Figure 13.1
Organization of the operating room equipment and personnel for posterior retroperitoneoscopic adrenalectomy
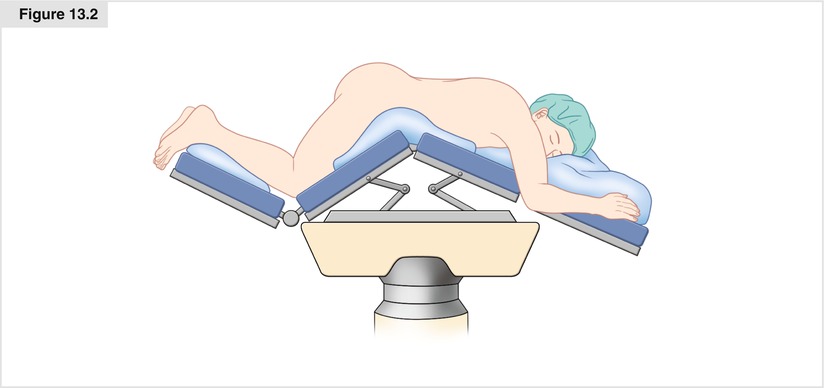
Figure 13.2
Positioning of the patient
Figure 13.3
The initial incision for 12 mm port (middle), with additional 5 mm port sites (medial and lateral)
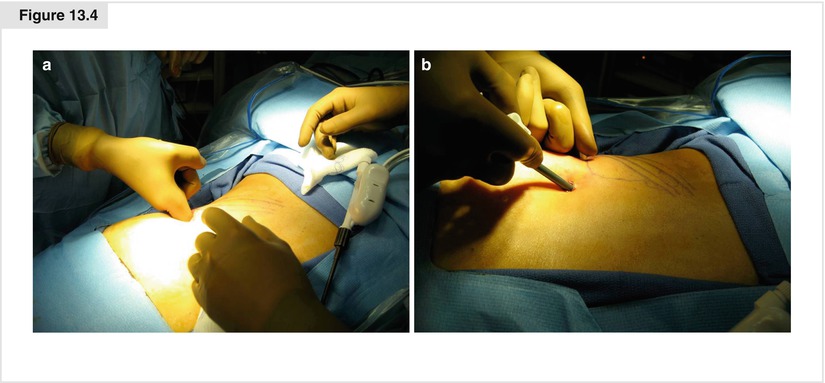
Figure 13.4
(a) The 12 mm trocar site incision is made in the left flank, and blunt dissection performed with a finger to enter the retroperitoneal space. (b) The medial 5 mm trocar is placed into the retroperitoneal working space with digital guidance
13.2.2 Creation of Working Space and Identification of Critical Landmarks
Insufflation pressures of 18–24 mmHg are utilized in the retroperitoneum to create an adequate working space. Opening of this potential space requires only the institution of positive gas insufflation and some gentle spreading with blunt-tipped instruments. A gentle, opposing, spreading motion of two instruments is used to open Gerota’s fascia (Fig. 13.5), exposing the perirenal and periadrenal fat. The upper pole of the kidney should be identified as a critical starting landmark for the dissection. The adrenal gland is found superomedial to the upper renal pole, and is generally situated very medially against the paraspinous muscles. The inferior portion of the gland occasionally extends in part somewhat anterior to the kidney (behind the kidney as viewed from the posterior approach). The surgical anatomy of the adrenal glands from the posterior view is shown in Fig. 13.6. The amount of retroperitoneal fat depends on the patient’s body habitus, and initial identification of the superior pole of the kidney is the key to establishing the surgical anatomy required to continue the dissection.
Figure 13.5
The opening of Gerota’s fascia, exposing the perirenal and periadrenal fat
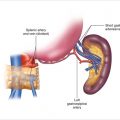
Figure 13.6
The surgical anatomy of the adrenal glands from the posterior view
13.2.3 Adrenal Gland Dissection: Operative Strategy
The initial localization of the adrenal gland within the retroperitoneal fat may be elusive at first, but with experience, the bright yellow appearance of the adrenal cortex is readily identified. Ultrasound may facilitate the expedient localization of the gland and may be performed in the operating room after patient positioning and prior to the incision, or with a laparoendoscopic ultrasound transducer. A suggested strategy for adrenal gland dissection is to initially develop the plane between the upper border of the kidney and the inferior edge of the adrenal gland. After defining the adrenal gland border, this dissection is continued around the inferior and medial aspects of the gland until the adrenal vein is identified. The upper pole of the kidney is gently retracted laterally and inferiorly, and the inferior and medial border of the adrenal gland is dissected (Fig. 13.7). The superolateral (diaphragmatic) and anterior (peritoneal) attachments of the adrenal gland are left intact until later, leaving the gland anchored for optimal dissection.