Outline
Human Papillomavirus Vaccination
Core Principles for Managing Abnormal Screening Test Results
Managing Abnormal Cervical Cancer Screening Test Results
Managing Abnormal Results in Young Women
Pap-Negative, Human Papillomavirus–Positive Women
Atypical Squamous Cells of Undetermined Significance Cytology
Atypical Squamous Cells, Cannot Exclude HSIL
Low-Grade Squamous Intraepithelial Lesion
High-Grade Squamous Intraepithelial Lesion
Managing Abnormal Results During Pregnancy
Key Points
- 1.
Human papillomavirus (HPV) persistent expression is required for progression to cancer.
- 2.
HPV vaccination has the potential to eradicate cervical cancer.
- 3.
Cervical cancer screening now relies heavily on HPV testing.
- 4.
mRNA expression is as sensitive but more specific than DNA testing.
- 5.
Screening guidelines have changed dramatically with the use of contesting and increased intervals between screenings.
Cervical cancer was once the most common cancer in women. It is among the most preventable cancers, and it has become rare among women who engage in cervical cancer prevention programs. Nevertheless, with some 100,000 preinvasive lesions diagnosed in the United States annually, it remains a substantial threat. After tremendous gains following introduction of cytology screening half a century ago, cervical cancer rates continue to fall by about 1% annually. Careful compliance with evidence-based guidelines remains critical to sustaining progress. Effective programs reflect organized public health efforts encompassing patient and clinician education, vaccination against causative types of human papillomavirus (HPV), cytology and HPV screening, colposcopy triage for abnormal screening test results, and destruction of the at-risk cervical transformation zone for women with cancer precursors.
Natural History
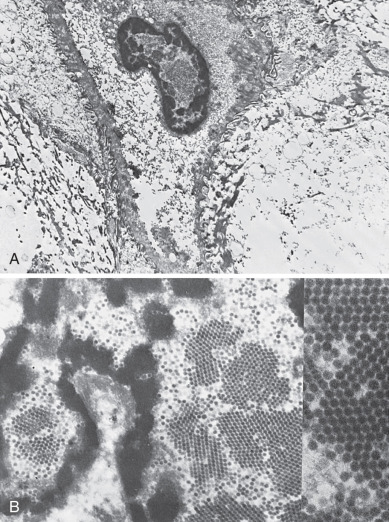
Essentially all cervical cancers arise from persistent genital HPV infections ( Fig. 1.1 ). The International Agency for Research on Cancer has designated as carcinogenic 12 HPV types: HPV-16, -18, -31, -33, -35, -39, -45, -51, -52, -56, -58, and -59. As described by Halec and associates, another eight types have been designated as possibly or probably carcinogenic: HPV–26, -53, -66, -67, -68, -70, -73, and -82. Almost 200 HPV types have been identified. A new genotype is based on DNA sequencing. A new type must share less than 90% DNA homology in the L1, E6, and E7 compared with known HPV types.
HPV-16 is the most oncogenic, accounting for more than 50% of cervical cancers. HPV-18 is found in 10% of cervical cancers and plays a particularly important role in adenocarcinogenesis. Types 31, 33, and 45 each account for around 5% of cancers. The other types are less oncogenic but have been reported in large typing studies of cervical cancers. HPV-18 and related HPV-45 are linked to cancers found at a younger age.
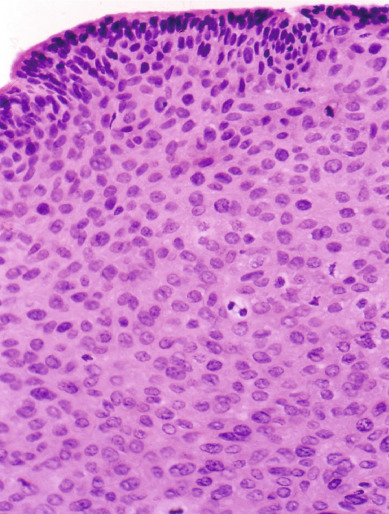
HPV infection leads to cancer through multiple pathways, but interaction of the HPV E6 and E7 gene products with p53 and pRb are critical: By inactivating or activating degradation of their targets, E6 and E7 eliminate genetic surveillance and allow unchecked cell cycling, leading to accumulation of mutations and eventual invasive cancer. HPV-16 E6 and E7 bind their targets with greater affinity than other HPV types; this may partly explain its greater oncogenicity. Persistent infections lead to cancer in steps: Initial infection into basal epithelial cells leads to establishment of a ring chromosome from which carcinogenic proteins are elaborated while virion production occurs in maturing epithelium. Disruption of the ring, often at the HPV E2 regulatory region, allows integration of E6 and E7 sequence into the host genome. The accumulation of mutations leads to nuclear changes visible cytologically as a high-grade squamous intraepithelial lesion (HSIL) and histologically as high-grade cervical intraepithelial neoplasia (CIN) ( Fig. 1.2 ) is apparent histologically. Selection for invasiveness and metastasis through additional mutation and through gene methylation results in evolution to cancer. Multitype infections do not appear to increase cancer risk, and when multitype infections include HPV-16, most lesions are caused by HPV-16. Extant HPV infections do not appear to predispose to or protect from infection by unrelated types.
