Highlights
- •
Omitting prophylactic PEG and younger age associated with increased weight loss.
- •
Higher risk of feeding tube duration with prophylactic PEG and older patients.
- •
Prophylactic PEG did not produce a significant change in global health score.
Abstract
Importance
The role of prophylactic percutaneous endoscopic gastrostomy (PEG) tube placement in head and neck cancer (HNC) patients treated with chemoradiation remains controversial and varies by center.
Objective
To evaluate the impact of prophylactic PEG tube placement in patients undergoing chemoradiation for HNC PEG tube use for more than 6 months and weight loss.
Design, Setting, and Participants
This single-institution retrospective study included 502 patients with head and neck cancer.
Exposures
Concurrent Chemoradiation (CCRT) and prophylactic PEG tube placement.
Main Outcomes and Measures
Univariate analyses were performed to determine risk factors for long term PEG tube and weight loss. Outcomes that were significantly associated with prophylactic PEG were selected for a multivariate analysis. The Kaplan-Meier method was used to estimate survival and the time to PEG removal, with comparisons between groups analyzed by log-rank tests. The global health status score from the EORTC QLQ30 was utilized to assess impact on quality of life.
Results
Significantly higher weight loss was seen with the following variables: 1) omitting prophylactic PEG tube (p < 0.00001), 2) younger age (p = 0.0032), and 3) adjuvant CCRT (p = 0.0005). There was significantly higher risk of feeding tube duration longer than 6 months in those who: received prophylactic PEG tube (p < 0.0001) and were older than the median age of 60.8 years (p = 0.0165) on multivariate analysis. Prophylactic PEG tube was not associated with improved global health status, overall survival, or progression-free survival on univariate analysis.
Conclusions and Relevance
Prophylactic feeding tubes significantly decreased weight loss during treatment. Prophylactic PEG tube and older than median age was significantly associated with higher risk of feeding tube duration longer than 6 months.
Introduction
Head and neck cancer (HNC) management involves a multidisciplinary approach involving surgery, chemotherapy, and radiation therapy . Concurrent chemotherapy with radiation has been shown to increase both local control and survival in locally advanced head and neck cancer .
Concurrent chemoradiation is associated with increased acute and late toxicity . Mucositis from concurrent chemoradiation can result in objective swallowing dysfunction for HNC patients . In some patients, swallowing dysfunction does not resolve with mucositis resolution and can lead to dependence on enteral feeding .
Percutaneous endoscopic gastrostomy (PEG) placement provides enteral feeding and necessary nutritional support without the need for oral intake . Multiple factors have been shown to predispose patients to PEG tube placement and extended dependency on PEG tube including concurrent chemotherapy .
Timing and indication for PEG tube varies by center. Prophylactic PEG tube placement occurs prior to the onset of mucositis and swallowing dysfunction from chemoradiation. On-demand PEG placement occurs only if necessitated by symptoms. The optimal timing of PEG tubes (prophylactic) or (on-demand) continues to be debated. Patients with prophylactic PEG placement have significantly less weight loss and fewer hospitalizations. However, data on long term PEG dependance and quality of life (QoL) over time based on prophylactic or on-demand PEG are lacking. We investigated the impact of prophylactic versus on-demand PEG tube placement on long term PEG tube dependance and overall health in patients undergoing chemoradiation of head and neck cancer at single center.
Methods
Our study was approved by the institutional review board. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline was reviewed, and our study follows the guideline. The study was conducted in accordance with the Declaration of Helsinki . A waiver of consent was obtained from the institutional review board of the institution due to the retrospective nature of the study making consent impractical and because contacting patients to obtain consent would pose a greater risk than the waiver.
