Aldosterone-producing carcinomas are often over 4 cm in diameter at presentation. They are usually associated with the hypersecretion of cortisol, androgens and oestrogens, as well as high levels of aldosterone.
Clinical presentations
Patients usually present with hypertension and hypokalaemia.
Hypertension is often asymptomatic. Hypokalaemia may cause fatigue, muscle weakness, cramps, polydipsia and polyuria (due to hypokalaemia-induced nephrogenic diabetes insipidus). Serum potassium may be normal in 50% of patients. A low-sodium diet may mask hypokalaemia as reduced sodium delivery to the distal nephron diminishes aldosterone-induced potassium loss.
Early haemorrhagic strokes are characteristic in patients with glucocorticoid-suppressible hyperaldosteronism.
Investigations
Primary hyperaldosteronism should be excluded in hypertensive patients with:
- a young age of onset (< 40 years)
- severe or resistant hypertension
- hypokalaemia: spontaneous or diuretic-induced hypokalaemia that does not respond to potassium replacement.
Screening tests
Nearly all patients have a serum potassium level below 4 mmol/L. A 24-hour urine collection (72 hours after stopping diuretics) may show inappropriate potassium wasting (> 30 mmol/L in a patient with hypokalaemia). Serum sodium levels usually remain normal because of the parallel increase in the water content of the blood.
The initial screening test is measurement of plasma aldosterone concentration and plasma renin activity. A raised plasma aldosterone concentration to renin activity ratio suggests primary hyperaldosteronism. The cut-off for a ‘high’ ratio is dependent on the plasma renin activity assay and is therefore laboratory dependent.
Two things must be done before measuring the ‘aldosterone-to-renin’ ratio:
- Several antihypertensives should be stopped. Spironolactone, eplerenone, angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers and diuretics increase plasma renin activity. Beta-blockers suppress renin release, and calcium channel blockers may reduce aldosterone levels. The duration of wash-out is 6 weeks for spironolactone and 2 weeks for most other antihypertensives. If antihypertensive therapy is required, an alpha-blocker (e.g. doxazosin) may be used.
- Hypokalaemia should be corrected (with oral potassium chloride supplementation) as it reduces aldosterone secretion.
A false-negative result may be seen in chronic renal failure.
Confirmatory tests
Salt loading
The response in normal people following a sodium load is aldosterone suppression. Failure of aldosterone suppression following a sodium load confirms primary hyperaldosteronism.
Oral sodium chloride (two 1 g sodium chloride tablets taken three times a day with food) is given. On the third day, a 24-hour urine specimen is collected for measurement of aldosterone, sodium and creatinine. Urine aldosterone excretion of greater than 39 nmol per day is consistent with hyperaldosteronism. The 24-hour urine sodium excretion should exceed 200 mmol to document adequate sodium loading. Urine creatinine is measured to ensure adequate urine collection. Remember that sodium loading causes increased urinary potassium loss and hypokalaemia. Therefore serum potassium should be measured daily, and hypokalaemia must be corrected.
Alternatively, intravenous 0.9% sodium chloride (2 L over 4 hours) may be given. A plasma aldosterone level of over 277 pmol/L is consistent with primary hyperaldosteronism.
Captopril suppression test
This involves the oral administration of 25–50 mg of captopril (an ACE inhibitor), which suppresses aldosterone levels in normal people. An inability to reduce plasma aldosterone levels after administration of captopril suggests primary hyperaldosteronism.
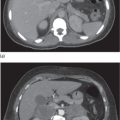
Determining the cause
The cause must be determined because of significant treatment implications. Unilateral adenomas can be surgically cured, whereas bilateral adrenal hyperplasia requires lifelong pharmacotherapy with aldosterone antagonists. The specific pitfalls of different biochemical and radiological tests need to be considered.
Postural test
Plasma aldosterone concentration, renin activity and cortisol are measured in the morning (8 a.m., after overnight recumbency) in the supine position and after 4 hours of maintaining an upright posture (at noon).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