Vertical transmission of HPV from mother to infant has been documented in the Finnish HPV Family Study but does not appear to result in cervical infection, with genital HPV in only 1.5% of infants after 2 years; fathers’ HPV infections did not increase infant HPV risk. Although lifetime abstinence protects against genital HPV infection, nonpenetrative sexual behaviors may transmit the virus, and male exposures modulate female risk. For example, spouses of men who engaged in sex with prostitutes were at higher risk for cervical cancer than those of men who did not, and cervical cancer risk is higher among women whose husbands had more sexual partners. Women who report recent sex only with women are also at risk, though their risk may be marginally lower than that of heterosexual women. Condom use is not fully protective against HPV infection because condoms fail to cover wide areas of genital skin, though it speeds clearance of HPV infections. Male circumcision also reduces but does not eliminate HPV and cancer risks. For these reasons, all women with prior sexual experience, including those who have not been sexually active for years, remain at risk for cervical cancer and merit screening until they have multiple negative test results.
Despite the high frequency of HPV infection, most women infected with carcinogenic HPV, including those with HPV-16, do not develop cervical cancer. Instead, most infections are cleared immunologically. HPV is an intraepithelial virus, and clearance appears to require recognition of infection by cell-mediated immune cells. Roughly half of new infections are cleared within 6 months, with half of the remainder cleared by the end of the first year after infection. Clearance is associated with greater density of CD8+ cells and lower density of T-regulatory cells in underlying stroma. Cervical treatment speeds clearance and reduces risk for posttreatment acquisition of new HPV infections. The type distribution of HPV infection after hysterectomy shows that HPV-16 and HPV-18 have a greater predilection for cervical rather than vaginal epithelium, with HPV types of lesser oncogenicity dominating in the posthysterectomy vagina.
HPV persistence is required for progression of infection to cancer, and women who clear their infections are at low risk. New infections in older women typically do not progress to preinvasive disease or cancer, and women who clear carcinogenic HPV infections have low risk for reappearance with subsequent high-grade CIN. These findings have important implications for termination of screening. Nevertheless, aging appears to result in immune senescence, with many HPV infections in older women attributable to reactivation of previously acquired by latent infections. Oral contraceptive use reduces clearance.
Although determinants of HPV persistence and progression of HPV infection to invasive cancer are poorly understood, several risk factors are known. HPV infection of a cervix undergoing active metaplasia increases risk, as reflected by the epidemiologic observations that early onset of first intercourse is associated with cancer. Smoking is linked to both CIN and cervical cancer. Benzopyrenes have been identified in cervical mucus, and the interaction of tobacco carcinogens with carcinogenic HPV increases risk substantially. Smoking also reduces immune-mediated HPV clearance. Cervical adenocarcinoma and adenocarcinoma in situ (AIS) have been linked to oral contraceptive use. Deficiencies in nutrients such as folate have been linked to cervical oncogenesis but are uncommon among US women. Variants of common HPV types that segregate by ethnicity and polymorphisms in genes related to HPV immune recognition or HPV protein products also modulate HPV persistence and carcinogenic progression. Perhaps most important, lack of screening is a high risk factor for progression of HPV infection to precancer and cancer: Whereas appropriately screened women with multiple risk factors are at relatively low risk, women with few risk factors who are not screened are at higher risk.
