Prevention, Diagnosis, and Treatment of Microvascular ComplicationsPart 2/Diabetic Nephropathy and Diabetic Retinopathy
Prevention, Diagnosis, and Treatment of Microvascular Complications Part 2/Diabetic Nephropathy and Diabetic Retinopathy
I have figured out that if I drink water through a straw rather than gulp it from a large glass, I am better able to quench my thirst during these hot summer months in Southern California.
—Eddie Hunter, kidney dialysis patient since 2009
Diabetic Nephropathy
Introduction
Diabetic nephropathy is characterized by proteinuria, hypertension, and progressive kidney failure. Thirty percent of patients with T1DM and 10% to 40% of patients with T2DM will eventually develop end-stage renal failure.1 In patients with T2DM, the prevalence of diabetic nephropathy varies from 5% to 10% in Caucasian patients, 10% to 20% in African Americans, and nearly 60% in members of the Pima Indian tribe.2 In 2008, the annual cost to society to support treatment of patients with end-stage renal disease (ESRD) was $38.45 billion.3 The annual per patient cost of managing ESRD in the United States is approximately $64,000, with initial first year cost approaching $90,000.3
Primary care physicians (PCPs) should take a proactive stance in screening high-risk patients for the presence of chronic kidney disease (CKD). Once these individuals are identified, PCPs are well trained to provide interventional strategies designed to reverse or slow the progression of the disease. Confusion exists as to the most appropriate time to refer patients with diabetic nephropathy for renal consultation.4 Demands for nephrology services across the United States are severely impacted by a shortage of specialist. In 2007, 6,891 nephrologists were listed as full-time equivalent clinicians.5 Nephrology patients face a future clouded by limited specialty access. Even more worrisome is a glance into the future of the nephrology population. Although 235 nephrologists completed fellowship training in 2007, this number consistently falls approximately 200 trainees short of the projections required to manage the medical needs of renal patients in years to come. Interestingly, 30% of all currently practicing nephrologists are 55 years of age or older and may retire prior to the projected expansion of baby boomers into the ESRD market place. Currently, 13% of the U.S. population has clinical evidence of CKD.6 Clearly, the burden of CKD detection and management will be shifting toward the primary care specialties where the patient-to-physician ratios are typically 1:1,100.7
Diabetes accounts for 38% of all ESRD in the United States. The mean A1C of patients initiating treatment for ESRD is 7.6%, suggesting that risk factors such as genetics, blood pressure (BP), smoking, obesity, and hyperlipidemia may be influential in determining both disease progression and outcomes.8,9 Fortunately, diabetes-related ESRD has declined in all age groups by 3.9% per year from 1996 to 2006 as physicians become more aware of the importance of intensive metabolic management of glucose, BP, and hyperlipidemia.10
Diabetic dialysis patients and transplant recipients do have higher mortality and morbidity rates than their nondiabetic counterparts.11 Microalbuminuria may substantially increase morbidity and mortality in diabetes patients.12
Patient awareness of CKD is extremely low. Less than 10% of 2,992 adult respondents in the 1994 to 2002 National Health and Nutrition Examination Survey (NHANES) who met criteria for CKD stage 1 to 3 answered yes to the question “Have you ever been told that you have weak or failing kidneys?” Only 42% of patients with CKD stage 4 were aware of their renal impairment.13 Although PCPs are quick to obtain renal function labs on patients, few patients receive feedback on the interpretation of the results. Perhaps this adds further truth to the belief that PCP’s familiarity with CKD is suboptimal.14
The early detection of diabetic nephropathy is dependent on measuring one’s urinary albumin excretion (UAE) rate. UAE levels within microalbuminuric levels (30 to 299 mg per 24 hour or a spot urine albumin-to-creatinine ratio of 30 to 299 mg per g) identify patients at increased risk for development of overt diabetic nephropathy.15 Kidneys damaged from diabetic nephropathy will experience a gradual decline in glomerular filtration rate (GFR). Over time, as more nephrons fail, CKD will progress and patient may eventually develop end-stage renal failure. Impaired renal function, as measured by GFR, may be present even in patients with a normal UAE rate. PCPs should feel confident assessing renal function studies in all patients with diabetes while providing appropriate initial and ongoing care to these individuals.