Patient data was extracted from medical records and stored on a secure REDCap database and subsequently used for statistical analyses. Patients selected underwent chemoradiation, which included concurrent chemoradiotherapy (CCRT: 70 Gy in 33 fractions to involved disease and 56 Gy in 33 fractions to elective neck lymph node volumes with high-dose cisplatin every 3 weeks), surgery + CCRT, and induction chemotherapy (ICT: TPF (docetaxel, cisplatin, fluorouracil) 3 cycles) + CCRT. Radiation therapy details have been previously published . A total of 502 patients fit these criteria. Continuous variables recorded medians, inter-quartile range limits (25th and 75th percentiles), and range (maximum and minimum). Categorical variables were summarized as frequencies and percentage. Cancer sites with less than 30 patients were grouped to the “other” category. A long-term feeding tube was defined as a feeding tube duration longer than 6 months. A prophylactic percutaneous endoscopic gastrotomy (PEG) tube was defined as patients who had a PEG tube and a radiotherapy (RT) start date earlier than 1/1/2011, or patients who had their PEG tube placed before their RT start date. For risk factors, the continuous variables were dichotomized at the median into upper and lower groups. Univariate analyses, such as logistic regression or Cox regression, were performed to determine risk factors for long term PEG tube and weight loss. Outcomes that were significantly associated with prophylactic PEG were selected for a multivariate analysis.
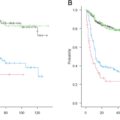
Time to PEG tube removal was defined as the duration from date of PEG placement to documented PEG out date or censored at the last follow-up date. Patients without documented PEG out date were censored at the last follow-up date. The Kaplan-Meier method was used to estimate the time to PEG tube removal, which was compared between acute and late PEG groups using log-rank tests. The proportion of patients who did not receive acute PEG, but received late PEG, was estimated using an exact binomial confidence interval.
The association between prophylactic PEG and longitudinal QoL overall health was assessed. The global health status score from the EORTC QLQ30 was utilized to assess impact on the quality of life . In the analysis we included QoL survey records from RT start to five years. We utilized linear mixed model on the survey to compare the time-averaged overall health using a mixed effect model.
Results
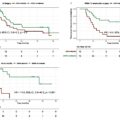
Of the 502 HNC patients examined, median overall survival was 65.8 months (95 % confidence interval (CI) of 45.9–94.3.) Progression free survival, which was measured to be the time from diagnosis to local/distant failure, or death, was 42.5 months (95 % CI of 31.9–64.6.) Prophylactic PEG tube placement did not impact overall (p = 0.237) or progression free survival (p = 0.728). Details of patient demographics can be found in Table 1 . Continuous variables were dichotomized into “higher” and “lower” groups based on the median. Baseline characteristics of patients with and without prophylactic PEG are listed in Table 2 . Median age in our cohort was 60.8 years.
| Variable | Value | Frequency | Percentage |
|---|---|---|---|
| Sex | Female | 119 | 23.7 % |
| Male | 383 | 76.3 % | |
| Race | African American | 49 | 9.8 % |
| American Indian | 5 | 1 % | |
| Asian | 4 | 0.8 % | |
| unknown | 22 | 4.4 % | |
| White | 422 | 84.1 % | |
| Smoking | Never | 100 | 19.9 % |
| Former | 274 | 54.6 % | |
| Current | 128 | 25.5 % | |
| Previous/Other Cancer | No | 400 | 79.7 % |
| Yes | 100 | 19.9 % | |
| Unknown | 2 | 0.4 % | |
| Previous Cancer Surgery | No | 430 | 85.7 % |
| Yes | 72 | 14.3 % | |
| Previous Surgery | No | 90 | 17.9 % |
| Yes | 412 | 82.1 % | |
| Previous Radiation | No | 472 | 94 % |
| Yes | 30 | 6 % | |