Immune factors play a clear role in the clearance or persistence of HPV-related cervical lesions, but the nature of immune defects is poorly understood. Fukuda and associates showed that lesions that persist have fewer Langerhans cells and helper T cells than lesions that are cleared, and tobacco smoking also lowers Langerhans and helper T-cell numbers. In contrast, Molling and associates showed that, although natural killer cells are decreased, regulatory T-cell numbers are increased in women with persistent HPV-16. Immunosuppression related to coinfection with the human immunodeficiency virus (HIV-1) illustrates the importance of immunity in the typical control of HPV. Women with HIV have much higher rates of HPV infection, including multitype infections. HPV clearance rates are lower, although most women do clear their HPV infections if observed long enough, especially if immune reserve as measured by CD4 lymphocyte count remains above 200/cmm. Although most HPV infections in HIV-seropositive women are cleared to such low levels of viral expression that they become nondetectable even with sensitive assays, reactivation appears to occur. This is apparent in cohort studies as the reappearance of previously cleared infections in women who deny sexual activity, often because of illness. Risks in other immunosuppressed states appear to be similar.
HPV infection predicts risk for subsequent high-grade CIN, even among cytologically normal women. In most cases, persistent HPV infections result first in cytologically detectable abnormalities and then in colposcopically visible lesions that grow laterally before developing into invasive cancers. The 10-year risk of high-grade CIN after a single detected HPV infection exceeds 10%.
As developed by Richart through observational studies of the cervix using cytology and colpomicroscopy, a diagnosis of CIN was based on progressively severe nuclear aneuploidy, abnormal mitotic figures, and loss of epithelial maturation. Initially considered a progressive lesion, CIN was thought to begin as a small lesion with atypia near the basement membrane of the cervical transformation zone, gradually increasing in size and becoming less differentiated with an increasing proportion of the epithelium taken up by atypical cells until a full-thickness carcinoma in situ developed and then became invasive. Given this concept of progression from low-grade to high-grade disease to cancer, lesions of all grades were treated. When progression does occur, however, it appears to require years. The median age of sexual debut in the United States is around 17 years of age, and HPV acquisition commonly follows, but the peak age of cervical cancer diagnosis lags by some 3 decades. This long transition time allows for even moderately sensitive screening tests to identify persistent lesions for treatment before invasive cancer develops ( Table 1.1 ).
| Stages | Mean Years |
|---|---|
| Normal to mild to moderate dysplasia | 1.62 |
| Normal to moderate to severe dysplasia | 2.2 |
| Normal to carcinoma in situ | 4.51 |
Gradually, the regressive nature of most low- and midgrade lesions became apparent. Low-grade lesions, including warts and CIN1, are histologic expressions of HPV infection. Greenberg and associates found that of 163 women with CIN1 after low-grade cytology followed for a median of 36 months, 49% regressed, 43% persisted, and only 8% progressed to CIN3. In the Atypical Squamous Cells of Undetermined Significance/Low Grade Squamous Intraepithelial Lesion Triage Study (ALTS), a large randomized trial of management options for women with borderline cytology results conducted under the auspices of the US National Cancer Institute (NCI), 2-year risk for CIN3 were 10% among women with CIN1. As reported by Castle and coworkers, after controlling for HPV genotype, with HPV-16–associated CIN1 progressing to CIN3 in 19% of cases, biopsy-proven CIN1 was not a risk factor for progression. These risk estimates may be substantially higher for women with prior high-grade cytology.
Higher grades of dysplasia appear to represent clonal lesions arising from single-type HPV infections. Although women may harbor multiple HPV types in the genital tract, most multitype infections are associated with multifocal lesions. Moscicki and her team showed that 63% of adolescents and young women with CIN2 resolved lesions without treatment within 2 years; subsequent clearance was minimal, rising only to 68% after an additional year. McAllum and colleagues showed a similar 62% regression after only 8 months of observation for women with CIN2 younger than 25 years of age. No patients in either study progressed to cancer during observation. In both studies, identified CIN2 likely represented recent HPV infections. Regression rates are lower in older women, at least in part because lesions detected later may have been persistent for years, and lesions that have evolved mechanisms to evade host immune-mediated clearance are likely to continue to persist. Castle and coworkers compared CIN2 rates in the immediate colposcopy and cytology surveillance arms of the ALTS. They found that over 2 years, some 40% of CIN2 regressed. Trimble and colleagues showed that HPV-16–associated lesions are less likely to resolve. Their finding of associations with human leukocyte antigen (HLA) alleles and regression support a role for HLA-restricted HPV-specific immune responses in determining clearance.
Untreated, CIN3 poses considerable risk of progression to invasive cancer. This was best shown in a study of New Zealand women with CIN3 who were diagnosed between 1955 and 1976 and were observed. Among 143 women reported by McCredie and coworkers, managed only by punch or wedge biopsy, 31 progressed to cancer of the cervix or vagina after 30 years. Risk rose to 59% in 92 women with persistent disease after 2 years of observation. These findings show both that treatment of CIN3 is mandatory regardless of age or other factors but also that not all CIN3 lesions will inevitably progress to cancer.