• Normal Renal Function
GFR is accepted as the best overall index of renal function and represents the total filtration rate of the functioning nephrons in the kidney. Chronic kidney disease is defined by the National Kidney Foundation as a decline in GFR to less than 60 mL per min per 1.73 m2 for a minimum of 3 months.16 Signs of kidney damage include proteinuria, but other markers such as persistent glomerulonephritis or structural damage from polycystic kidney disease may also be present.
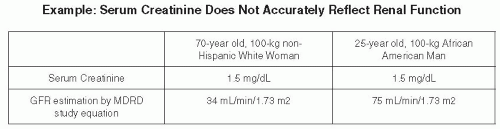
Although serum creatinine can provide a rough index of GFR, used alone, the test may overestimate renal function by as much as 40%16 (Fig. 6-1). Creatinine is produced at a fairly constant rate within muscle cells. However, the greater one’s muscle mass, the greater will be the production of creatinine. Younger patients and African Americans have more muscle mass than older non-Hispanic white individuals. Men produce more creatinine than females. Because creatinine is filtered by the proximal tubules of the kidneys, any reduction in the number of nephrons (i.e., renal insufficiency—RI) will result in an elevation of serum creatinine. RI also will result in an increase in myocyte production, secretion, and clearance of creatinine.17 Thus, validated GFR calculators must consider multiple factors including age, gender, serum creatinine, and race.18
A normal GFR ranges from 120 to 130 mL per min per 1.73 m2. Normal kidney function is proportional to kidney size, which is determined by the body’s surface area considered to be 1.73 m2 for young adults. Thus, these units are included in the GFR formula. In healthy individuals, the GFR does not decrease to less than 90 mL per min per 1.73 m2 until age 60. Early kidney disease is defined as having a GFR of 60 to 89 mL per min per 1.73 m2 with proteinuria, suggesting that the kidneys have been exposed to some form of toxicity. CKD is diagnosed when one’s GFR remains less than 60 mL per min per 1.73 m2 for greater than 3 months.19 Children reach adult values for mean GFR by approximately age 2 years.20
Figure 6-1 • Example: Serum Creatinine Does Not Accurately Reflect Renal Function. GFR is considered to be the best index of kidney function for both healthy and disease states. In this example, patients have the same weight and serum creatinine levels. They are of different races and their ages differ by 45 years. However, the calculation of their GFRs reveals substantial differences. The older woman has lost a significant number of nephrons, resulting in a diagnosis of advanced stage 3 CKD. The younger patient has evidence of CKD stage 2.
MDRD, Modification of Diet in Renal Disease.
(Reference: Shemesh O, Golbetz H, Kriss HP, et al. Limitations of creatinine as a filtration marker in glomerulopathic patients. Kidney Int. 1985;28(5):830-838.)
The Modification of Diet in Renal Disease (MDRD) equation is the preferred means by which GFR should be determined and may be accessed online.21 The Cockroft-Gault equation is used to calculate medication dosing adjustments in patients with renal insufficiency.22 Neither formula is validated for use during acute renal failure because a stable serum creatinine is required to ensure accuracy.
The MDRD has not been validated for patients with diabetic kidney disease, patients over age 70, or in those patients with normal renal function (GFR greater than 60 mL per min per 1.73 m2). The MDRD equation was developed from a study of 1,628 patients with impaired renal function, only 6% of whom had diabetes.23 Both the MDRD equation and the Cockcroft-Gault formula tend to underestimate GFR in patients with T2DM who have microalbuminuria.24 Despite the lack of precision and accuracy of the MDRD estimate, epidemiologic studies using the MDRD estimates of renal function have demonstrated a significant correlation between declining GFR trends with all-cause mortality and cardiovascular disease (CVD).25,26
The CKD-EPI equation may also be used to estimate GFR. Compared with the MDRD, CKD-EPI is more accurate at determining GFRs in patients with estimated GFR greater than 60 mL per min per 1.73 m2.27
Internet and smartphone access to all GFR calculations are found in Table 6-1.
