglu and colleagues26 concluded that 48% of RP cases were “hard to score” (vs. “unambiguous”) because of confounding factors (e.g., tumor progression, acute exacerbation of COPD, and infection). The traditional scoring system developed by the Radiation Therapy Oncology Group (RTOG), which dates back to the early 1970s, is shown in Table 58-1.27 This system is no longer generally used because of limitations such as an arbitrary cutoff of 90 days between acute and late radiation lung injury28; however, understanding of this system is important because numerous publications rely on it. Modern toxicity scoring is performed according to the Common Terminology Criteria (CTC), currently at version 4 (CTCv4).29 The CTCv4 definitions and grading for select pulmonary events are shown in Table 58-2. A comparison of CTCv3 or the old RTOG criteria to CTCv4 shows that numerous changes have been made to the scoring criteria in the pulmonology section. Separate scales are no longer used for early and late radiation therapy-related events. Table 58-1 Traditional Scoring System for Radiation Lung Injury Based on the Radiation Therapy Oncology Group Data from http://www.rtog.org/ResearchAssociates/AdverseEventReporting/AcuteRadiationMorbidityScoringCriteria.aspx and http://www.rtog.org/ResearchAssociates/AdverseEventReporting/RTOGEORTCLateRadiationMorbidityScoringSchema.aspx. Table 58-2 Common Terminology Criteria Version 4* Select Common Terminology Criteria for Adverse Events Related to the Lung *This is an abbreviated/abridged version of the Common Terminology Criteria, Version 4; the complete version can be found at http://evs.nci.nih.gov/ftp1/CTCAE/About.html. †As with the older scoring systems, grade 5 (not shown) is death, and grade 0 is the absence of the particular toxicity. Note that for some adverse events, grades 1 to 2 (mild to moderate) might not be applicable (e.g., acute respiratory distress syndrome). Conversely, for some adverse events, grade 4 (life threatening) might not be applicable (e.g., cough). Tucker et al.30 found that the scoring system used (CTCv2 vs. CTCv3 vs. RTOG) greatly affected the results of analyses of the risk of RP and the radiation dose-volume factors associated with RP. Although radiation dose-volume parameters are the major predictor of radiation pneumonopathy, the addition of systemic therapy must also be considered. It appears that neoadjuvant chemotherapy before radiotherapy does not greatly affect the risk of radiation pneumonopathy. However, concurrent chemoradiotherapy probably increases the risk significantly; the maximum tolerated dose of localized radiotherapy with concurrent chemotherapy for NSCLC is generally considered to be 74 Gy,31 whereas the maximum tolerated dose for radiotherapy alone is usually considered to be higher than that.14 A combination of concurrent radiotherapy and gemcitabine appears to have a particularly high rate of radiation pneumonopathy, and extreme caution is advised for this combination (Table 58-3).32 Several other drugs, most notably the anthracyclines (e.g., doxorubicin), methotrexate, and bleomycin, should be considered contraindicated during thoracic radiotherapy.33 Concurrent thoracic radiotherapy plus a taxane (paclitaxel or docetaxel) is a commonly used and generally safe combination, although it has been suggested that the risk of radiation pneumonopathy might be slightly higher than expected from historical series based on older chemoradiotherapy regimens, particularly with weekly taxane schedules.36–36 It may be especially prudent to use three-dimensional radiotherapy techniques and to carefully analyze lung dose-volume histogram parameters in patients who are receiving a concurrent taxane. Table 58-3 Select Large Clinical Studies of the Incidence and Severity of Radiation Pneumonopathy Nontreatment factors that appear to be predictive of radiation lung injury have been studied. Not surprisingly, pretreatment performance status has been shown to correlate with development of clinical radiation pneumonopathy.37 Underlying pretreatment pulmonary function is probably an important factor as well,38 although study results have been inconsistent,39,40 perhaps because in many cases, poor pretreatment pulmonary function is due to effects of the cancer itself; an effective treatment (such as radiotherapy) may then substantially improve rather than harm pulmonary function. Other possible risk factors for toxicity include prior thoracic irradiation, volume loss due to lung collapse, forced expiratory volume in one second <2 L for severe (grade ≥3) RP,37 older age,33 female gender,21,33 never or current nonsmokers33,41,42 and poor pretreatment performance status, and pretreatment COPD in patients with lung cancer.43 Risk factors significantly associated with RP in patients with Hodgkin lymphoma were minimum lethal dose ≥13.5 Gy and V20 ≥33.5% when initial combined modality therapy consisted of Adriamycin (doxorubicin), bleomycin, vinblastine, and dacarbazine and mediastinal radiotherapy.44 