Treated CIN3 continues to pose a risk of progression to cancer. Women in the New Zealand study whose treatment appeared adequate by current standards faced only 0.7% cancer risk after 30 years. Studies from Scandinavian countries with integrated health systems can link databases on procedures and subsequent cancers and provide accurate long-term results with minimal loss to follow-up. Strander and associates showed that risk for cervical cancer rose significantly in previously treated women after age 50 years, with standardized incidence ratios compared with untreated women ranging from 3 to 5. Vaginal cancer risks were elevated across all ages, although the absolute risk of vaginal cancer was low. Kalliala and colleagues in Finland confirmed this long-term increased risk and also found an increased risk for nongenital smoking-related cancers. Jakobsson and coworkers found that in addition to cervical cancer, women treated for CIN faced higher mortality rates from circulatory system, alcohol-related, and traumatic death, consistent with the demographic and behavioral factors linked to CIN.
Epidemiology
More than 80% of sexually active individuals acquire genital HPV infections. Some 20 million Americans and 630 million persons worldwide are infected with HPV. In the United States, about 6.2 million people will acquire a new infection annually. Prevalence rates are highest among women in their late teens and early 20s, declining with age. Risk factors for HPV acquisition include smoking, oral contraceptive use, and new male partners.
Among high-risk HPV types, HPV-53 is most common, detected in 5.8% of US women ages 14 to 59 years screened in the National Health and Nutrition Examination Survey (NHANES) in 2003 to 2006. This was followed by HPV-16 (4.7%), HPV-51 (4.1%), HPV-52 (3.6%), and HPV-66 (3.4%). HP-V18 was present in only 1.8% of screened women. In NHANES, demographic risk factors for prevalent HPV infection included younger age, peaking at ages 20 to 24 years; non-Hispanic black ethnicity; unmarried; never educated beyond high school; and living below the poverty line. Behavioral risk factors included reporting ever having sex, first intercourse before age 16 years, greater numbers of lifetime partners, and number of partners in the past year. HPV type distributions vary across continents.
HPV infection determines subsequent risk for precancer. Among women enrolled in a Portland health maintenance organization who had HPV-16, the 10-year risk for CIN3, AIS, or cancer was more than 15% after HPV-16 infection, almost 15% after HPV-18, less than 3% after other oncogenic HPV infections, and less than 1% after a negative HPV test result.
In the United States more than 400,000 cases of CIN are identified annually, at a cost of approximately $570 million. Of these, Flagg and colleagues estimate about 100,000 are true precancers. The annual incidence of high-grade CIN is some 6 to 10 times higher than cervical cancer incidence. Preinvasive lesions begin to appear some 2 years after infection. Cancer risk is quite low soon after infection: Despite a high prevalence of HPV detection among sexually active teens, cervical cancer incidence is only about 1 in 1,000,000 before 20 years of age. Among women who develop high-grade CIN, only 30% to 50% will develop cancer over years of observation.
Although demographic and behavioral risk factors cannot be used to target evaluation or therapy, clear risks for CIN and cervical cancer have been identified. The international Collaboration of Epidemiological Studies of Cervical Cancer reviewed evidence for various risk factors for cervical cancer and carcinoma in situ, although their studies were not linked to HPV data. They found that oral contraceptive use raised the risk for cervical disease by 1.9-fold for every 5 years of use. First intercourse before 15 years of age was associated with twice the risk of cervical cancer found in women with first intercourse after 23 years of age, and having more than five lifetime sexual partners carried more than double the cervical cancer risk of lifetime monogamy. Lesser but still significant increases in risk were associated with number of pregnancies and earlier age at first term pregnancy. Both squamous cancers and adenocarcinomas share epidemiologic risk factors, except that smoking is linked only to the former.
The role of family history in determining cervical cancer risk. Dissociating genetic components of familial risk from cultural ones is difficult, as sexual attitudes and behaviors, reproductive patterns, and smoking are often linked to family. Zelmanowicz and associates assessed the role of family history in cohorts of women prospectively studied in Costa Rica and the United States. A family history of cervical cancer in a first-degree relative tripled the risk for CIN3 or squamous cervical cancer. The effect persisted after controlling for HPV exposure. No effect of family history on adenocarcinoma risk was seen. Although several genome-wide association studies (GWASs) have identified a range of genetic variants in candidate pathways that might contribute to cervical oncogenesis, Chen and colleagues in a large Chinese GWAS found that only HLA and major histocompatibility class I polypeptide-related sequence A genes were identified as candidate risk genes across several populations.