TABLE 6-1. Internet Sites for GFR and Renal Function Calculations
From American Diabetes Association. Clinical Practice Recommendations 2011. Diabetes Care. 2011;34(Suppl 1):S33.
• Importance of Screening for Diabetic Nephropathy
The American Diabetes Association (ADA) screening recommendations for nephropathy are displayed in Table 6-2. Both estimate glomerular filtration rate (eGFR), and UAE should be accessed annually in adult patients with T2DM. Once one is diagnosed with kidney damage (defined as having abnormalities on pathologic, urine, blood, or imaging tests) or a reduced eGFR for greater than or equal to 3 months, the GFR and UAE labs should be routinely evaluated to monitor disease progression.28
eGFR is the best measure of kidney function in both healthy and ill patients. The severity of RI is determined by the eGFR level shown in Figure 6-2. eGFR is calculated based upon the serum creatinine, as well as the patient’s age, gender, and race. The GFR in patients with early stages of CKD due to diabetic nephropathy may be abnormally high due to hyperfiltration. Therefore, one must evaluate the presence of both UAE and eGFR to determine if kidney injury is present and, if so, what stage of CKD the patient is in.
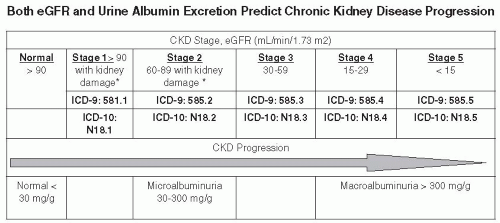
Albuminuria may be determined with a spot urine test assessing the albumin-to-creatinine ratio. A result of less than 30 mg albumin per gram of creatinine is considered normal. Microalbuminuria is defined as 30 to 300 mg per g, whereas macroalbuminuria is diagnosed when one excretes greater than 300 m per g of albumin (Table 6-3).28 Albuminuria is indicative of diabetic nephropathy, although other forms of CKD may occur in diabetic patients. One should note that the presence of albuminuria or other markers of renal damage are only necessary to diagnose CKD stages 1 and 2. Advanced CKD may be present without evidence of albuminuria.
Due to the intrasubject variability in UAE, at least two specimens, preferably first morning voids collected within a 3- to 6-month period, should be abnormal before diagnosing CKD. Stages 3 to 5 CKD occurs in the absence of UAE in many patients with T2DM. Therefore, GFR should be used to stage, rather than screen, patients for CKD.
Figure 6-2 • Both eGFR and Urine Albumin Excretion Predict Chronic Kidney Disease Progression. (ICD-9 and ICD-10 coding provided courtesy of Reinhard Beel, rbeel@hotmail.com.)
Note: A false-positive urine protein test may occur under the following circumstances: vigorous exercise within 24 hours of testing, preexisting fever or infection, presence of CHF, severe hypertension, or marked hyperglycemia.
Once these conditions are identified and corrected, the urinary protein testing should be repeated. If the A:C ≥30 in two of three specimens within 3 months, the diagnosis of albuminuria is established.
a The presence of premicroalbuminuria can increase one’s risk for developing hypertension.