| Previous Chemotherapy | No | 477 | 95 % |
| Yes | 25 | 5 % | |
| Clinical stage | I | 7 | 1.4 % |
| II | 25 | 5 % | |
| III | 98 | 19.5 % | |
| IV | 360 | 71.7 % | |
| Unknown | 12 | 2.4 % | |
| Site | Larynx | 112 | 22.3 % |
| Lip/oral cavity | 82 | 16.3 % | |
| Other | 39 | 7.8 % | |
| Pharynx | 269 | 53.6 % | |
| Treatment type | CCRT | 310 | 61.8 % |
| CCRT/ND | 9 | 1.8 % | |
| ICT/CCRT | 58 | 11.6 % | |
| Surg/CCRT | 125 | 24.9 % | |
| PEG tube | No | 21 | 4.2 % |
| Yes | 481 | 95.8 % | |
| Prophylactic PEG | No | 219 | 43.6 % |
| Yes | 283 | 56.4 % | |
| Feeding tube long term | No | 87 | 17.3 % |
| Unknown | 5 | 1 % | |
| Yes | 410 | 81.7 % |
| Variable | Value | No | Yes | p-value |
|---|---|---|---|---|
| Age | higher | 116 (46.2 %) | 135 (53.8 %) | 0.2801 |
| lower | 103 (41 %) | 148 (59 %) | ||
| Sex | Female | 47 (39.5 %) | 72 (60.5 %) | 0.3411 |
| Male | 172 (44.9 %) | 211 (55.1 %) | ||
| Race | Other | 16 (27.6 %) | 42 (72.4 %) | 0.0106 |
| White | 194 (46 %) | 228 (54 %) | ||
| Smoking | Never | 53 (53 %) | 47 (47 %) | 0.0798 |
| Former | 117 (42.7 %) | 157 (57.3 %) | ||
| Current | 49 (38.3 %) | 79 (61.7 %) | ||
| Previous/ Other/Current Cancer | No | 171 (42.8 %) | 229 (57.3 %) | 0.5742 |
| Yes | 46 (46 %) | 54 (54 %) | ||
| Previous Surgery | No | 30 (33.3 %) | 60 (66.7 %) | 0.0345 |
| Yes | 189 (45.9 %) | 223 (54.1 %) | ||
| Previous Radiation | No | 206 (43.6 %) | 266 (56.4 %) | 1 |
| Yes | 13 (43.3 %) | 17 (56.7 %) | ||
| Previous Chemotherapy | No | 209 (43.8 %) | 268 (56.2 %) | 0.8369 |
| Yes | 10 (40 %) | 15 (60 %) | ||
| Clinical Stage | I | 4 (57.1 %) | 3 (42.9 %) | 0.2494 |
| II | 9 (36 %) | 16 (64 %) | ||
| III | 51 (52 %) | 47 (48 %) | ||
| IV | 153 (42.5 %) | 207 (57.5 %) | ||
| Site | Larynx | 51 (45.5 %) | 61 (54.5 %) | 0 |
| Lip/Oral Cavity | 9 (11 %) | 73 (89 %) | ||
| Other | 17 (43.6 %) | 22 (56.4 %) | ||
| Pharynx | 142 (52.8 %) | 127 (47.2 %) | ||
| Treatment Type | CCRT | 180 (58.1 %) | 130 (41.9 %) | 0 |
| CCRT/ND | 0 (0 %) | 9 (100 %) | ||
| ICT/CCRT | 20 (34.5 %) | 38 (65.5 %) | ||
| Surg/CCRT | 19 (15.2 %) | 106 (84.8 %) |
Related posts:
 Surgical complications and functional outcomes of 3191 jejunal free flaps used for reconstruction of circumferential defects following head and neck cancer resections: A systematic review
Surgical complications and functional outcomes of 3191 jejunal free flaps used for reconstruction of circumferential defects following head and neck cancer resections: A systematic review
 Submandibular gland transfer into the temporal fossa in patients with oral squamous cell carcinoma: A viable option to prevent radiation-induced xerostomia
Submandibular gland transfer into the temporal fossa in patients with oral squamous cell carcinoma: A viable option to prevent radiation-induced xerostomia
 Induction chemotherapy for locally advanced nasopharyngeal carcinoma: Efficacy and safety of the TPC regimen compared to GP and TPF
Induction chemotherapy for locally advanced nasopharyngeal carcinoma: Efficacy and safety of the TPC regimen compared to GP and TPF
 Predictors of recurrence and survival after salivary gland cancer surgery: A multicenter, retrospective study in northern Japan
Predictors of recurrence and survival after salivary gland cancer surgery: A multicenter, retrospective study in northern Japan
 The 10 %-rule debate: A fresh perspective on sentinel lymph node biopsy in OSCC
The 10 %-rule debate: A fresh perspective on sentinel lymph node biopsy in OSCC
 Deciphering molecular relapse and intra-tumor heterogeneity in non-metastatic resectable head and neck squamous cell carcinoma using circulating tumor DNA
Deciphering molecular relapse and intra-tumor heterogeneity in non-metastatic resectable head and neck squamous cell carcinoma using circulating tumor DNA
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