Lower socioeconomic status (SES) and minority ethnicity are also linked to CIN and cervical cancer risk in the United States, although distinguishing cultural contributions to cervical cancer risk, such as a sense of fatalism, distrust of the medical care system providing screening services, and lack of health education about the benefits of screening, are difficult to distinguish from biologic risks related to ethnicity and SES, such as genetic predisposition, toxin exposure, and micronutrient deficiencies.
Human Papillomavirus Vaccination
Because HPV is the cause of essentially all cervical cancer, HPV vaccination has the potential to eliminate cervical cancer. However, the US experience with HPV vaccination has shown that several barriers will limit achievement of this goal.
Intramuscular delivery of synthetic HPV L1 capsid antigens results in humor immunity; current vaccines are created in protein synthesis using cell culture systems; because no actual live or killed virions are used, HPV vaccines cannot cause HPV-related cancer. Despite early concerns that humoral immunity would be insufficient to prevent infection, vaccine efficacy appears to approach 100%. However, currently available vaccines are prophylactic: They must be delivered before HPV exposure and do not appear to reduce risk in untreated women with established target-type HPV infections. This is reflected in the epidemiology of vaccine effectiveness, which declines with age, number of prior sexual partners, and prior abnormal cytology. These findings mean that, although vaccination is effective for type-specific HPV naïve women through 45 years of age, population effectiveness is too low to justify widespread use of vaccines beyond the upper age limit in vaccine trials, which extended to 26 years of age. Within trials, effectiveness declined with age, and the American Cancer Society has reiterated its guidance that HPV vaccination extend only through 18 years of age.
Three HPV vaccines are available. US clinicians have favored the quadrivalent HPV vaccine, which protects against HPV-16 and -18, which together account for almost 70% of all cervical cancers, as well as HPV-6 and -11, which are the most common causes of genital warts. The benefit of cervical cancer prevention, which might take decades to become manifest, is augmented by its ability to prevent genital warts, a concern for many young women. The bivalent HPV vaccine protects against only HPV-16 and -18 and is less commonly used in the United States. It may have superior antigenicity and may have some cross-protection against HPV types related to HPV-16 and -18. Most recently, a nonavalent vaccine has been introduced, which is effective against the same types as the quadrivalent vaccine and also includes coverage against HPV types 31, 33, 45, 52, and 58; enhanced coverage should prevent 90% of all cervical cancers.
Because HPV vaccines are prophylactic, population-based vaccination should begin before first sexual intercourse. Because some 5% of US 13-year-old girls are sexually active, the target age for HPV vaccination is the ages of 11 to 12 years. However, vaccination can be initiated at 9 years of age in populations in which sexual debut may occur earlier. Three injections over 6 months are recommended for all vaccines, although schedules vary. Some data suggest that two injections or even one may be sufficient, at least for adolescents, but shortened vaccination schedules have not been approved by the US Food and Drug Administration (FDA). Because teen sexual activity is unpredictable, delaying vaccination until girls are more mature risks missing the vaccination window for many. Nevertheless, many sexually active young women show no evidence of infection by target HPV types, and “catch-up” vaccination should be considered. Testing of cervicovaginal secretions and serum antibody testing are both insensitive for detecting prior HPV vaccination and are not recommended before a decision about HPV vaccination.
Several countries have instituted organized vaccination programs, either mandatory or using a school-based opt-in mechanism with high uptake. Countries that used quadrivalent vaccine have documented a dramatic decrease in genital warts among teens but not older women, and abnormal cytology rates have also fallen in the youngest women.
In the United States, vaccination rates are suboptimal, with barely one-third of girls in target populations having received all three injections. Regrettably, despite the potential for vaccination to eliminate the disparately high risk of cervical cancer among women of minority ethnicity and lower SES, uptake has been lowest in these groups, potentially widening cancer disparities in future years. Nevertheless, decreases in HPV-16 and -18 in the pool of sexually active young women have been documented, suggesting that less than ideal vaccination rates may nevertheless eventually yield population effectiveness.