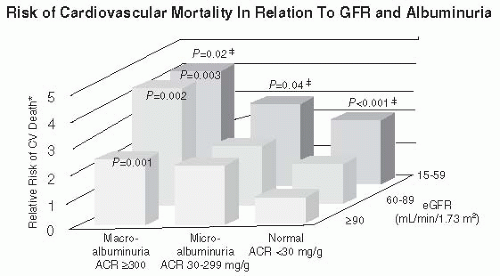
CKD increases cardiovascular (CV) risk including death. Figure 6-3 shows a graph relating GFR and albuminuria levels from 14,586 patients from the NHANES 1988 to 2000 dataset. The highest mortality rates are observed with macroalbuminuria (ACR greater than or equal to 300 mg per g) and a GFR less than 60 mL per min per 1.73 m2. Such individuals are four times more likely to die from a CV event and three times more likely to die from any cause.29 Lowest mortality rates are observed in patients with GFRs greater than or equal to 90 mL per min per 1.73 m2 and without evidence of albuminuria.
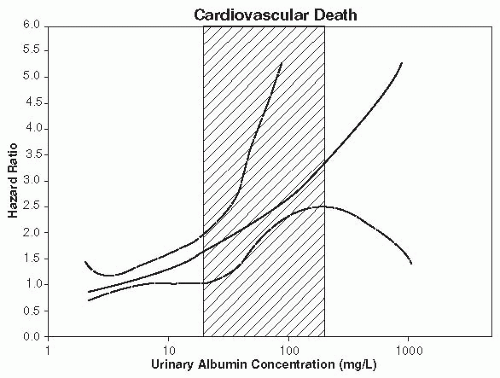
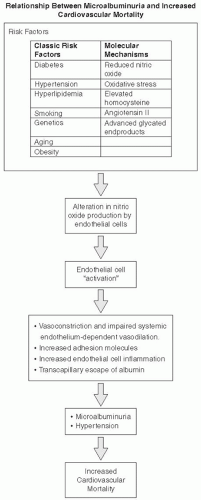
Microalbuminuria is a marker of vascular disease, endothelial dysfunction, and all-cause mortality in the general population30 (Fig. 6-4). Patients with microalbuminuria also have a greater chance of developing renal impairment over a 4-year follow-up period.31
Endothelial dysfunction may be defined as alterations in the normal properties of endothelium that are inappropriate for the preservation of organ function.32 Under physiologic circumstances, the endothelium maintains homeostasis at the vascular wall. Normal healthy endothelium reduces vascular tone, regulates vascular permeability, limits platelet adhesion and aggregation, prevents activation of the coagulation cascade, and restricts leukocyte adhesion. One of the most potent mediators of endothelium function is nitric oxide (NO). NO acts as a potent vasodilator, inhibits inflammation, growth of vascular smooth muscle, and aggregation of platelets. Altered production and bioavailability of NO are associated with endothelial dysfunction. NO production may be affected by diabetes, hypertension, aging, oxidative stress, genetic factors, and hyperlipidemia.33 As endothelial cells become inflamed and dysfunctional due to alterations in NO production, vascular permeability is increased, allowing greater rates of transcapillary leakage of albumin systemically as well as through the glomeruli.34
Figure 6-3 • Risk of Cardiovascular Mortality in Relation to GFR and Albuminuria. The risk of CV mortality rises with each 10 mL per min per 1.73 m2 decrease in estimated GFR, particularly when the GFR is less than 60 mL per min per 1.73 m2. Below this level, the risk of CV mortality increased by 29% and all-cause mortality by 22% with each 10-point reduction in GFR. The risk of CV and all-cause death also increased with each doubling of albumin/creatinine ratio by 6.3%. (Adapted from Astor BC, Hallan SI, Miller ER III, et al. Glomerular filtration rate, albuminuria, and risk of cardiovascular and all-cause mortality in the U.S. population. Am J Epidemiol. 2008;167(10):1226-1234.)
Figure 6-4 • Urinary Albumin Excretion Predicts cardiovascular Mortality in the General Population. Relationship between UAE and hazard ratio. The dotted lines represent 95% confidence limit and the squared area indicates the definition of microalbuminuria. (From Hillege HL, Fidler V, Diercks GF, et al. Urinary albumin excretion predicts cardiovascular and noncardiovascular mortality in general population. Circulation. 2002;106:1777-1782.)