Use of angiotensin-converting enzyme (ACE) inhibitors may be associated with a lower risk of RP,45 although this is controversial and not confirmed by any prospective data. Risk of radiation-induced lung injury may be higher in patients with certain genetic variations. Studies have explored ataxia-telangiectasia mutated (ATM) gene46 or TGFβ1 gene polymorphisms47 as they relate to radiation lung injury, although this parameter is not yet used clinically. With modern, three-dimensional conformal, multifield radiation therapy, SBRT, or intensity-modulated radiation therapy, it is not possible to simply look for pathognomonic rectangular infiltrates on a chest radiograph to confirm RP. A patient who has undergone radiation treatment (particularly if a large volume of lung was irradiated to a dose >20 Gy) and has symptoms should undergo computed tomography (CT) scanning, in some cases with high-resolution CT imaging. CT angiography may also be indicated to rule out a pulmonary embolism. Imaging will typically reveal an interstitial infiltrate and/or ground-glass appearance, which can be very difficult to distinguish from an infection or tumor-related changes. Suspected moderate to severe radiation pneumonopathy should be evaluated by a pulmonologist for consideration of bronchoscopy to rule out infection, particularly if fever is present.48 Pulse oximetry or arterial blood gas testing should be performed to assess the need for supplemental oxygen. Pulmonary function testing, especially the diffusion capacity of the lung for carbon monoxide (DLCO) test, is useful as part of the diagnostic workup, in particular to assess the severity of gas-exchange dysfunction, although pulmonary function tests are not strongly correlated to clinical symptoms of radiation-induced lung disease.33 Spirometric parameters of pulmonary function are frequently reversible after radiation pneumonopathy, whereas DLCO abnormalities are less likely to improve.49 The tests and procedures to be considered in the evaluation of patients with cancer who have suspected pneumonopathy are summarized in Table 58-4. This workup should be considered appropriate for either suspected radiation-related or chemotherapy-related pneumonopathy. Table 58-4 Evaluation of Patients with Cancer Who Have Pulmonary Symptoms (Especially Dyspnea) and Suspected Radiation or Chemotherapy Pneumonopathy
Pulmonary Complications of Anticancer Treatment
Pulmonary Toxicity of Thoracic Radiation Therapy
Incidence of Radiation Lung Injury and Predictive Factors
Grade
(Acute) Radiation Pneumonopathy (Within 90 Days of Start of External Beam Radiation Therapy)
(Late) Radiation Pneumonopathy (>90 Days after Start of External Beam Radiation Therapy)
1
Mild, dry cough; dyspnea on significant exertion
Asymptomatic (e.g., slight radiographic findings only) or mild symptoms (e.g., dry cough)
2
Dyspnea on minimal exertion and/or persistent cough (requiring narcotics)
Moderate symptomatic fibrosis and/or pneumonitis (severe cough), fever, patchy radiographic appearances
3
Obvious severe radiation pneumonitis with dyspnea at rest and/or severe cough unresponsive to narcotics; oxygen and/or steroids are indicated
Severe symptomatic fibrosis/pneumonitis with dense radiographic changes
3
Life-threatening respiratory insufficiency requiring continuous oxygen/mechanical ventilation
Life-threatening respiratory insufficiency requiring continuous oxygen/mechanical ventilation
5
Death
Death
Event
Grade 1†
Grade 2
Grade 3
Grade 4
Acute respiratory distress syndrome
N/A
N/A
Present with radiologic findings; intubation not required
Life-threatening respiratory or hemodynamic compromise; intubation required
Atelectasis
Asymptomatic; clinical or diagnostic observations only; intervention not indicated
Symptomatic (e.g., dyspnea, cough), medical intervention indicated (e.g., chest physiotherapy, suctioning); bronchoscopic suctioning
Oxygen indicated; hospitalization or elective operative intervention indicated (e.g., stent, laser)
Life-threatening respiratory or hemodynamic compromise; intubation or urgent intervention indicated
Carbon monoxide diffusion capacity (DLCO)
3 to 5 units below LLN; for follow-up, a decrease of 3 to 5 units (mL/min/mm Hg) below the baseline value
6 to 8 units below LLN; for follow-up, an asymptomatic decrease of >5 to 8 units (mL/min/mm Hg) below the baseline value
Asymptomatic decrease of >8 units drop; >5 units drop along with the presence of pulmonary symptoms (e.g., >grade 2 hypoxia or >grade 2 or higher dyspnea)
N/A
Cough
Mild symptoms; nonprescription intervention indicated
Moderate symptoms, medical intervention indicated; limiting instrumental ADL
Severe symptoms; limiting self-care ADL
N/A
Dyspnea
Shortness of breath with moderate exertion
Shortness of breath with minimal exertion; limiting instrumental ADL
Shortness of breath at rest; limiting self-care ADL
Life-threatening consequences; urgent intervention indicated
FEV1
99% to 70% of predicted value
60% to 69% of predicted value
50% to 59% of predicted value