Vaccine risks appear tolerable. Common side effects include fever, rash, injection site pain, nausea, headache, and dizziness. Anaphylactic and vagal reactions may be fatal, so vaccination should only be administered in sites with ability to manage anaphylaxis and fainting. Despite initial concerns, HPV vaccination status does not enter into young women’s decisions to initiate sex. Vaccination is contraindicated for pregnant women, although no congenital anomalies or adverse pregnancy outcomes have been linked to HPV vaccination; the vaccine series may begin after delivery. Interruption of vaccination does not appear to require reinitiation of the three-shot series.
The duration of vaccine effectiveness is unclear, but antibody levels remain elevated for several years after vaccination. Booster doses are not recommended at this time. However, revaccination with nonavalent vaccine may provide additional benefit and should be considered for women younger than 26 years of age who previously completed bivalent or quadrivalent vaccines, especially those who have not initiated sexual activity and so are at low risk for having acquired HPV.
A history of HPV vaccination does not alter screening recommendations for US women. This is because many women of screening age were not vaccinated before initiating intercourse, so vaccine effectiveness is unclear. There is no central US vaccine registry, and identifying vaccinated women by self-report may be inaccurate. No HPV vaccine covers all carcinogenic HPV types, so women vaccinated before first intercourse remain at risk for infection and cancer due to nonvaccine types. However, for women known to have been vaccinated against HPV-16 and -18 before first intercourse, and so at much lower risk for disease, deferring screening initiation until age 25 years and screening with HPV testing alone at 5-year intervals is rational.
Screening
The goal of any cancer prevention program is the reduction of morbidity and mortality through intervention before symptom onset. The current mechanism to achieve this goal is the identification and destruction of high-grade CIN lesions that are presumed precancers. Many novices and some experienced clinicians mistake the mechanism for the goal. However, identification of apparent precancers in women with comorbidities that will be fatal in the medium term, before progression to symptomatic cancer, is not helpful. High-grade CIN in young women may resolve spontaneously and in some cases may be observed to avoid the sequelae of treatment. On the other hand, some women without identified high-grade CIN face cancer risks similar to those of women with high-grade CIN and merit destructive cervical therapy.
Classically, screening has relied on Papanicolaou cytology testing followed by colposcopic assessment of women with Pap abnormalities, directed biopsy of the worst colposcopic lesion, and treatment of biopsy proven high-grade lesions. Papanicolaou testing is relatively insensitive: A single Pap test may be negative in almost half of women with high-grade CIN. However, progression from HPV infection to cancer usually requires several years, allowing for multiple rounds of screening, with greater sensitivity than single tests.
Cytology is the interpretation of all the mutations, methylations, and other genetic modifications that alter the nuclear and cytoplasmic appearance of cells. As such, it is infinitely graded. To be clinically useful, these changes must be aggregated into categories that reflect a common natural history. Papanicolaou developed a five-class grading system, from normal to invasive cancer, with atypia, dysplasia, and carcinoma in situ between. Modified systems were developed, and alternatives were proposed. To unify terminology, the NCI convened a consensus meeting that developed the 1988 terminology known as the Bethesda System for cervicovaginal cytologic diagnosis. With the most recent update in 2001, this classification system identifies cytology as satisfactory or unsatisfactory, includes nonneoplastic changes, and divides epithelial cell abnormalities into squamous and glandular changes of varying degrees of severity ( Table 1.2 ). Distinguishing squamous from glandular abnormalities is critical because glandular abnormalities carry much higher risk for high-grade CIN, including squamous dysplasias, as well as endometrial cancer and cervical adenocarcinoma and AIS. Squamous changes related to HPV are termed “squamous intraepithelial lesions (SILs)” because some lesser changes do not reflect dysplasia or neoplasia, only cytomorphologic changes of HPV infection. Indeterminate lesions are termed “atypical squamous cells (ASC),” and these are subdivided into ASC “of undetermined significance (ASC-US),” which carries a low risk of associated high-grade CIN, or “cannot exclude high-grade SIL (ASC-H),” which is a more ominous finding that requires immediate colposcopy (see later discussion). An online atlas allows pathologists to standardize findings and interpretations against national norms ( http://nih.techriver.net ). The 2001 update provided the basis for subsequent consensus conferences that provided risk-based management guidelines.