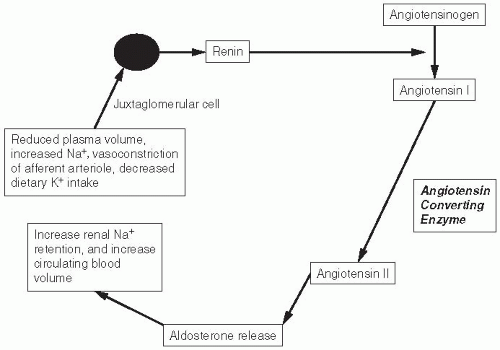
Endothelial injury increases the release of renin, an enzyme produced primarily by the juxtaglomerular cells of the kidneys. Renin catalyzes the conversion of angiotensinogen into an inactive substance: angiotensin I (A-I) (Fig. 6-5). Angiotensin-converting enzyme (ACE) then converts A-I to the physiologically active angiotensin II (A-II), which causes potent vasoconstriction, aldosterone secretion, sympathetic activation, and hypertension.35 ACE inhibitor drugs block the conversion of A-I to A-II. Angiotensin receptor blockers (ARBs) antagonize A-II-induced biologic actions, which include smooth muscle contractions, sympathetic pressor mechanisms, and aldosterone secretion.
Patients with both T1DM and T2DM who have microalbuminuria lose vasomotor control of their peripheral vessels.36,37 Elevations of UAE are associated with vascular proinflammation. Higher levels of von Willebrand factor, tissue-type plasminogen activator (t-PA), and plasminogen activator inhibitor-1 (PAI-1) are found in patients with T2DM with microalbuminuria and surrogate markers of oxidative stress.33 The resulting endothelial proinflammation and inflammation are shared metabolic consequences of hypertension and diabetes as mediated by factors such as oxidative stress. This may explain the heightened risk of CV mortality observed in all patients with microalbuminuria (Fig. 6-6).
• Chronic Kidney Disease and Cardiovascular Mortality
Patients with CKD stage 1 or 2 often have traditional Framingham CV risk factors such as diabetes, hypertension, dyslipidemia, obesity, tobacco use and advancing age. In more advanced CKD stages, the CV hazard ratio is accelerated due to the influence of nontraditional risk factors such as secondary hyperparathyroidism, anemia, oxidative stress, and vascular inflammation. Thus, proactive screening, recognition, and intensive management of renal insufficiency are required to prevent disease progression. Little can be done to reverse or delay diabetic nephropathy once the serum creatinine exceeds 2.5 mg/dL.
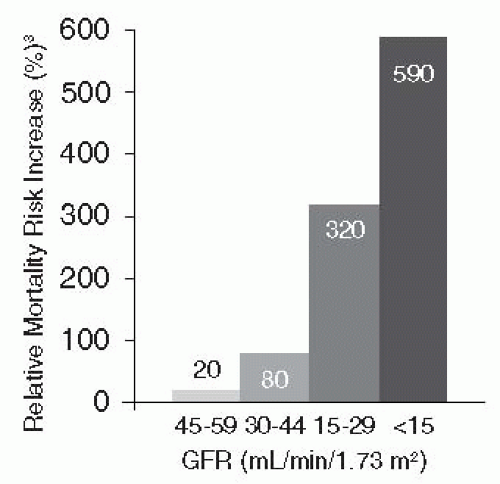
Increasing CV risk begins at the earliest stages of renal impairment and rises continuously as renal damage progresses toward ESRD (Fig. 6-7). There is a strong, continuous correlation between increased risk for CVD events and impaired renal function, which begins at the earliest stages of renal impairment and rises continuously to 20 to 30 times above the risk in the general population as renal damage progresses to ESRD.38 The relative risk of mortality for patients in ESRD is 590% higher than patients in CKD stage 3.25
Figure 6-5 • The Renin-Angiotensin-Aldosterone System: Physiology and Pharmacology. Renin is released from juxtaglomerular cells acting as pressure and renal profusion sensors. A reduction in plasma volume is perceived by the juxtaglomerular cell as a threat to maintenance of BP homeostasis. Decreased dietary potassium (K+) intake, increased plasma sodium (Na+) levels, and sympathetic input from changes in posture also result in the renin release. Renin then catalyzes the conversion of angiotensinogen into angiotensin I (A-I). ACE converts inactive A-I into active angiotensin II (A-II). A-II results in vasoconstriction, sympathetic discharge, and hypertension. ARBs block the pharmacologic effects of A-II in the periphery: smooth muscle contraction, sympathetic discharge, and aldosterone secretion. Aldosterone secretion leads to sodium retention, an increase in circulation blood volume, and a rise in BP. (Adapted from Matsubara H. Pathophysiological role of angiotensin II receptor in cardiac and renal diseases. Circ Res. 1998;83:1182-1191.)
