Popliteal Resections
Amir Sternheim
Yair Gortzak
Jacob Bickels
BACKGROUND
Soft tissue sarcomas of the popliteal fossa are rare, accounting for less than 5% of all soft tissue sarcomas of the extremities. Surgery in this anatomic area is challenging: Performing a wide resection with negative surgical margins is often difficult because of the periarticular location and the proximity to neurovascular structures.3,7,10
Such tumors formerly were treated with amputations4; however, better understanding of tumor biology and advances in chemotherapy and radiation therapy now allow limb-sparing procedures to be performed in most of these cases.
ANATOMY
The popliteal space is diamond-shaped; on its superior aspect, it is bounded by the semimembranosus and semitendinosus muscles medially and by the biceps femoris muscle laterally. Its inferior boundaries are the two heads of the gastrocnemius muscle. The roof of the fossa is the thin popliteal fascia; the floor is the posterior aspect of the distal end of the femur, the posterior capsule of the joint, and the popliteus muscle, which overlies the proximal tibia.
The popliteal artery and vein enter the popliteal space from its medial aspect through the adductor hiatus and lie directly behind the posterior capsule of the knee joint.
They run obliquely through the fossa and branch into two superior, a single middle, and two inferior genicular branches. After exiting the popliteal fossa, the popliteal artery divides into its terminal branches: the anterior tibial, posterior tibial, and peroneal arteries. The popliteal vein lies between the tibial nerve and the popliteal artery. The short saphenous vein pierces the popliteal fascia to join the popliteal vein within the fossa.
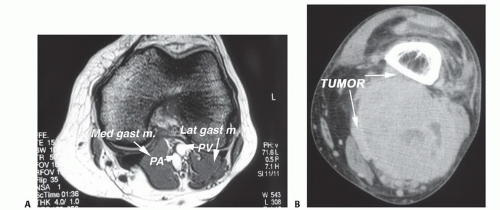
FIG 1 • MRI of a typical popliteal sarcoma. A. Normal MRI of the distal section of the popliteal (diamond) space through the medial and lateral gastrocnemius muscle insertions onto the femoral condyles. B. Large popliteal soft tissue sarcoma. (continued)
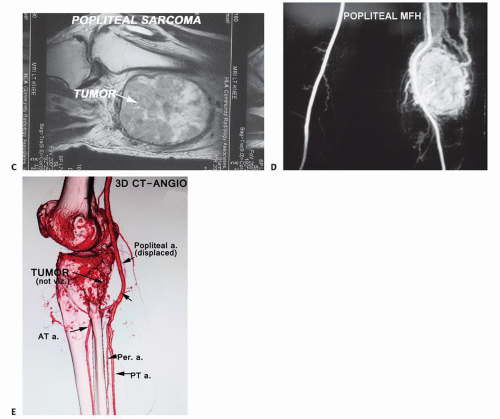
FIG 1 • (continued) C. Sagittal view showing the relationship of a popliteal sarcoma to the adjacent femur and knee joint (not involved in this case). D. Angiogram of an extremely vascular popliteal sarcoma. Arterial embolization may be useful. All of the small pedicles to the tumor must be ligated at the time of resection. The popliteal artery is rarely involved directly and is often preserved. E. CT angiogram demonstrating displacement of the popliteal artery.
The tibial nerve enters the popliteal fossa lateral to the popliteal artery and approximately in the middle of the fossa. It crosses the artery to its medial aspect and remains at that location. The common peroneal nerve slopes down the superolateral border of the popliteal fossa toward the medial aspect and along the biceps femoris tendon, where it enters a tunnel within the substance of the peroneus longus muscle.
IMAGING AND OTHER STAGING STUDIES
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is the imaging modality of choice for the diagnosis of popliteal soft tissue sarcomas. The typical finding is a soft tissue mass with a solid component, no communication to the knee, and central or irregular nodular gadolinium enhancement. Conversely, the classic presentation on MRI of popliteal cysts, which are the most frequently encountered masses in the popliteal fossa, is a well-defined, unilocular, fluid-filled cyst in direct communication with the knee joint; its peripheral walls are normally enhanced with gadolinium.
MRI is also used to evaluate the size of the tumor and its relation to the neurovascular structures, the posterior knee joint capsule, and surrounding musculature and to assess local lymph node involvement (FIG 1A-C).
Plain Radiography and Computed Tomography
Plain radiography and computed tomography (CT) scans are performed to rule out invasion of the tumor into the adjacent bones.
Angiography
Angiography (FIG 1D-E) is routinely used to assess the relation of the tumor to the popliteal artery, patterns of possible vascular displacement, the presence of vascular anomalies, and arterial and venous patency.
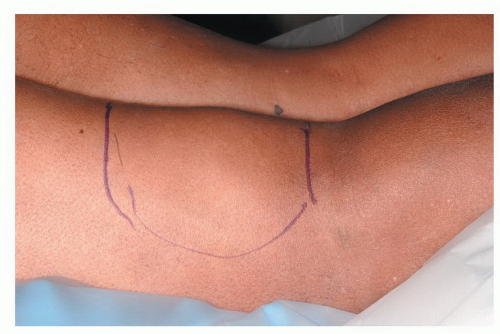 FIG 2 • Clinical photograph of a large popliteal sarcoma. A prone position is routinely used for surgical resection. |
SURGICAL MANAGEMENT
Positioning
The patient is placed in the prone position (FIG 2) and both lower limbs are draped.
The contralateral leg is prepared for saphenous vein harvesting, which will be necessary for arterial reconstruction if the popliteal artery must be resected.
TECHNIQUES
▪ Exposure
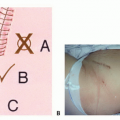
An S-shaped incision is made, crossing from proximal-medial to distal-lateral at the level of the knee joint (TECH FIG 1A). The medial-proximal arm of the incision allows the popliteal vessels to be identified as they exit the adductor hiatus, and the lateral distal arm enables easy exposure of the peroneal nerve, posterior to the fibular head. In addition, making the distal arm of the incision lateral avoids damaging the greater saphenous vein, which runs on the medial aspect of the leg (TECH FIG 1B).Related posts:
 Biopsy of Musculoskeletal Tumors
Biopsy of Musculoskeletal Tumors
 Overview of Resections around the Shoulder Girdle
Overview of Resections around the Shoulder Girdle
 Primary and Metastatic Tumors of the Spine: Total En Bloc Spondylectomy
Primary and Metastatic Tumors of the Spine: Total En Bloc Spondylectomy
 Surgical Management of Metastatic Bone Disease: Pelvic Lesions
Surgical Management of Metastatic Bone Disease: Pelvic Lesions
 Adductor Muscle Group (Medial Thigh) Resection
Adductor Muscle Group (Medial Thigh) Resection
 Distal Femoral Resections with Endoprosthetic Replacement
Distal Femoral Resections with Endoprosthetic Replacement

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