|
Traditional Pap smears were collected by smearing samples across a glass slide and applying fixative followed by staining with a Papanicolaou stain. Today most cytology tests in the United States are conducted using liquid-based assays. In these tests, cells are collected and suspended in preservative solution and then transferred to a slide. Liquid-based cytology results in an even dispersion of cells, and techniques are available that allow for elimination of red and white blood cells, but the “tumor diathesis” of pus and necrosis that allowed identification of cancer is lost, as are the “microbiopsies” that allowed interpretation of epithelial fragments. Liquid-based cytology was marketed as more sensitive than conventional Pap smears. However, a meta-analysis by Arbyn and colleagues showed that, although liquid-based cytology yields more abnormalities, including high-grade SILs, it is not superior to conventional smears in cancer prevention. It remains preferred in the United States because it allows for molecular triage of equivocal results using HPV and other assays. Interpretation is still done visually, although some centers use automated imaging and pattern recognition software to eliminate the least abnormal slides. Cytotechnologists perform initial assessment, with slides containing abnormal findings and a proportion of normal slides read by cytopathologists.
The effectiveness of screening has not been demonstrated in randomized trials, but population studies have shown unequivocal benefits. . An NCI study by Erickson and associates assessed cytology screening by vaginal aspiration for 108,000 women in Shelby County, Tennessee. They showed a high yield of unsuspected high-grade CIN and early cancer at the first screen, with a substantial reduction in invasive lesions in the second screen. Gustafsson and associates reviewed data from 17 cancer registries and showed marked effects, especially in Scandinavian countries. Eddy assessed the impact of screening on cervical cancer incidence and death. Without screening, a 20-year-old average-risk woman faces a 2.5% risk of cancer and a 1.2% risk of cancer death. Triennial screening between ages 20 and 75 years reduces risk to less than 0.4% and 0.1%. Annual screening improves effectiveness but by less than 5% of these low rates, with substantial increase in cost.
Initially, screening was opportunistic: Women had screening when they presented for care, usually at annual visits. Opportunistic screening remains the norm in the United States, although screening intervals have lengthened; some electronic medical records prompt clinicians when screening is due; and some health care organizations have developed standards, rewards, and reminders. Several countries with centralized medical care systems have developed organized screening, with coordinated identification, invitation, and management of women due for screening. Serraino and colleagues showed that the move from opportunistic to organized screening in Italy resulted in a decline in cervical cancer incidence and a downstaging of incident cervical cancers after an increase in precursor detection. Quinn and coworkers found that institution a national call/recall system with incentive payments to general practitioners in Britain instituted in 1988 increased screening coverage to 85% of the target population, increased detection of high-grade CIN, and reduced mortality in women younger than age 55 years.
Cytology-based screening has several weaknesses. Most fundamentally, the process of screening, triage, and treatment is cumbersome, and noncompliance at any point renders it ineffective. Cytology results are reported in ways that can be confusing, and efficient, effective management may require integration of current results with prior abnormalities. Multiple studies have shown that most women who develop cervical cancer in developed countries, especially those presenting at advanced stages, are inadequately screened. Sung and associates studied incident cancers in a US prepaid health plan. They reported that 53% were nonadherent to screening, 28% had false-negative Pap tests, 4% had inadequate follow-up after an abnormal Pap test result, and the rest either developed cancer despite appropriate investigations or were unclassified. Kinney and associates in the same US health maintenance organization found that 60% of cervical cancer patients were inadequately screened. Deeper exploration of the records of long-standing plan members with inadequate screening showed that 70% had missed opportunities for screening in primary care clinics.
In addition, cytology-based screening performs poorly in younger women. Sasieni and colleagues from Britain showed that cervical screening in women ages 20 to 24 years had little impact on actual cancer risk until those women reached 30 years of age, but screening older women results in an immediate benefit. Because younger women have low rates of cervical cancer incidence and death but high rates of HPV infection, abnormal cytology, and CIN destined to regress, the benefits of early initiation of screening may be difficult to balance against potential harms. Cytology preferentially detects squamous cell carcinomas, and the impact of cytology screening on adenocarcinoma incidence has been muted.
The harms of excessive screening are more difficult to quantify. These include stigmatization, unfounded fear of cancer, and interventions without cancer prevention benefit. Sharp and associates showed that depression, distress, and anxiety occurred in 15% to 30% of women in the months after reporting of marginal cytology abnormalities. The costs, pain, and inconvenience of testing, triage, and treatment of abnormalities destined to regress with no impact on cancer morbidity or mortality must outweigh nonexistent benefits, though prospectively identifying these lesions in individuals is problematic.