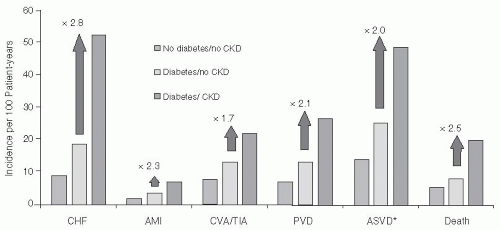
As shown in Figure 6-8, diabetic nephropathy significantly increases one’s risk for congestive heart failure (CHF), atherosclerotic vascular disease, stroke, MI, peripheral vascular disease, and mortality.
As recommended by the American Heart Association, patients with diabetic nephropathy should be considered to have the “highest risk stratification” for subsequent cardiac events, even in early stages of CKD.39 Any patient with early-stage CKD (eGFR greater than 60 mL per min per 1.73 m2) and demonstrated proteinuria should be treated as a coronary artery disease equivalent for purposes of risk stratification.40
• Predicting Risk of Chronic Kidney Disease Progression
CKD management is challenging due to the heterogeneity of the disease process, variability in rates of progression and high risk of CV mortality. Determining the probability of kidney failure may be useful for patient and provider communication, triage and management of nephrology referrals, and timing of dialysis access placement and living-related kidney transplant. eGFR is not a sufficient measure to predict progression toward ESRD.
Using a set of variables that are routinely measured in laboratories, disease progression may now be determined accurately within a primary care practice. The kidney risk equation provides the 2- and 5-year probability of progression to dialysis or transplantation for a patient with CKD stages 3 to 5.41 Physicians will need to input the patient’s age, sex, eGFR, urine albumin:creatinine ratio, calcium, phosphorus, albumin, and bicarbonate into an online formula available at: http://www.qxmd.com/calculate-online/nephrology/kidney-failure-risk-equation. A free app is also available at this web site for use on smartphones.
Figure 6-6 • Relationship between Microalbuminuria and Increased Cardiovascular Mortality.
Figure 6-7 • The Risk of All Cause Mortality Increases Sharply in Patients Having an eGFR Below 45 mL Per Minute Per 1.73 m2. In a registry study of over 1 million adult participants, patients with an eGFR less than 60 mL per min per 1.73 m2 were found to have a dramatically increased risk of death from any cause, which increased in a nonlinear fashion with decreasing GFR. Patients with stage 3 CKD were subdivided into two categories. Those with eGFR between 45 and 59 mL per min per 1.73 m2 had an increased rate of mortality of 20% compared to those patients with eGFR greater than 60 mL per min per 1.73 m2. Patients in CKD stage 4 have a 320% greater risk of all cause mortality than those with GFR levels above 60 mL/min/1.73 m2. Those patients with ESRD and a GFR < 15 mL/min/1.73 m2 have a 590% increase in mortality. (Adapted from Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004. 23;351(13):1296-305.)