≤49% of predicted value
Hypoxia
N/A
Decreased O2 saturation with exercise (e.g., <88% pulse oximetry); intermittent supplemental oxygen
Decreased O2 saturation at rest (e.g., <88% pulse oxymetry or PaO2 ≤55 mm Hg)
Life-threatening airway compromise; urgent intervention indicated (e.g., tracheotomy or intubation)
Pleural effusion (nonmalignant)
Asymptomatic; clinical or diagnostic observations only; intervention not indicated
Symptomatic, intervention indicated (e.g., diuretics or limited therapeutic thoracentesis)
Symptomatic with respiratory distress and hypoxia; surgical intervention including chest tube or pleurodesis indicated
Life-threatening respiratory or hemodynamic compromise; intubation or urgent intervention indicated
Pneumonitis/pulmonary infiltrates
Asymptomatic; clinical or diagnostic observations only; intervention not indicated
Symptomatic; medical intervention indicated; limiting instrumental ADL
Severe symptoms; limiting self-care ADL; oxygen indicated
Life-threatening respiratory compromise; urgent intervention indicated (e.g., tracheotomy or intubation)
Pneumothorax
Asymptomatic; clinical or diagnostic observations only; intervention not indicated
Symptomatic; intervention indicated (e.g., tube placement without sclerosis) or temporary chest tube
Sclerosis and/or operation indicated; hospitalization indicated
Life-threatening consequences; urgent intervention indicated
Pulmonary fibrosis
Mild hypoxemia; radiologic pulmonary fibrosis <25% of lung volume
Moderate hypoxemia; evidence of pulmonary hypertension; radiographic pulmonary fibrosis 25%-50%
Severe hypoxemia; evidence of right-sided heart failure; radiographic pulmonary fibrosis >50%-75%
Life-threatening consequences (e.g., hemodynamic/pulmonary complications); intubation with ventilator support indicated; radiographic pulmonary fibrosis >75% with severe honeycombing
Study
Patient Population
Rate of Grade 2 Pneumonopathy (%)
Rate of Grade 3+ Pneumonopathy (%)
Comments
LUNG CANCER STUDIES
Byhardt et al.156
388 patients treated with conventional (large field) chemo-RT in the RTOG experience
NS
17
2-dimensional, large-field XRT; grade 3 RP 20% with concurrent chemo-RT vs. 10% with sequential chemo-RT
Keller et al.157
488 patients with moderate dose postoperative RT
NS
3.5
High performance status population of patients, moderate dose radiotherapy
Turrisi et al.158
417 patients (limited stage small cell cancer) with concurrent chemo-RT
12
5
Small cell cancer (moderate dose RT); no difference between once daily and twice a day XRT
Wang et al.13
223 patients treated with 3D XRT + concurrent chemo
NS
32
Higher rate than other studies may reflect the use of actuarial statistics and CTCv3 definition
Hope et al.159
219 patients treated with high-dose 3D XRT
12
11
Strong association of RP with tumor location, lung DVH characteristics
Palma et al.36
836 patients in a multicenter individual patient meta-analysis
30 “symptomatic” pneumonitis
All patients received concurrent chemo—higher risk with taxane-based therapy
Movsas et al.62
205 patients in an RTOG randomized trial of chemo-RT ± Amifostine
17
10
No significant differences with/without amifostine
STUDIES IN CANCERS OTHER THAN LUNG CANCER
Lind et al.160
613 patients with breast cancer
2.4% of patients diagnosed with RP
RP was significantly more common with regional nodal irradiation
Yu et al.161
189 patients with breast cancer randomized between different chemo regimens prior to RT
5
<1
High rate (24% to 39%) of radiographic changes but low rate of clinical RP
Hughes-Davies et al.162
172 patients with bulky intrathoracic Hodgkin disease
14
NS
1% fatal toxicity
Koh et al.163
64 patients with Hodgkin disease
3
<1
RP associated with larger lung volume irradiated
Cooper et al.164
117 patients with esophageal cancer treated with chemo-RT
NS
4
Ishikura et al.165
139 patients with esophageal cancer treated with chemo-RT
2
2
In both of these studies, Radiation-induced cardiac complications and/or pleural effusions were more common than RP
Kato et al.166
76 patients with esophageal cancer treated with chemoradiotherapy
NS
4
Diagnosis and Management of (Acute and Subacute) Radiation Pneumonitis
Study*
Rationale
BASIC, MINIMAL WORKUP
CT of chest, preferably both with and without contrast
Assess extent/appearance/location of infiltrates/effusions; correlate with radiation therapy and/or surgical data; rule out recurrent/progressive cancer and/or other etiologies for dyspnea
Pulse oximetry
Assess degree of hypoxia and possible need for supplemental oxygen
Pulmonary function testing (spirometry and DLCO)
Assess extent and type of pulmonary function (radiation/drug pneumonitis is a restrictive pattern, with DLCO often markedly abnormal compared with baseline levels)
CBC/differential; chemistry panel
Rule out leukocytosis and/or leukopenia (possible signs of infection), anemia, hepatic and/or renal insufficiency (all factors that can lead to pulmonary distress)
EXTENDED WORKUP† Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access