Essentially all cervical cancer is caused by HPV. Castle and colleagues have shown that women who test HPV negative remain at low risk for precancer and cancer for more than a decade. Incorporation of HPV testing into screening has allowed for longer screening intervals. The development of HPV assays has allowed the development of protocols for HPV testing as a primary screening test in combination screening with cytology (co-testing) and as a triage test for women with borderline cytology results. Only high-risk HPV types have a role in screening; because low-risk types essentially play no role in screening and identification of HPV infection in the absence of visible genital warts causes stigmatization without impacting care, testing for low-risk types is contraindicated. HPV genotyping assays for types 16 and 18 identifies women at higher risk. The disadvantage of HPV testing is poor specificity, with up to 30% of young women testing positive in some studies. Because all commercially available HPV tests have a detection threshold designed to balance sensitivity and specificity, a negative test result does not absolutely exclude HPV infection, and prior cytologic or histologic abnormalities may mandate close follow-up or even treatment despite absence of detectable HPV. The performance characteristics of HPV assays that have not been FDA approved are unknown, and these tests should not be used in the absence of peer-reviewed literature describing their sensitivity and specificity against histologically defined precancer in large screening populations. HPV tests also should not be collected in media whose effects of test performance have not been evaluated by the FDA.
Although only one HPV assay was approved in the United States for primary screening at the time of writing, four assays were approved for risk stratification for women with ASC-US cytology and for screening in conjunction with Pap testing. Comparative trials are few. Cuzick et al. studied six HPV assays, some of which are available only in Europe. They found that an mRNA test had similar sensitivity but greater specificity than DNA tests.
Beyond these weaknesses, screening has potential harms. Identification of HPV infection, abnormal cytology, and cervical cancer precursors is not without consequences, including anxiety, relationship disruption after diagnosis of a sexually transmitted infection, the inconvenience and cost of accelerated follow-up visits, and the pain of repeated examinations. Treatment of precursor lesions also carries risks, including bleeding, infection, and injury to adjacent organs. Some studies have suggested that destructive cervical treatments increase the risk for preterm delivery and pregnancy loss. US studies have failed to replicate these results in women after cervical loop electrosurgical excision procedure (LEEP). Women with cervical dysplasias are at higher risk for pregnancy loss that those who do not, perhaps because of common risk factors, including smoking, nutritional deficiencies, and lower SES, and these confounding factors may account for differences. However, there may be a threshold effect for treatment, and women with deep or repeated excisional procedures may be at higher risk for pregnancy loss. Shorter screening intervals with increasingly sensitive tests will reduce cancer risk, but benefits decline toward an irreducible asymptote, but harms and costs climb.
After the utility of screening is accepted, societies, women at risk, and clinicians must decide when to initiate screening, which screening tests to use, how often to screen, and when toward the end of life the identification of asymptomatic disease ceases to be beneficial. With all choices, sensitivity and specificity must be balanced. Earlier screening starts with more sensitive tests at shorter intervals until later in life will decrease cancer incidence and mortality, but costs and harms from diagnosing lesions that would never have progressed to cancer will increase. In developed societies, guidelines for screening have been developed by experts assessing evidence for benefit and harm and deciding how these can best be balanced. In the United States, the most cited guidelines were released in 2012 guidelines by the US Preventive Services Task Force (USPSTF) and a consensus conference sponsored the American Cancer Society (ACS), the American Society for Colposcopy and Cervical Pathology (ASCCP), and the American Society for Clinical Pathology (ASCP) ( Table 1.3 ). The two guidelines were developed from a common evidence assessment and reached similar conclusions. In both sets, screening is recommended to begin at 21 years of age, continuing at 3-year intervals until 65 years of age, when screening should stop if the patient is adequately screened and has no history or prior high-grade CIN. Screening also should stop at the time of total hysterectomy for indications other than high-grade CIN or cervical cancer. The ACS/ASCCP/ASCP guidelines contain a preference for screening using combination cytology and HPV testing beginning at 30 years of age; the USPSTF considered co-testing between 30 and 65 years of age to be acceptable but did not find evidence sufficiently compelling to prefer it. Table 1.3 compares the two guidelines.
| USPSTF | ACS/ASCCP/ASCP | |
|---|---|---|
| When to start? | Age 21 years | Age 21 years |
| How often? | Pap tests every 3 years Co-tests every 5 years at ages 30–64 | Pap tests every 3 years at ages 21–29 years Co-tests every 5 years at ages 30–64 years preferred Pap tests every 3 years remain an option |
| When to stop? | Age 65 years if adequate prior screens | Age 65 years if the patient has had three negative Pap tests or two negative co-tests After hysterectomy for benign disease |
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