• Specialty Referral Guidelines for Diabetic Nephropathy
Patients with CKD should be referred to a nephrologist for consultation and comanagement if a clinical action plan cannot be prepared, the appropriate evaluation cannot be performed, or the recommended treatment cannot be implemented. In most cases, patients with a GFR below 30 mL per min per 1.73 m2 should be referred to a nephrologist.15 Most patients will require either dialysis or renal transplantation once they progress into CKD stage 5. Unfortunately, few patients actually progress from CKD stage 4 to CKD stage 5. For patients with CKD stage 4 disease, death is twice as likely as progression to CKD stage 5.42 Five percent to 20% of all patients in CKD stage 5 die annually.43
Figure 6-8 • Among Patients with Both Chronic Kidney Disease and Diabetes, the Rate of Cardiovascular Events is More Than Twice the Rate Among Patients with Diabetes Alone. Relative to healthy individuals, patients with CKD and diabetes have a 79% increased risk of CHF, a 41% increased risk of ASVD, and a 56% increased risk of death. These statistics are from a sample of the U.S. Medicare population from 1998 and 1999 (n = 1,091,201) who were divided according to diabetes and CKD status: no diabetes, no CKD (79.7%); diabetes, no CKD (16.5%); CKD, no diabetes (2.2%); and both CKD and diabetes (1.6%). (Adapted from Foley RN, Murray AM, Li S, et al. Chronic kidney disease and the risk for cardiovascular disease, renal replacement, and death in the United States Medicare population, 1998 to 1999. J Am Soc Nephrol. 2005;16(2):489-495.)
Renal biopsy should be considered in newly diagnosed patients with T1DM with proteinuria and a rapid decline in renal function. Because nephropathy and retinopathy so often coexist, patients with CKD without evidence of eye disease should also undergo a renal biopsy to determine if the kidney disease is related to diabetes or an unrelated disorder.44 Diabetes causes unique changes in kidney structure. Classic glomerulosclerosis is characterized by increased glomerular basement membrane width, diffuse mesangial sclerosis, hyalinosis, microaneurysm, and hyaline arteriosclerosis.45 Areas of extreme mesangial expansion called Kimmelstiel-Wilson nodules or nodular mesangial expansion are observed in 40% to 50% of patients developing proteinuria.46 The indications for performing renal biopsies in patients with T2DM are unclear.
• Clinical Management of Diabetic Nephropathy
Treatment of patients with diabetic nephropathy includes the following: management of comorbid conditions, measures to slow loss of kidney function, measures to prevent and treat CVD, measures to prevent and treat complications of decreased kidney function, preparation for kidney failure and kidney replacement therapy, and replacement of kidney function by dialysis or transplantation if signs and symptoms of uremia are present.
Medications should be reviewed at all visits. Patients with stages 4 and 5 CKD should be questioned regarding the incidence of hypoglycemia. Dosage adjustments for medications such as dipeptidyl peptidase-4 (DPP-4) inhibitors (sitagliptin and saxagliptin), metformin, insulin, and sulfonylureas should be based on one’s eGFR. The primary route of elimination for sulfonylureas is via the kidneys. Elderly, debilitated, and malnourished patients with renal or hepatic impairment are most at risk for developing severe hypoglycemia in association with the use of sulfonylureas. Renal patients should be prescribed with low doses of sulfonylureas or have the drug discontinued, especially when used in combination with insulin or other glucose-lowering agents.
The ADA recommends screening for complications related to CKD when the GFR is less than 60 mL per min per 1.73 m2 (Table 6-4). Early vaccination against hepatitis B is indicated for patients likely to progress to ESRD.
The basis for prevention of diabetic nephropathy is treatment of known risk factors, including hypertension, hyperglycemia, anemia, and dyslipidemia. Lifestyle interventions should also be identified and enforced. Smoking cessation is a necessity. Patients who stop drinking alcohol may notice an improvement in their BP readings. Early recognition and management of secondary hyperparathyroidism and vitamin D deficiencies are within the realm of PCPs. Patients should be evaluated for possible coexisting obstructive sleep apnea and treated accordingly. In patients with moderate-to-severe obstructive sleep apnea, 3 months of continuous positive airway pressure (CPAP) therapy was found to lower BP, improve lipid profiles, and lower A1C by 0.2%.47 Patients with advanced CKD should be identified as potential candidates for renal transplantation and referred to an appropriate transplant center.
Progression of CKD may best be halted by intensively targeting the following behavioral, pharmacologic, and nutritional therapies:
1. Intensive glycemic control
The DCCT demonstrated that intensively managing T1DM reduces the incidence of microalbuminuria by 39%.48 “Graduates” from the intensively managed arm of the DCCT were able to reduce their incidence of microalbuminuria and hypertension by 40% even as their glycemic control deteriorated over time.49 Patients with T2DM in the United Kingdom Prospective Diabetes Study (UKPDS) who were intensively managed demonstrated a 30% reduction in the development of microalbuminuria.50 Thus, intensive treatment of glycemia targeting an A1C lower than 7% in most patients should be pursued as early as possible after the diagnosis of diabetes is made to prevent the development of microalbuminuria.
TABLE 6-4. American Diabetes Association Recommendations for Management of CKD in Diabetes
GFR (mL/min/1.73 m2)
Recommended Management
All patients with diabetes
• Yearly measurements of creatinine, UAE, potassium
a Consider evaluating risk of renal disease progression: http://www.qxmd.com/calculate-online/nephrology/kidney-failure-risk-equation.
Adapted from American Diabetes Association. Clinical Practice Recommendations 2011. Diabetes Care. 2011;34 (Suppl 1):S35.
The glycemic targets of patients with renal insufficiency should be customized. Patients with CKD stages 1 and 2 may safely target A1C levels of 6.5-7% assuming they have no other significant contraindications for diabetes intensification. Because patients with advanced stage 3 through stage 5 CKD are at higher risk for cardiovascular events and hypoglycemia, targeting an A1C in the range of 7.5% appears to be prudent.51
2. Intensive management of hypertension
Both prospective and post hoc evidence indicates that systolic blood pressure (SBP) reduction to less than 130 mm Hg in nephropathic patients is associated with a decreased progression to ESRD.52 In the Action in Diabetes and Vascular Disease Preterax and Diamicron MR Controlled Evaluation (ADVANCE) trial, a 21% reduction in the risk of new or worsening nephropathy was noted in patients as SBP was reduced to 110 mm Hg.53
Although the recommendation to lower BP to less than 130/80 mm Hg in diabetic and high-risk patients appears to have clear benefits in MOST patients, not all individuals appear to demonstrate improved outcomes with ambitious BP reduction. The ACCORD BP trial was a prospective randomized double-blind study that investigated whether therapy targeting normal SBP less than 120 mm Hg reduces CV event in high-risk patients with T2DM.54 Despite the 14.2 mm Hg difference in SBP between the intensive and standard therapy groups, the rate of nonfatal MI, nonfatal stroke, or death from CV causes was identical. Intensive hypertensive therapy was associated with a lower rate of stroke, yet serious adverse events attributed to antihypertensive treatment occurred more frequently in the intensive therapy group than in the standard therapy group. Thus, as with glycemic targets, individualization of BP targets is warranted in all patients with diabetes.
TABLE 6-5. Treatment for Diabetic Nephropathy
Treatment Category
Recommended Treatment
T1DM or T2DM with micro- or macroalbuminuria
• ACE inhibitor or ARBs
T1DM with HTN and albuminuria
• ACE inhibitor delays progression of nephropathy
T2DM with HTN and microalbuminuria
• ACE inhibitor or ARBs delay the progression to macroalbuminuria
T2DM with HTN and macroalbuminuria and RI (serum creatinine > 1.5 mg/dL)
May 25, 2016 | Posted by drzezo in ENDOCRINOLOGY | Comments Off on Prevention, Diagnosis, and Treatment of Microvascular ComplicationsPart 2/Diabetic Nephropathy and Diabetic Retinopathy